Systemic Vascular Resistance (SVR) is a crucial physiological parameter that describes the opposition to blood flow within the systemic circulation. In simpler terms, it quantifies how constricted or dilated the blood vessels are, dictating the amount of pressure the heart must generate to pump blood effectively throughout the body. Understanding SVR is fundamental to comprehending cardiovascular health, disease states, and the mechanisms of various pharmacological interventions. This article delves into the intricate nature of SVR, exploring its determinants, its measurement, and its significance in clinical practice.
Understanding the Pillars of SVR
Systemic Vascular Resistance is not a monolithic entity but rather a complex interplay of several factors. At its core, SVR is determined by the properties of the blood vessels and the characteristics of the blood itself.
Vessel Diameter: The Primary Determinant
The most significant factor influencing SVR is the diameter of the systemic arteries and arterioles. According to Poiseuille’s Law, resistance to fluid flow is inversely proportional to the fourth power of the radius. This means that even a small change in the diameter of a blood vessel can have a profound impact on resistance.
- Arterioles: These are the smallest arteries and are considered the primary regulators of SVR. Their muscular walls allow for significant vasoconstriction (narrowing) and vasodilation (widening), enabling the body to precisely control blood flow distribution and overall vascular resistance. When arterioles constrict, SVR increases, leading to higher blood pressure. Conversely, vasodilation decreases SVR and lowers blood pressure.
- Arteries: Larger arteries, while less capable of rapid diameter changes, also contribute to resistance. Their elasticity plays a role in dampening the pulsatile flow from the heart and maintaining blood pressure during diastole. However, their contribution to the dynamic regulation of SVR is less pronounced than that of the arterioles.
- Veins: While veins have a larger total diameter than arteries, their walls are thinner and less muscular. They are considered capacitance vessels, holding a significant portion of the body’s blood volume. Their contribution to resistance is much lower than arteries and arterioles, but their tone can influence venous return to the heart, indirectly affecting cardiac output.
Blood Viscosity: The Internal Friction
The viscosity of blood, its “thickness” or resistance to flow, also contributes to SVR. Factors that increase blood viscosity, such as dehydration, polycythemia (an excess of red blood cells), or high levels of plasma proteins, will increase SVR. Conversely, conditions that decrease blood viscosity, like anemia, can reduce SVR. However, blood viscosity is generally a less significant determinant of acute changes in SVR compared to vessel diameter.
Blood Volume: The Driving Force
While not a direct component of the SVR calculation, blood volume is intrinsically linked. A larger blood volume generally leads to higher cardiac output and can contribute to increased SVR if the vascular network cannot adequately accommodate the increased volume. Conversely, a decrease in blood volume (e.g., due to hemorrhage) will reduce cardiac output and blood pressure, often accompanied by compensatory mechanisms that may temporarily increase SVR to maintain perfusion.
Calculating and Measuring SVR
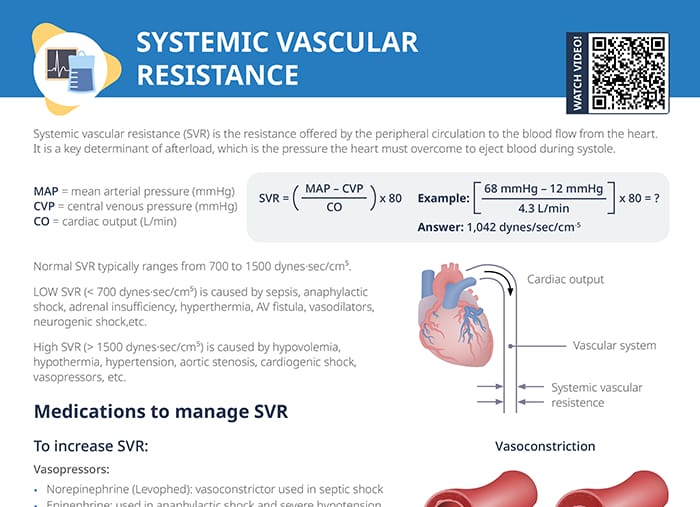
SVR is not directly measured but is rather calculated using a derived formula based on other measurable hemodynamic parameters. The standard formula for calculating SVR is:
SVR = (Mean Arterial Pressure – Central Venous Pressure) / Cardiac Output
Let’s break down the components of this formula:
- Mean Arterial Pressure (MAP): This represents the average arterial pressure throughout one cardiac cycle. It is the primary driving pressure for blood flow. MAP can be estimated using the formula: MAP ≈ Diastolic Blood Pressure + 1/3 (Systolic Blood Pressure – Diastolic Blood Pressure). More precise measurement requires invasive arterial catheterization.
