The oral mucosa refers to the moist lining of the entire oral cavity, serving as a critical barrier and interface between the external environment and the internal systems of the body. Far more than just a simple lining, this complex tissue performs a multitude of essential functions, from protection against mechanical trauma and microbial invasion to sensory perception and selective absorption. Understanding its intricate structure, diverse types, and dynamic health status is paramount not only for dental and medical professionals but also for anyone seeking a comprehensive grasp of oral health. Its unique properties and responses to various stimuli also make it a fascinating subject for advanced diagnostic and imaging technologies.
The Fundamental Structure of Oral Mucosa
At its core, oral mucosa is a mucous membrane composed of two primary layers: a stratified squamous epithelium and an underlying connective tissue layer known as the lamina propria. These layers are intricately interdigitated by a basement membrane, which plays a crucial role in cellular adhesion, communication, and overall tissue integrity.
Stratified Squamous Epithelium
The epithelial layer is the outermost component, directly exposed to the oral environment. It is typically non-keratinized or parakeratinized in most areas, meaning its superficial cells retain their nuclei, unlike the heavily keratinized epithelium of the skin. This characteristic allows the oral mucosa to remain soft, flexible, and moist, essential for functions like speech, mastication, and taste. The epithelium is a dynamic tissue, constantly undergoing renewal through cell division in its basal layer, with cells migrating upwards and eventually desquamating (shedding) from the surface. This rapid turnover is a vital protective mechanism, allowing the tissue to quickly replace damaged cells and shed microorganisms. Specialized cells within the epithelium include melanocytes (producing pigment), Merkel cells (mechanoreceptors), and Langerhans cells (immune cells), each contributing to the diverse functions of the oral lining. The thickness and degree of keratinization can vary significantly depending on the specific location within the oral cavity, reflecting different functional demands.
Lamina Propria and Submucosa
Beneath the epithelium lies the lamina propria, a layer of dense fibrous connective tissue rich in collagen and elastic fibers. This layer provides structural support and anchors the epithelium, while also housing blood vessels, lymphatic vessels, nerves, and various immune cells (such as fibroblasts, macrophages, and mast cells). The rich vascular supply within the lamina propria is crucial for nourishing the overlying epithelium and facilitating the rapid inflammatory responses often observed in the oral cavity. In many regions of the oral cavity, an additional deeper layer called the submucosa is present. The submucosa consists of looser connective tissue and may contain glands (salivary glands), fat cells, and larger neurovascular bundles. Its presence or absence, and the density of its contents, dictates the mobility of the overlying mucosa. For instance, in areas like the cheeks and floor of the mouth, a thick, loose submucosa allows for considerable movement, whereas in regions firmly bound to bone, like the gingiva and hard palate, the submucosa is absent or minimal, resulting in firmly attached mucosa.
Diverse Types and Specialized Functions
The oral mucosa is not a monolithic tissue; rather, it is broadly categorized into three main types, each with distinct histological features and functional adaptations tailored to their specific locations within the mouth.
