The human body possesses an intricate and highly sophisticated defense system, the immune system, designed to protect against a ceaseless barrage of pathogens, toxins, and internal threats. Central to this defense are white blood cells, or leukocytes, a diverse group of cells each specialized for distinct immunological roles. Among these, granulocytes stand out as a critical first line of cellular defense, characterized by the prominent granules in their cytoplasm, which contain a potent arsenal of enzymes and antimicrobial compounds. These polymorphic cells are not merely bystanders in the immune response; they are active, dynamic participants, constantly patrolling tissues and rapidly deploying to sites of infection or inflammation. Understanding granulocytes is fundamental to comprehending the body’s innate immunity, its response to diverse threats, and the delicate balance required for maintaining health.
The Fundamental Role of Granulocytes in Immunity
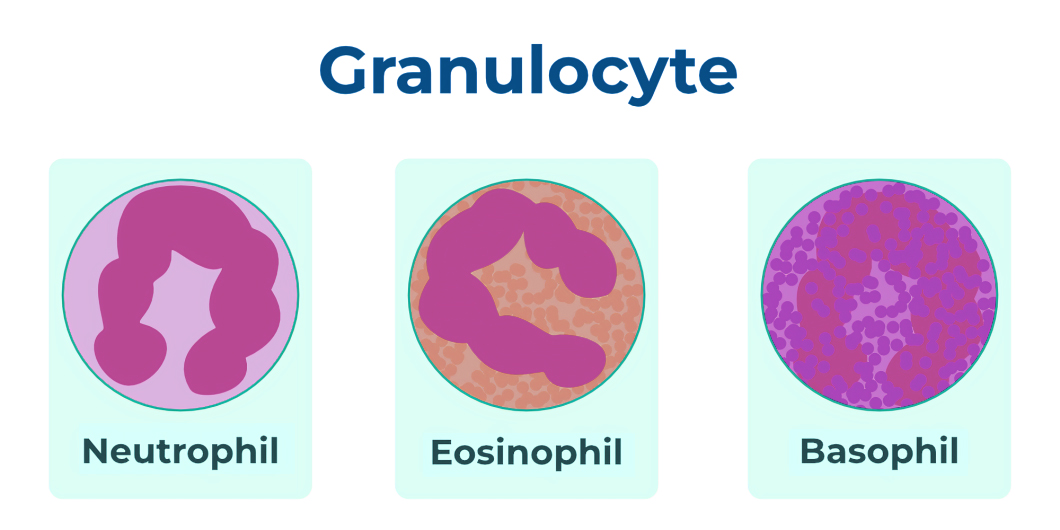
Granulocytes comprise three primary types: neutrophils, eosinophils, and basophils, each distinguished by the staining properties of their cytoplasmic granules and their unique functional specializations. Together, they represent a significant proportion of circulating white blood cells and are pivotal in orchestrating rapid, effective immune responses against a wide array of foreign invaders. Their collective actions range from direct phagocytosis and pathogen destruction to modulating inflammatory processes and allergic reactions, highlighting their multifaceted contribution to immune homeostasis.
Neutrophils: The First Responders
Neutrophils are the most abundant type of granulocyte, typically constituting 50-70% of all circulating white blood cells. Their characteristic multi-lobed nucleus and pale, finely granular cytoplasm make them identifiable under a microscope. Neutrophils are aptly termed the “first responders” of the immune system due to their rapid mobilization to sites of acute inflammation and infection. Upon sensing chemotactic signals released by damaged tissues or invading microbes, neutrophils quickly extravasate from the bloodstream, traversing endothelial barriers to reach the affected area.
Their primary mechanism of action is phagocytosis, wherein they engulf and destroy bacteria, fungi, and cellular debris. Once ingested, these pathogens are subjected to a lethal cocktail of reactive oxygen species (like superoxide and hydrogen peroxide) and enzymes contained within their granules, such as myeloperoxidase. Beyond phagocytosis, neutrophils also employ other sophisticated defense mechanisms, including degranulation (releasing antimicrobial compounds into the extracellular space) and the formation of neutrophil extracellular traps (NETs). NETs are intricate web-like structures composed of decondensed chromatin, histones, and granular proteins that trap and kill extracellular pathogens, acting as a final, desperate measure of defense when conventional phagocytosis is insufficient. The lifespan of neutrophils in circulation is remarkably short, often just 6-10 hours, underscoring their role in immediate, high-impact defense.