- Central Venous Pressure (CVP): This is the pressure in the thoracic vena cava, near the right atrium. It reflects the filling pressure of the right side of the heart and is generally considered the pressure to which blood flows in the systemic circulation. CVP is typically measured using a central venous catheter.
- Cardiac Output (CO): This is the volume of blood pumped by the heart per minute. It is the product of stroke volume (the amount of blood ejected by the left ventricle per beat) and heart rate. CO can be measured non-invasively using techniques like echocardiography or thermodilution, or invasively via a pulmonary artery catheter.
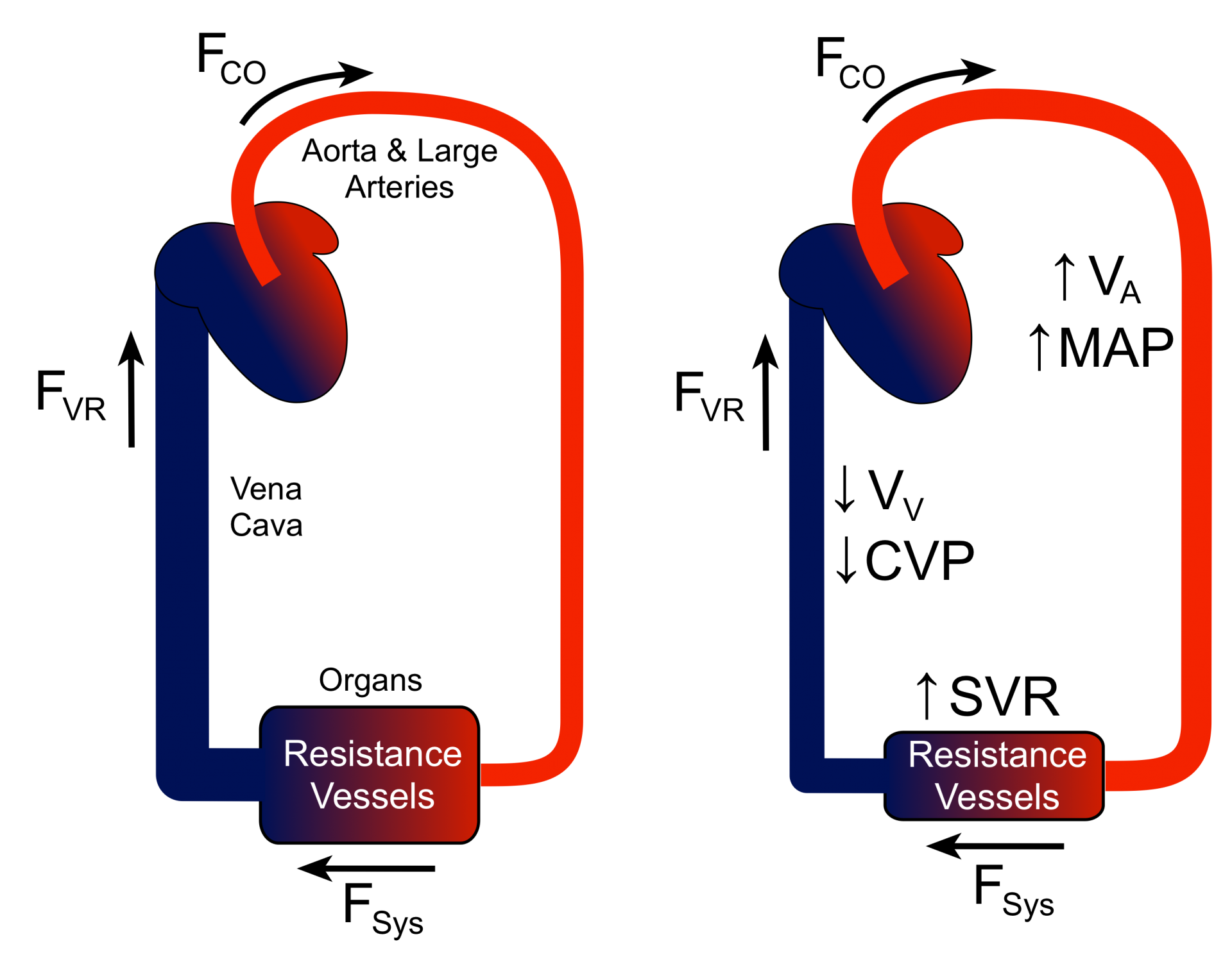
The formula highlights that as MAP increases (while CVP and CO remain constant), SVR increases. Conversely, if CO increases (while MAP and CVP remain constant), SVR decreases, as the heart is pumping more blood through the same vascular resistance. The subtraction of CVP from MAP accounts for the pressure gradient that drives blood flow through the systemic circuit, acknowledging that the “resistance” is relative to the pressure at the point of venous return.