Masticatory Mucosa
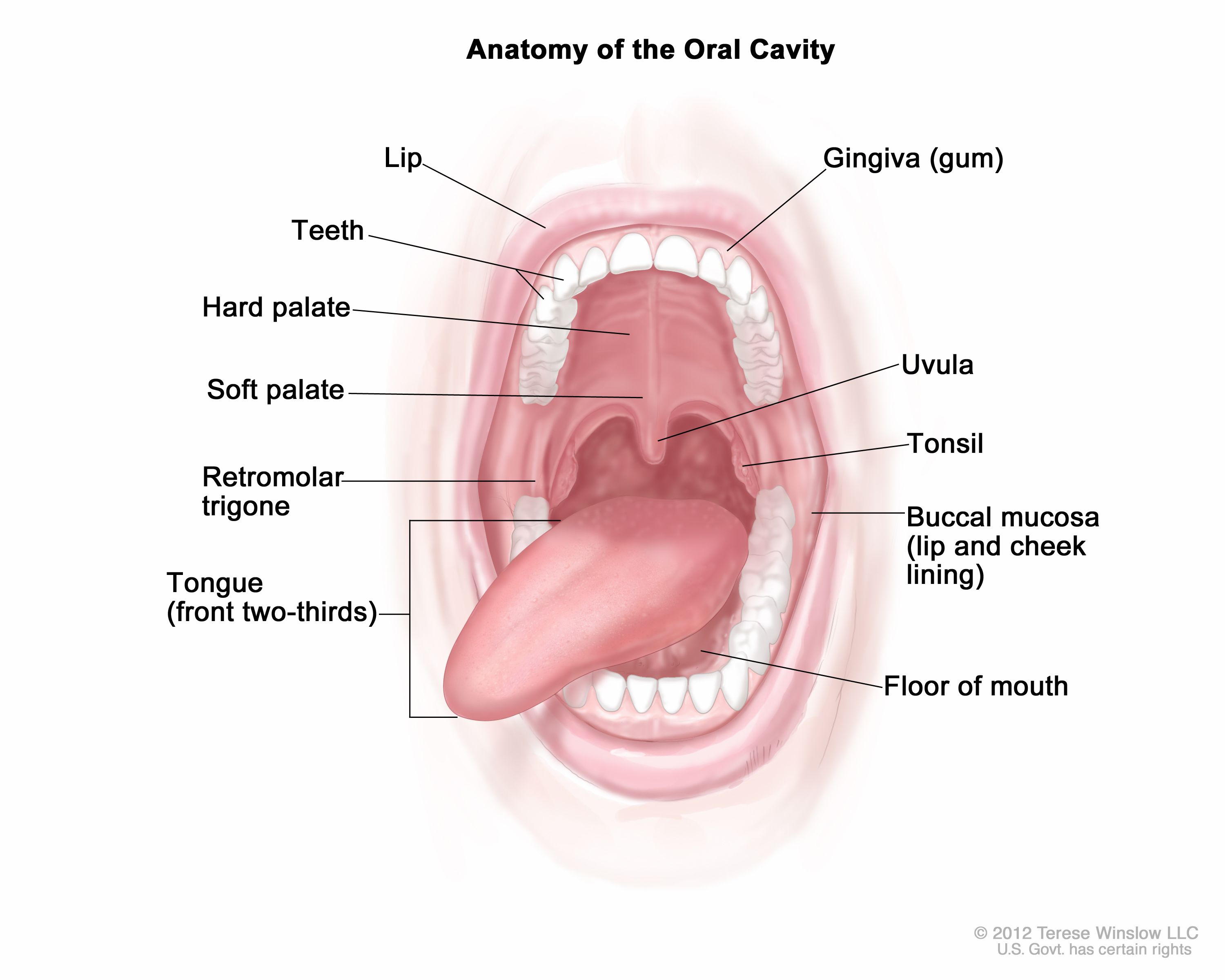
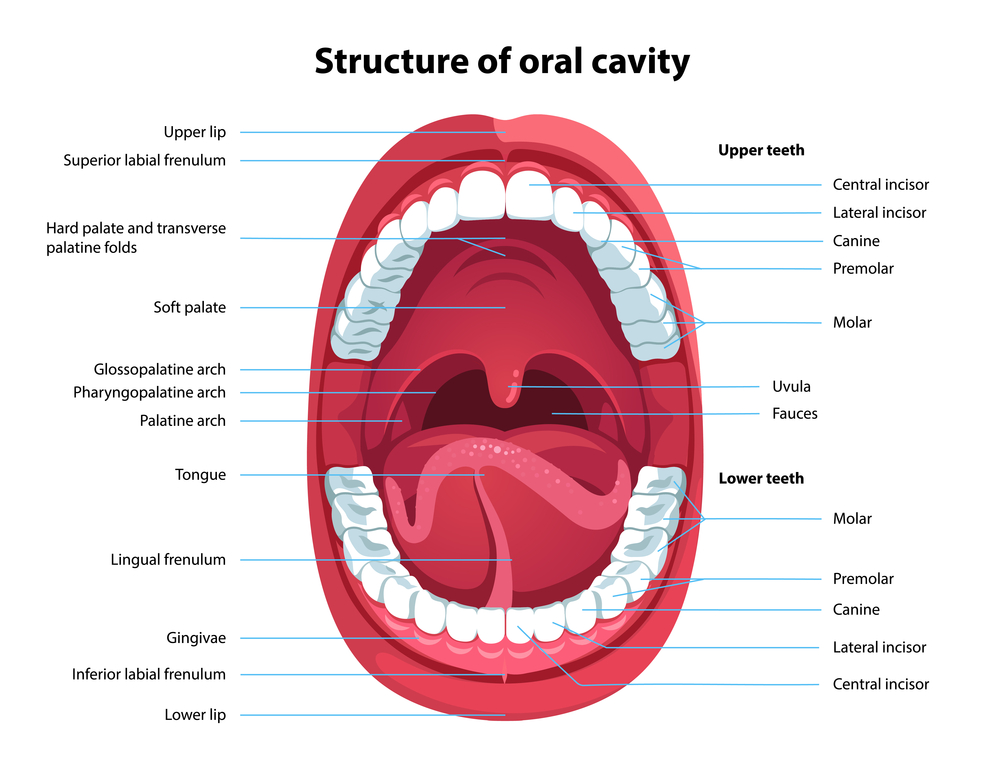
Found in areas subjected to significant friction and pressure during chewing, such as the gingiva (gums) and the hard palate, masticatory mucosa is robust and often keratinized or parakeratinized. Its epithelium is thicker and features prominent epithelial ridges (rete ridges) that interlock firmly with the connective tissue papillae of the lamina propria, enhancing its resistance to mechanical stress. The lamina propria in these regions is typically dense and directly attached to the underlying bone, limiting mobility. This firm attachment and resilient surface are essential for withstanding the forces of mastication, preventing tissue damage, and maintaining the stability of teeth. Clinically, the color of healthy masticatory mucosa is typically pale pink, reflecting the dense connective tissue and limited vascularity near the surface, though melanin pigmentation can vary widely among individuals.
Lining Mucosa
Covering the vast majority of the oral cavity, including the labial (lips), buccal (cheeks), alveolar (overlying alveolar bone), soft palate, sublingual (underside of the tongue), and floor of the mouth, lining mucosa is characterized by its non-keratinized, thinner epithelium. It is soft, pliable, and highly movable, an adaptation facilitated by the presence of a well-developed, loose submucosa containing numerous elastic fibers, minor salivary glands, and adipose tissue. This mobility is critical for allowing the extensive movements required for speech, swallowing, and facial expressions. The rich vascular supply in its lamina propria gives lining mucosa a characteristic reddish-pink appearance. Its delicate nature also makes it more susceptible to minor trauma, though its rapid healing capacity is also a notable feature.
Specialized Mucosa
