Graves’ disease is a complex autoimmune disorder that primarily affects the thyroid gland, leading to a condition known as hyperthyroidism. Unlike other forms of hyperthyroidism, Graves’ disease is specifically characterized by the body’s own immune system mistakenly attacking the thyroid gland. This attack stimulates the thyroid to produce an excessive amount of thyroid hormones, specifically thyroxine (T4) and triiodothyronine (T3), disrupting the delicate balance of metabolism in the body. Understanding Graves’ disease requires delving into its autoimmune origins, the resulting hormonal imbalance, and the diverse range of symptoms it can manifest.
The Autoimmune Assault on the Thyroid
At its core, Graves’ disease is an autoimmune condition. In a healthy immune response, the body produces antibodies to defend against foreign invaders like bacteria and viruses. However, in Graves’ disease, the immune system malfunctions and generates antibodies that target specific components of the thyroid gland. The primary culprit is a type of antibody known as thyroid-stimulating immunoglobulin (TSI). These TSIs mimic the action of thyroid-stimulating hormone (TSH), a natural hormone produced by the pituitary gland that signals the thyroid to release thyroid hormones.
The Role of Thyroid-Stimulating Immunoglobulin (TSI)
TSIs bind to the TSH receptors on the surface of thyroid cells. Instead of signaling the gland to produce a normal amount of hormones, the TSIs continuously stimulate these receptors, causing the thyroid to become overactive and enlarge (a condition called a goiter). This relentless stimulation leads to the overproduction and release of excess T4 and T3 into the bloodstream. The body’s regulatory mechanisms, which would normally sense high thyroid hormone levels and reduce TSH production, are bypassed by the persistent action of TSI. This continuous signal from the TSIs ensures that the thyroid remains overstimulated, regardless of the body’s actual hormonal needs.
Genetic and Environmental Factors
While the precise trigger for this autoimmune misdirection is not fully understood, a combination of genetic predisposition and environmental factors is believed to play a significant role in the development of Graves’ disease. Individuals with a family history of autoimmune diseases, including Graves’ disease, thyroid disorders, or other conditions like type 1 diabetes or rheumatoid arthritis, are at a higher risk. However, having the genetic susceptibility does not guarantee the development of the disease; environmental factors are thought to act as triggers. Potential environmental triggers that have been investigated include viral infections, exposure to certain chemicals, and iodine intake. Stress has also been implicated as a potential factor that can exacerbate or even trigger autoimmune conditions in susceptible individuals. Research continues to explore the intricate interplay between genes and environment in initiating and perpetuating the autoimmune attack characteristic of Graves’ disease.
The Consequences of Excess Thyroid Hormones: Hyperthyroidism
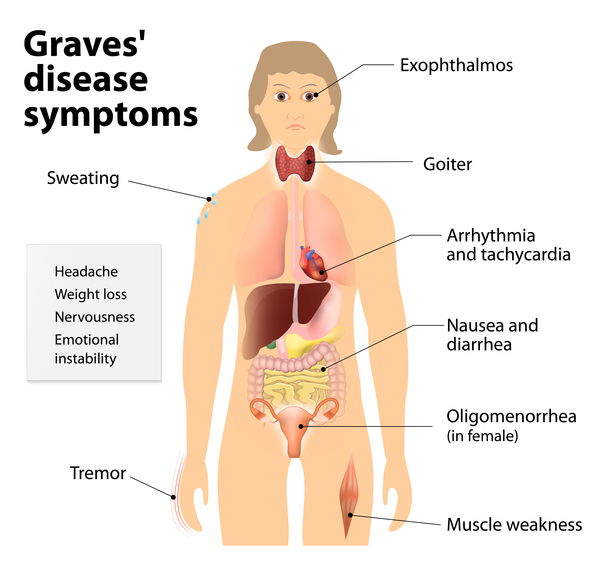
The overproduction of thyroid hormones by the overstimulated gland triggers a cascade of metabolic changes throughout the body, leading to the symptoms of hyperthyroidism. Thyroid hormones are crucial for regulating virtually every metabolic process, from heart rate and body temperature to digestion and energy utilization. When their levels are excessively high, these processes are sped up, resulting in a wide array of clinical manifestations.
Impact on Metabolism and Energy Levels
The most prominent effect of hyperthyroidism is a significant increase in the body’s metabolic rate. This means that cells are burning energy at an accelerated pace. Individuals often experience a persistent feeling of being “wired” or restless, even when trying to relax. Despite eating more food, many individuals with Graves’ disease lose weight because their bodies are expending energy at such a high rate. This can lead to fatigue and muscle weakness, paradoxically, due to the overstimulation. The increased metabolism also affects body temperature regulation, leading to an intolerance to heat and increased sweating, even in cool environments.
