Pleurodynia, a term often encountered in medical contexts, refers to a sharp, stabbing pain that occurs in the chest wall, typically on one side. While not a diagnosis in itself, it is a symptom that signals an underlying condition requiring careful evaluation. Understanding the causes, characteristics, and potential implications of pleurodynia is crucial for both medical professionals and individuals experiencing this discomfort. This article delves into the nature of pleurodynia, exploring its common etiologies, diagnostic approaches, and management strategies, all within the framework of understanding the body’s intricate systems.
Understanding the Chest Wall and its Pain Pathways
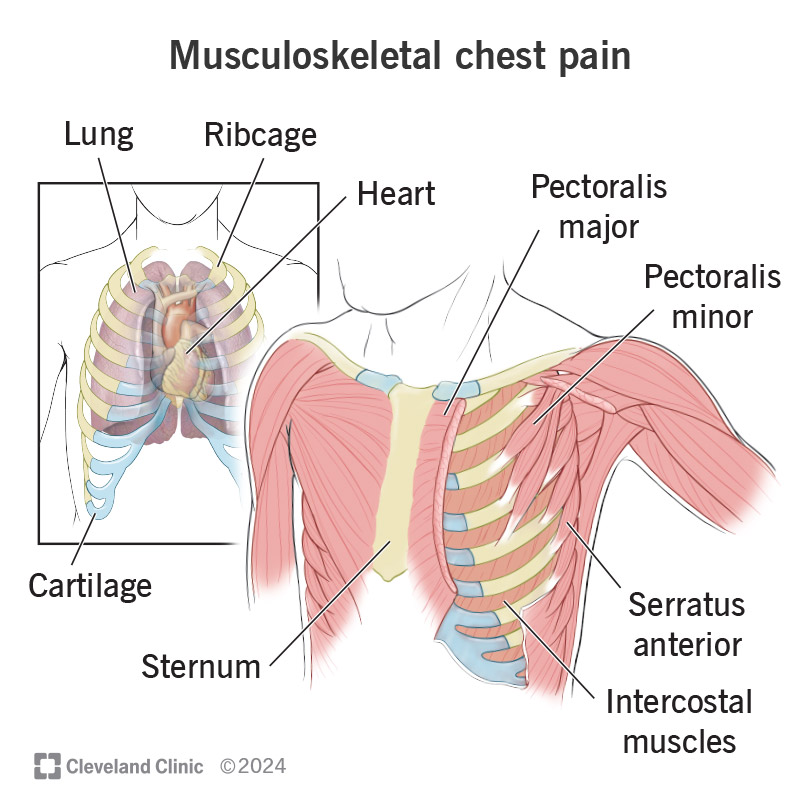
The chest wall is a complex structure composed of bone, muscle, cartilage, and nerves, all working in concert to protect vital organs like the heart and lungs and to facilitate respiration. Pain originating from this region can be notoriously difficult to pinpoint due to the interwoven nature of these components and the extensive nerve pathways that transmit sensory information to the brain.

Anatomical Structures Involved in Chest Pain
- Ribs and Intercostal Muscles: The ribs, a series of curved bones, form a protective cage. Between each rib are the intercostal muscles, which play a vital role in breathing. Strains, inflammation, or direct injury to these muscles can lead to significant pain.
- Pleura: The pleura are two thin membranes that line the chest cavity and surround the lungs. The visceral pleura covers the surface of the lungs, while the parietal pleura lines the inner surface of the chest wall, diaphragm, and mediastinum. The space between these two layers, the pleural space, normally contains a small amount of lubricating fluid. Inflammation of the pleura, known as pleurisy or pleuritis, is a common cause of sharp chest pain, often exacerbated by breathing.
- Nerves of the Thoracic Wall: A network of nerves, including the intercostal nerves, supply the chest wall. Irritation, compression, or inflammation of these nerves can result in sharp, localized pain that may radiate.
- Diaphragm: This large, dome-shaped muscle at the base of the chest cavity is essential for breathing. Problems with the diaphragm, such as irritation or spasm, can also manifest as chest pain.
The Sensory Experience of Pleurodynia
Pleurodynia is characterized by its acute and often intense nature. Patients frequently describe it as:
- Sharp and Stabbing: A sudden, piercing sensation rather than a dull ache.
- Localized: Typically felt on one side of the chest, though it can occasionally occur on both.
- Exacerbated by Respiration: Deep breaths, coughing, sneezing, or even movement can significantly worsen the pain, a hallmark of pleural or musculoskeletal involvement.