This unique type of mucosa is found exclusively on the dorsal surface of the tongue and is distinguished by the presence of numerous papillae. These papillae are epithelial projections, some of which house taste buds, making this mucosa specialized for sensory perception. The four main types of lingual papillae are:
- Filiform papillae: The most numerous, cone-shaped, and covered with keratinized epithelium. They provide a rough surface for mechanical grip on food and do not contain taste buds. Their keratinized tips are important for tactile sensation.
- Fungiform papillae: Mushroom-shaped, scattered among the filiform papillae, appearing as red dots. They have a thinner, non-keratinized epithelium and usually contain taste buds on their dorsal surface. Their rich vascular core gives them their reddish hue, easily discernible upon visual inspection.
- Circumvallate papillae: Large, flat-topped papillae surrounded by a trench, typically 8-12 in number, located in a V-shape near the back of the tongue. Their lateral walls contain numerous taste buds, and serous glands of von Ebner empty into the trench, aiding in taste perception by flushing food particles.
- Foliate papillae: Leaf-like folds located on the lateral borders of the posterior tongue. They contain taste buds primarily in infancy and childhood.
The specialized mucosa’s varied texture and color across these papillae are often key visual indicators in clinical examinations.
Oral Mucosa in Health and Disease
A healthy oral mucosa presents a uniformly pink, moist, and smooth surface, though color can vary with ethnicity (due to melanin pigmentation) and location (e.g., darker on the soft palate, lighter on the gingiva). Its integrity is a crucial component of overall health, as it acts as the first line of defense against pathogens, irritants, and mechanical forces. Saliva constantly bathes the oral mucosa, providing lubrication, cleansing, and antimicrobial properties that support its barrier function.