Cardiovascular and Neurological Manifestations
The cardiovascular system is particularly sensitive to elevated thyroid hormone levels. The heart pumps faster and harder, leading to symptoms like palpitations, a racing heart (tachycardia), and even irregular heartbeats, such as atrial fibrillation. Blood pressure may also be elevated, particularly systolic blood pressure. On a neurological level, the increased metabolic activity affects the nervous system, leading to symptoms like tremors, particularly in the hands, nervousness, irritability, anxiety, and difficulty sleeping. Some individuals may also experience mood swings and a heightened sense of anxiety.
Other Systemic Effects
Beyond the metabolic, cardiovascular, and neurological systems, excess thyroid hormones can impact virtually every other organ system. The digestive system speeds up, leading to increased bowel movements and sometimes diarrhea. The skin can become warm, moist, and thinner, with hair becoming fine and brittle. In women, menstrual irregularities are common. Eye problems, a hallmark of Graves’ disease, will be discussed in more detail below. In severe, untreated cases, hyperthyroidism can lead to a life-threatening condition called thyroid storm, characterized by a sudden and severe worsening of symptoms.
Unique Manifestations of Graves’ Disease: Beyond Hyperthyroidism
While hyperthyroidism is the primary consequence of Graves’ disease, the autoimmune nature of the condition can lead to specific and often distinctive symptoms that are not typically seen in other forms of thyroid overactivity. These manifestations are directly related to the immune system’s attack not only on the thyroid gland itself but also on tissues elsewhere in the body that share similar cellular components.
Graves’ Ophthalmopathy: The Eyes in Focus
One of the most recognizable and concerning complications of Graves’ disease is Graves’ ophthalmopathy, also known as Graves’ eye disease or thyroid eye disease. In this condition, the immune system mistakenly attacks the tissues and muscles surrounding the eyes. Antibodies and inflammatory cells target these structures, leading to inflammation, swelling, and, in some cases, the enlargement of the eye muscles and fatty tissue within the eye socket. This can cause a variety of symptoms, including:
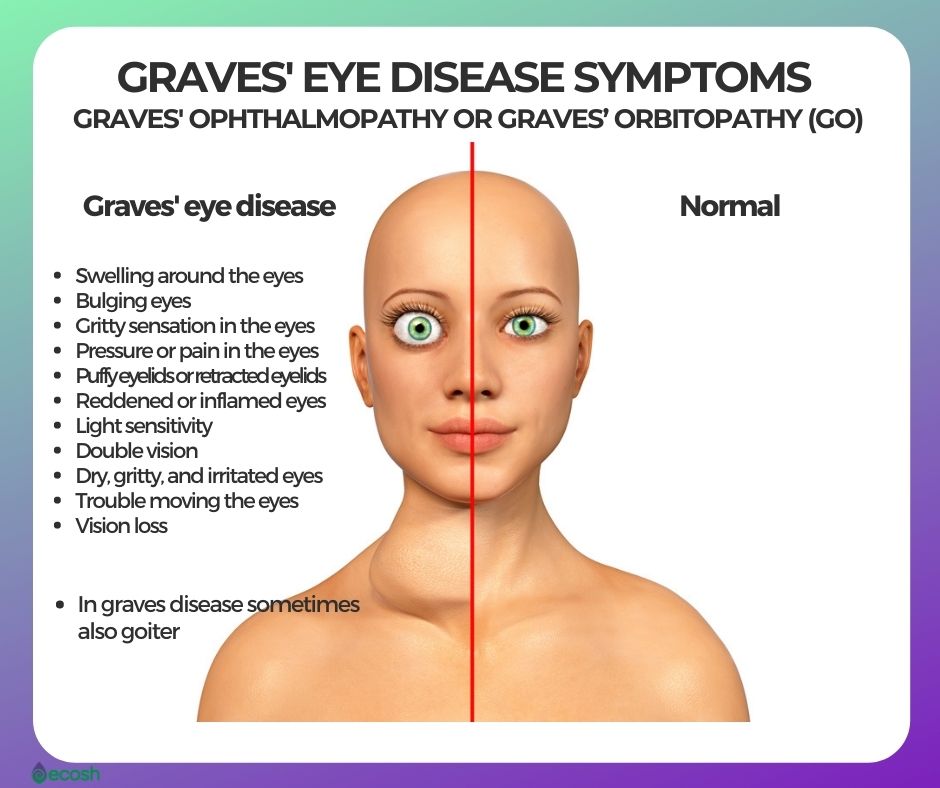
- Protrusion of the eyeballs (exophthalmos or proptosis): This is often the most striking symptom, where the eyes appear to bulge forward.
- Gritty sensation or dryness: Inflammation and altered tear production can lead to discomfort.
- Redness and swelling: The tissues around the eyes may become inflamed and puffy.
- Double vision (diplopia): Swelling or damage to the eye muscles can affect eye coordination.
- Light sensitivity: Increased sensitivity to light is common.
- Pain or pressure: Discomfort within or around the eyes can occur.