Clinical Methods of SVR Assessment
While the formula provides a theoretical basis, in clinical settings, SVR is typically calculated by hemodynamic monitoring systems. These systems continuously or intermittently acquire the necessary data (MAP, CVP, and CO) and display the calculated SVR value.
- Invasive Hemodynamic Monitoring: This is the gold standard for accurate SVR assessment and is commonly employed in intensive care units (ICUs) and operating rooms. It involves inserting catheters into arteries (e.g., radial artery) to measure blood pressure continuously and into large veins (e.g., internal jugular vein) or the pulmonary artery to measure CVP and CO.
- Non-Invasive Methods: While less precise for direct SVR calculation, non-invasive methods like echocardiography can provide estimates of cardiac output and inferences about vascular tone. Blood pressure cuffs provide systemic blood pressure, which, combined with estimates of CVP and CO, can lead to less accurate SVR estimations.
The Significance of SVR in Health and Disease
SVR plays a critical role in maintaining adequate tissue perfusion and organ function. Its dynamic regulation is essential for adapting to changing physiological demands.
Physiological Regulation of SVR
The body employs sophisticated mechanisms to control SVR, primarily through the autonomic nervous system and hormonal influences.
- Autonomic Nervous System: The sympathetic nervous system exerts a powerful influence on vascular tone. Activation of sympathetic nerves releases norepinephrine, which binds to alpha-adrenergic receptors on vascular smooth muscle, causing vasoconstriction and increasing SVR. Conversely, parasympathetic activity has a less pronounced direct effect on systemic arteries.
- Hormonal Control: Several hormones can affect SVR.
- Angiotensin II: A potent vasoconstrictor that significantly increases SVR. It is a key component of the renin-angiotensin-aldosterone system (RAAS), which plays a crucial role in blood pressure regulation.
- Vasopressin (Antidiuretic Hormone – ADH): Can cause vasoconstriction at higher concentrations, increasing SVR.
- Norepinephrine and Epinephrine (Adrenaline): Released during stress, these hormones cause widespread vasoconstriction by stimulating alpha-adrenergic receptors, thus increasing SVR.
- Nitric Oxide (NO): A potent vasodilator produced by endothelial cells. It promotes relaxation of vascular smooth muscle, decreasing SVR. Its production and release are influenced by factors like shear stress and various signaling pathways.
- Endothelin: A potent vasoconstrictor that can increase SVR.
SVR in Cardiovascular Disease
Abnormalities in SVR are central to many cardiovascular pathologies.
- Hypertension: Chronically elevated SVR is a hallmark of essential hypertension. The persistent narrowing of blood vessels requires the heart to work harder, leading to increased workload and potential damage to the heart and other organs over time.
- Heart Failure: In heart failure, the heart’s pumping function is compromised. If SVR is high, the failing heart has to pump against increased resistance, further exacerbating its inefficiency. Therapies for heart failure often aim to reduce SVR to ease the heart’s workload.
- Septic Shock: This life-threatening condition involves widespread inflammation and infection, leading to a profound drop in SVR (vasodilation). This results in a drastic decrease in blood pressure and inadequate tissue perfusion, despite a potentially compensatory increase in cardiac output.
- Aortic Stenosis: Narrowing of the aortic valve increases the resistance to left ventricular ejection, but the primary issue here is afterload at the valve itself, not necessarily a systemic increase in SVR. However, the compensatory mechanisms to maintain cardiac output can indirectly influence SVR.
- Pulmonary Hypertension: This condition affects the pulmonary circulation, which has its own resistance (Pulmonary Vascular Resistance – PVR). While distinct from SVR, understanding the principles of resistance in one vascular bed informs the understanding of the other.
Pharmacological Impact on SVR
Many medications used to treat cardiovascular conditions directly target SVR.
- Vasodilators: Drugs like ACE inhibitors, angiotensin II receptor blockers (ARBs), calcium channel blockers, and nitrates work by widening blood vessels, thus decreasing SVR and lowering blood pressure. This is particularly beneficial in hypertension and heart failure.
- Vasoconstrictors: In certain critical care situations, such as septic shock, vasopressors like norepinephrine are used to constrict blood vessels and increase SVR, thereby raising blood pressure and improving organ perfusion.
- Diuretics: While primarily acting to reduce blood volume, diuretics can indirectly affect SVR by reducing preload and afterload.
In conclusion, Systemic Vascular Resistance is a dynamic and vital physiological indicator. Its intricate regulation, determined by vessel diameter, viscosity, and influenced by numerous neural and hormonal factors, ensures adequate blood flow to all tissues. Understanding SVR is paramount for diagnosing and managing a wide spectrum of cardiovascular diseases and for appreciating the mechanisms of therapeutic interventions aimed at optimizing circulatory function.