Eosinophils: Allergies and Parasitic Defense
Eosinophils, typically making up 1-4% of white blood cells, are distinguished by their bilobed nucleus and prominent, large red-staining granules (when stained with eosin). While less numerous than neutrophils, eosinophils play crucial, specialized roles, particularly in defense against parasitic infections and in the pathogenesis of allergic diseases. Their granules contain a unique array of cationic proteins, including major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and eosinophil peroxidase (EPO). These proteins are highly toxic to parasites, especially helminths (worms), and contribute to tissue damage in allergic and asthmatic conditions.
Upon activation, eosinophils degranulate, releasing these cytotoxic proteins into the extracellular environment to directly attack parasites too large for phagocytosis. Their involvement in allergic reactions and asthma is well-documented, where their activation contributes to bronchoconstriction, tissue inflammation, and airway remodeling through the release of inflammatory mediators like leukotrienes and prostaglandins. While their role in parasitic defense is protective, their contribution to allergic inflammation highlights the delicate balance of immune responses.
Basophils: Inflammation and Hypersensitivity
Basophils are the least common type of granulocyte, accounting for less than 1% of circulating white blood cells. They possess a bilobed nucleus (often obscured by their granules) and large, prominent blue-purple staining granules (with basic dyes) that contain histamine, heparin, serotonin, and other potent inflammatory mediators. Basophils are closely related to mast cells, which reside in tissues and share many functional similarities, particularly in mediating immediate hypersensitivity reactions.
When activated, typically by allergens binding to IgE antibodies on their surface, basophils rapidly degranulate, releasing their preformed mediators. Histamine, a key component, causes vasodilation, increases vascular permeability, and triggers smooth muscle contraction, contributing to the classic symptoms of allergy such as swelling, redness, and itching. Heparin acts as an anticoagulant, potentially preventing clot formation in areas of inflammation. While infamous for their role in anaphylaxis and allergic responses, basophils also contribute to anti-parasitic immunity and modulate adaptive immune responses, playing a more complex role than initially understood.
Granulopoiesis: The Journey of Formation
The continuous demand for granulocytes necessitates a robust and highly regulated production process known as granulopoiesis. This intricate hematopoietic pathway ensures a constant supply of these short-lived but vital immune cells, originating from pluripotent stem cells within the bone marrow.