However, the oral mucosa is also highly susceptible to a wide range of pathological conditions, including infections (bacterial, viral, fungal), inflammatory disorders (e.g., lichen planus, aphthous ulcers), systemic diseases with oral manifestations (e.g., Crohn’s disease, vitamin deficiencies), and neoplastic changes (pre-cancerous lesions and oral cancer). Changes in color (redness, pallor, white patches), texture (roughness, ulceration, swelling), and consistency (hardness, softness) are often the earliest clinical signs of disease. Early detection of these changes is critical for effective diagnosis and treatment. For instance, persistent white patches (leukoplakia) or red patches (erythroplakia) warrant immediate investigation due to their potential for malignant transformation.
Advanced Imaging Perspectives on Oral Mucosa
The visual accessibility of the oral mucosa makes it an ideal target for various imaging techniques, both traditional and cutting-edge. Beyond direct visual inspection, which relies on ambient light and trained clinical eyes, advanced imaging plays an increasingly vital role in characterizing, diagnosing, and monitoring the health and disease states of this complex tissue.
Optical and Digital Imaging
High-resolution digital cameras, often integrated into intraoral scanners or specialized microscopes, are fundamental tools. They capture precise details of surface morphology, color variations, and textural changes that might be subtle to the naked eye. Digital images provide objective records, allowing for comparative analysis over time, crucial for monitoring lesion progression or response to treatment. Image processing software can enhance contrast, measure lesion dimensions, and even analyze color profiles to identify early signs of inflammation or dysplasia. Polarization filters can be used to reduce glare and reveal deeper tissue structures.
Fluorescence Imaging
Autofluorescence imaging, utilizing specific wavelengths of light, can detect changes in the metabolic activity of oral mucosal cells. Healthy tissue emits a characteristic green fluorescence due to endogenous fluorophores (like collagen and flavins). Dysplastic or malignant tissue often exhibits a loss of this autofluorescence (appears dark), a phenomenon that can aid in the early detection of potentially cancerous lesions not yet visible under white light. Devices like VELscope or Identafi leverage this principle, providing a non-invasive adjunct to traditional oral cancer screenings. This technique essentially “lights up” metabolic differences, making them detectable by specialized cameras.
Confocal Microscopy and Optical Coherence Tomography (OCT)
For non-invasive, real-time visualization of cellular and architectural features in vivo, confocal microscopy and Optical Coherence Tomography (OCT) offer unparalleled insights. Confocal microscopy uses focused light and a pinhole to achieve high-resolution imaging of thin optical sections, akin to a “virtual biopsy.” It can reveal cellular morphology, nuclear characteristics, and the integrity of the epithelial-connective tissue junction without needing to remove tissue. OCT, on the other hand, utilizes light waves to create cross-sectional images of biological tissues up to several millimeters deep, providing detailed architectural information about the epithelial thickness, the basement membrane zone, and the underlying lamina propria and submucosa. Both techniques are invaluable for studying micro-structural changes associated with various oral diseases and for guiding biopsy decisions, essentially providing high-definition “scans” of the mucosal layers.

Hyperspectral Imaging
Emerging technologies like hyperspectral imaging, which captures images across a wide range of the electromagnetic spectrum, offer even more detailed biochemical information. By analyzing the unique spectral signatures of different tissue components, hyperspectral cameras can detect subtle changes in tissue oxygenation, blood flow, and the distribution of specific molecules indicative of disease, long before macroscopic changes become apparent. This multi-spectral data can be processed to create “maps” of various tissue properties, providing a powerful, non-invasive diagnostic tool that could potentially detect precancerous changes at a very early stage, leveraging advanced sensor arrays to differentiate between healthy and pathological states based on their unique light absorption and reflection profiles.
The continuous evolution of imaging technologies offers increasingly sophisticated methods to probe the complexities of the oral mucosa. These advancements empower clinicians with enhanced diagnostic capabilities, enabling earlier intervention, more precise treatment planning, and ultimately, improved patient outcomes in oral health care.