- Referred Pain: In some instances, the pain may radiate to other areas, such as the shoulder, abdomen, or back, making the diagnosis more challenging.
Common Causes of Pleurodynia
The etiologies of pleurodynia are diverse, ranging from infectious agents to musculoskeletal issues and inflammatory conditions. A thorough medical history, physical examination, and targeted investigations are essential for accurate diagnosis.
Infectious Etiologies
Infections are a significant cause of pleurodynia, particularly those affecting the respiratory system.
Viral Infections
- Coxsackievirus B: This group of enteroviruses is a common culprit behind pleurodynia, often referred to as “epidemic pleurodynia” or “Bornholm disease.” It typically presents with sudden onset of fever, headache, and severe chest pain. The pain is often pleuritic, meaning it worsens with breathing.
- Influenza and other Respiratory Viruses: While not exclusively causing pleurodynia, other viral infections affecting the respiratory tract, such as influenza, parainfluenza, and adenoviruses, can lead to inflammation of the pleura or intercostal muscles, resulting in chest pain.
Bacterial Infections
- Pneumonia: Inflammation of the lung tissue, often caused by bacteria, can lead to pleuritic chest pain if the infection extends to the pleura. This is known as parapneumonic pleurisy.
- Tuberculosis (TB): While primarily known for affecting the lungs, TB can also involve the pleura, causing pleurisy and associated pain.
- Bacterial Pleurisy: Direct bacterial infection of the pleural space, often as a complication of pneumonia or chest trauma, can cause severe pleurodynia.
Musculoskeletal Causes
The robust musculature of the chest wall is susceptible to injury and inflammation.
- Intercostal Muscle Strain: Overexertion, sudden movements, or forceful coughing can lead to strains or tears in the intercostal muscles, causing sharp, localized pain that is often reproduced by palpation or specific movements.
- Rib Fractures: Traumatic injury to the ribs, even hairline fractures, can result in significant pain, particularly with breathing, coughing, and palpation.
- Costochondritis: This is a condition characterized by inflammation of the cartilage that connects the ribs to the breastbone (sternum). It can cause sharp chest pain that is often mistaken for cardiac pain, though it is typically reproducible with palpation over the affected area.
- Fibromyalgia: In individuals with fibromyalgia, widespread musculoskeletal pain can include the chest wall, leading to pleurodynia-like symptoms.
Inflammatory and Autoimmune Conditions
Certain systemic inflammatory conditions can affect the pleura.
- Rheumatoid Arthritis: While primarily affecting joints, rheumatoid arthritis can sometimes involve the pleura, leading to pleurisy and pleurodynia.
- Lupus Erythematosus (SLE): Systemic lupus erythematosus is an autoimmune disease that can cause inflammation in various organs, including the pleura.
- Vasculitis: Inflammation of blood vessels can affect the pleura, leading to pleuritic chest pain.

Other Causes
- Pulmonary Embolism (PE): While not a direct cause of pleurodynia in the classic sense, a pulmonary embolism, a blood clot in the lung, can cause pleuritic chest pain due to inflammation of the pleura as the clot irritates the lung surface. This is a medical emergency.
- Pneumothorax: A collapsed lung, where air enters the pleural space, can cause sudden, sharp chest pain and shortness of breath.
- Herpes Zoster (Shingles): Before the characteristic rash appears, shingles can cause burning or stabbing pain in the chest area supplied by the affected nerve, mimicking pleurodynia.
- Gastrointestinal Issues: While less common, conditions like esophageal spasm or peptic ulcer disease can sometimes refer pain to the chest, and in rare instances, may be perceived as pleurodynia.
Diagnosis and Evaluation of Pleurodynia
The diagnostic process for pleurodynia aims to identify the underlying cause and rule out more serious conditions, especially those affecting the heart and lungs.
Medical History and Physical Examination
The cornerstone of diagnosis is a detailed patient history. Key questions include:
- Onset and Duration: When did the pain start? How long does it last?
- Character of Pain: Sharp, dull, burning, aching?
- Location and Radiation: Where is the pain most intense? Does it move to other areas?
- Aggravating and Alleviating Factors: What makes the pain worse (breathing, movement, position)? What makes it better?
- Associated Symptoms: Fever, cough, shortness of breath, nausea, rash, recent illness, or injury?
- Past Medical History: Pre-existing conditions, medications, recent travel.