- Vision loss: In severe cases, compression of the optic nerve can lead to irreversible vision loss.
The severity of Graves’ ophthalmopathy can range from mild and barely noticeable to severe and sight-threatening. It’s important to note that eye symptoms can occur before, during, or even after the thyroid dysfunction is diagnosed and treated.
Pretibial Myxedema: Skin Changes
Another less common but characteristic manifestation of Graves’ disease is pretibial myxedema. This refers to a skin condition that affects the front of the lower legs. The immune system attacks the skin and subcutaneous tissues, causing them to thicken and develop a peau d’orange (orange peel) appearance. The affected skin may be reddish-brown and feel firm and lumpy. It is usually painless, but can sometimes be itchy or tender. While pretibial myxedema is a clear indicator of Graves’ disease, it occurs in a minority of patients, typically those with more severe forms of the condition.
Thyroid Acropachy: Rare Bone and Joint Changes
In extremely rare instances, a condition called thyroid acropachy can occur in individuals with long-standing Graves’ disease. This involves characteristic changes in the fingers and toes, including clubbing (widening and thickening of the fingertips) and swelling of the joints. It is a very uncommon manifestation and is usually associated with severe ophthalmopathy and pretibial myxedema.
Diagnosis and Management of Graves’ Disease
Diagnosing Graves’ disease involves a combination of medical history, physical examination, blood tests, and sometimes imaging studies. Once diagnosed, the management aims to control the overproduction of thyroid hormones and address any specific complications.
Diagnostic Tools and Blood Tests
A thorough medical history will include questions about symptoms suggestive of hyperthyroidism, as well as family history of thyroid or autoimmune disorders. A physical examination may reveal an enlarged thyroid gland (goiter), a rapid heart rate, tremors, and the characteristic eye changes of Graves’ ophthalmopathy.
Key blood tests used for diagnosis include:
- Thyroid-stimulating hormone (TSH): In Graves’ disease, TSH levels are typically very low or undetectable because the pituitary gland senses the high levels of thyroid hormones and reduces its own production of TSH.
- Free thyroxine (FT4) and free triiodothyronine (FT3): These will be elevated, confirming hyperthyroidism.
- Thyroid-stimulating immunoglobulin (TSI) or TSH receptor antibodies (TRAb): Detecting these antibodies is crucial for confirming the autoimmune basis of the hyperthyroidism and specifically diagnosing Graves’ disease.
- Thyroid peroxidase antibodies (TPOAb) and thyroglobulin antibodies (TgAb): While these antibodies are more commonly associated with Hashimoto’s thyroiditis, they can also be present in Graves’ disease.
Additional tests like a radioactive iodine uptake and scan can help assess thyroid function and size, but are less commonly used for initial diagnosis when TSI or TRAb levels are clearly positive.
Treatment Strategies: A Multimodal Approach
Treatment for Graves’ disease is tailored to the individual’s symptoms, severity, age, and presence of complications. The main goals are to reduce thyroid hormone production and manage symptoms. The primary treatment options include:
- Antithyroid Medications: Drugs such as methimazole and propylthiouracil (PTU) work by blocking the thyroid gland’s ability to produce thyroid hormones. These medications can effectively control hyperthyroidism and may lead to remission in some individuals. However, they require long-term use and can have side effects, including rare but serious ones like liver problems or a drop in white blood cell count.
- Radioactive Iodine Therapy: This treatment involves ingesting a capsule or liquid containing radioactive iodine. The thyroid gland absorbs the iodine, and the radiation selectively destroys overactive thyroid cells. This is a highly effective treatment that often leads to permanent hypothyroidism (underactive thyroid), which can then be managed with thyroid hormone replacement therapy. It is generally not recommended for pregnant or breastfeeding women.
- Surgery (Thyroidectomy): In some cases, surgical removal of all or part of the thyroid gland may be recommended. This is often considered for individuals who cannot tolerate antithyroid medications or radioactive iodine, have very large goiters causing compressive symptoms, or have suspected thyroid cancer. Like radioactive iodine, thyroidectomy typically results in permanent hypothyroidism requiring hormone replacement.

Managing Graves’ Ophthalmopathy and Other Complications
Managing Graves’ ophthalmopathy often requires a multidisciplinary approach. Mild cases may be managed with artificial tears, sunglasses to reduce light sensitivity, and head elevation to reduce swelling. More severe cases may require treatment with oral corticosteroids to reduce inflammation. In some instances, orbital radiation therapy or surgical interventions to decompress the eye socket or correct double vision may be necessary.
For pretibial myxedema, topical corticosteroids can sometimes help reduce inflammation and skin thickening.
Regular follow-up with an endocrinologist is essential for all individuals with Graves’ disease to monitor thyroid hormone levels, adjust treatment as needed, and screen for any new or worsening complications. While Graves’ disease is a chronic condition, with appropriate diagnosis and management, most individuals can lead healthy and fulfilling lives.