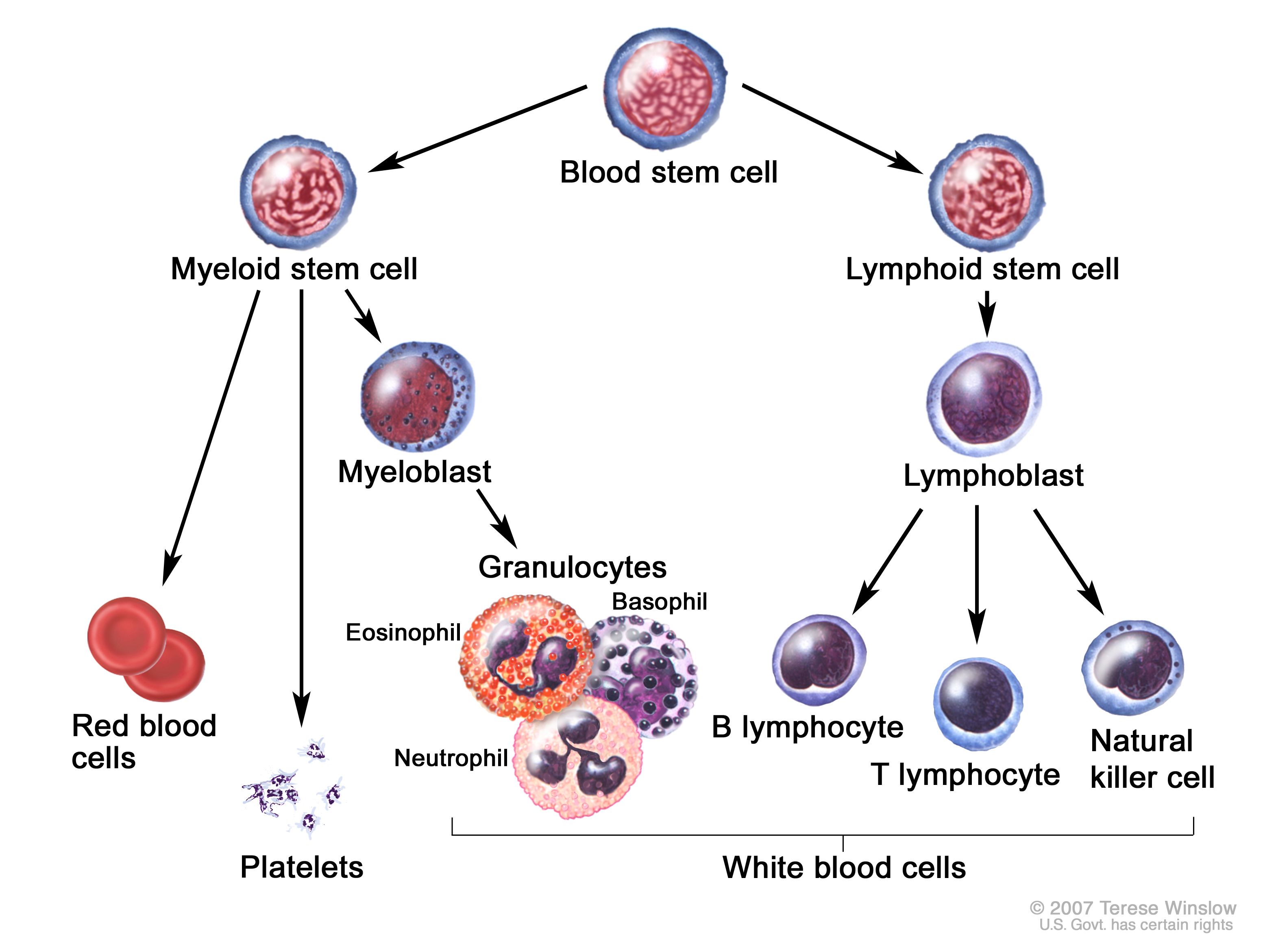
Myeloid Stem Cells to Mature Granulocytes
Granulopoiesis begins in the bone marrow with hematopoietic stem cells (HSCs), which are multipotent and capable of differentiating into all blood cell types. Under the influence of specific cytokines and growth factors, HSCs commit to the myeloid lineage, giving rise to common myeloid progenitors (CMPs). CMPs then differentiate into granulocyte-monocyte progenitors (GMPs), which are the direct precursors to granulocytes and monocytes.
The journey from GMP to mature granulocyte involves several distinct morphological stages:
- Myeloblast: The earliest identifiable granulocyte precursor, characterized by a large nucleus and minimal cytoplasm, lacking granules.
- Promyelocyte: Granules begin to appear in the cytoplasm (primary or azurophilic granules, which are non-specific).
- Myelocyte: Secondary (specific) granules, characteristic of neutrophils, eosinophils, or basophils, appear and begin to differentiate. This stage marks the commitment to a specific granulocyte lineage.
- Metamyelocyte: The nucleus begins to indent or kidney-shape, and granules become more pronounced. These cells lose their mitotic capability.
- Band form: The nucleus further constricts into a horseshoe or band shape. These are immature forms of granulocytes, particularly neutrophils, and can be released into circulation in response to severe infection (a “left shift”).
- Mature Granulocyte: The nucleus segments (in neutrophils), becomes bilobed (in eosinophils), or is obscured by granules (in basophils). These fully functional cells are released into the peripheral blood.
Regulatory Mechanisms of Production

The precise regulation of granulopoiesis is crucial for maintaining an appropriate balance of immune cells. Key regulatory molecules, particularly colony-stimulating factors (CSFs), govern the proliferation, differentiation, and maturation of granulocyte precursors. Granulocyte colony-stimulating factor (G-CSF) is perhaps the most critical, promoting the growth and differentiation of committed granulocyte progenitors and stimulating the release of mature neutrophils from the bone marrow. Granulocyte-macrophage colony-stimulating factor (GM-CSF) also plays a significant role in stimulating the proliferation of GMPs and the maturation of granulocytes and macrophages.
Other cytokines, such as interleukin-3 (IL-3), also contribute to the early stages of myeloid differentiation. The production and release of these growth factors are tightly controlled, often increasing dramatically during infections or inflammatory conditions to rapidly ramp up granulocyte production, ensuring the immune system can mount an effective defense. Conversely, their down-regulation helps to bring granulocyte counts back to normal levels once the threat has subsided.