The physical examination will focus on:
- Vital Signs: Temperature, heart rate, respiratory rate, blood pressure, oxygen saturation.
- Cardiovascular and Pulmonary Auscultation: Listening to heart and lung sounds for any abnormalities like crackles, wheezes, or pleural rub.
- Palpation of the Chest Wall: To identify areas of tenderness, which can suggest musculoskeletal causes like costochondritis or muscle strain.
- Assessment of Range of Motion: Evaluating how movement affects the pain.
Diagnostic Investigations
Based on the initial assessment, further investigations may be ordered:
- Chest X-ray (CXR): A fundamental imaging tool that can help identify pneumonia, pleural effusions (fluid in the pleural space), pneumothorax, and rib fractures.
- Electrocardiogram (ECG): Essential to rule out cardiac causes of chest pain, such as myocardial infarction (heart attack) or pericarditis.
- Blood Tests:
- Complete Blood Count (CBC): To detect signs of infection or inflammation.
- Inflammatory Markers (e.g., C-reactive protein (CRP), Erythrocyte Sedimentation Rate (ESR)): To assess for systemic inflammation.
- D-dimer: If pulmonary embolism is suspected.
- Viral Serology: To identify specific viral infections if suspected.
- Computed Tomography (CT) Scan: May be used for more detailed imaging of the lungs, pleura, or chest wall if the CXR is inconclusive or if a PE is strongly suspected (CT pulmonary angiography).
- Ultrasound: Can be useful for evaluating the pleura, detecting effusions, or examining musculoskeletal structures.
- Sputum Culture: If pneumonia or other respiratory infections are suspected.
- Pleural Fluid Analysis: If a significant pleural effusion is present, the fluid may be drained and analyzed to determine the cause (e.g., infection, inflammation, malignancy).
Management and Treatment of Pleurodynia
The treatment of pleurodynia is directed at the underlying cause. Once the etiology is identified, a tailored approach can be implemented.
Symptomatic Relief
Regardless of the underlying cause, managing the pain is a priority.
- Analgesics: Over-the-counter pain relievers like acetaminophen (Tylenol) or nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Advil, Motrin) or naproxen (Aleve) are often effective for mild to moderate pain. NSAIDs also help reduce inflammation.
- Prescription Pain Medications: For severe pain, stronger analgesics, including opioids, may be prescribed for short-term use.
- Rest: Avoiding activities that exacerbate the pain, such as strenuous exercise or deep breathing, can aid in recovery.
- Heat or Cold Therapy: Applying heat or cold packs to the affected area may provide some relief for musculoskeletal pain.
Specific Treatments Based on Etiology
- Viral Infections: Treatment is primarily supportive, focusing on pain relief and managing fever. Antiviral medications are generally not effective for Coxsackievirus B infections causing pleurodynia.
- Bacterial Infections: Antibiotics are crucial for treating bacterial pneumonia, pleurisy, or other bacterial infections. The choice of antibiotic depends on the identified bacteria.
- Musculoskeletal Causes:
- Muscle Strain: Rest, physical therapy, and stretching exercises are key.
- Costochondritis: NSAIDs, rest, and sometimes local corticosteroid injections may be used.
- Rib Fractures: Pain management, breathing exercises to prevent complications like pneumonia, and sometimes bracing for severe fractures.
- Inflammatory Conditions: Treatment involves managing the underlying autoimmune disease with immunosuppressive medications or biologics as prescribed by a rheumatologist.
- Pulmonary Embolism: Anticoagulant medications (blood thinners) are the primary treatment to prevent clot formation and extension. In severe cases, thrombolytic therapy (clot-busting drugs) or surgical removal of the clot may be considered.
- Pneumothorax: Depending on the size of the pneumothorax, treatment can range from observation to insertion of a chest tube to remove air from the pleural space.
When to Seek Medical Attention
While many cases of pleurodynia are benign and resolve on their own, it is important to seek medical attention if:
- The pain is severe or sudden in onset.
- The pain is accompanied by shortness of breath, dizziness, or fainting.
- There is a fever, persistent cough, or production of colored sputum.
- The pain is associated with a known risk factor for heart disease or pulmonary embolism.
- The pain does not improve with over-the-counter pain relief or persists for more than a few days.
Understanding pleurodynia is essential for navigating the complexities of chest pain and ensuring appropriate medical care. By recognizing its diverse origins and characteristics, individuals and healthcare providers can work together to achieve accurate diagnoses and effective management strategies, ultimately restoring comfort and well-being.