Clinical Significance: When Granulocytes Go Awry
Dysregulation of granulocyte production or function can have profound implications for health, leading to various clinical conditions ranging from heightened susceptibility to infection to chronic inflammatory diseases. Monitoring granulocyte levels through a complete blood count (CBC) with differential is a routine diagnostic tool providing vital insights into a patient’s immune status.
Granulocytosis: Elevated Levels and Their Implications
Granulocytosis refers to an abnormally high number of granulocytes in the peripheral blood, most commonly elevated neutrophils (neutrophilia). This condition is a common indicator of acute bacterial infections, as the body mobilizes a massive influx of neutrophils to combat the invading pathogens. Other causes include inflammation (e.g., in autoimmune diseases like rheumatoid arthritis), tissue necrosis (e.g., after a heart attack), certain malignancies (especially myeloproliferative disorders), and stress or corticosteroid use.
While often a protective response, extreme or prolonged granulocytosis can sometimes indicate underlying pathological processes. For instance, in chronic myeloid leukemia, there is an uncontrolled proliferation of granulocytic precursors, leading to markedly elevated and dysfunctional granulocyte counts. Eosinophilia (elevated eosinophils) is typically associated with parasitic infections, allergic reactions (e.g., asthma, hay fever), and certain drug reactions. Basophilia (elevated basophils), though rare, can be seen in chronic myelogenous leukemia, allergic reactions, and hypothyroidism.
Granulocytopenia: Low Counts and Immune Compromise
Granulocytopenia, particularly neutropenia (a low neutrophil count), renders an individual highly vulnerable to infections. Neutropenia can arise from decreased production in the bone marrow (e.g., due to chemotherapy, radiation therapy, aplastic anemia, or viral infections suppressing marrow function), increased destruction or sequestration (e.g., autoimmune neutropenia, hypersplenism), or peripheral consumption (e.g., severe sepsis).
Patients with severe neutropenia are at high risk for life-threatening bacterial and fungal infections, often requiring prophylactic antibiotics and sometimes G-CSF therapy to stimulate neutrophil production. Agranulocytosis is a severe form of neutropenia characterized by a near absence of granulocytes, often induced by drugs (e.g., certain antithyroid medications, antipsychotics) and representing a medical emergency due to profound immune suppression. Understanding the cause of granulocytopenia is critical for appropriate management and preventing serious complications.
Granulocyte Disorders and Diagnostic Approaches
Beyond quantitative abnormalities, qualitative defects in granulocyte function can also lead to disease. Conditions like Chronic Granulomatous Disease (CGD) involve defects in the neutrophil’s ability to produce reactive oxygen species, rendering them unable to kill ingested pathogens effectively, leading to recurrent severe infections. Leukocyte Adhesion Deficiency (LAD) is another genetic disorder where neutrophils cannot properly adhere to endothelial cells and extravasate into tissues, impairing their ability to reach infection sites.
Diagnosis of granulocyte disorders relies on a combination of blood tests (CBC with differential), bone marrow examination, flow cytometry, genetic testing, and specific functional assays (e.g., neutrophil oxidative burst assay for CGD). These diagnostic tools are essential for accurately identifying the underlying pathology and guiding appropriate therapeutic interventions.
The Future of Granulocyte Research and Therapeutic Potential
Ongoing research continues to unravel the complex biology of granulocytes, revealing new insights into their diverse roles beyond conventional immune defense. This deeper understanding is paving the way for innovative therapeutic strategies.
Novel Insights into Immune Modulation
Recent studies have highlighted the plasticity of granulocytes and their capacity to modulate both innate and adaptive immune responses in ways previously underestimated. For instance, neutrophils are not merely suicidal pathogen killers; they can also interact with T cells and dendritic cells, influencing the initiation and progression of adaptive immunity. Eosinophils are being recognized for their roles in tissue repair and remodeling, as well as their contribution to homeostatic functions in various organs. Basophils are emerging as important regulators of T helper 2 (Th2) cell differentiation, crucial for allergic and anti-parasitic responses. Further research into these nuanced roles could open new avenues for immune modulation in chronic inflammatory diseases, autoimmune disorders, and cancer.
Therapeutic Targeting and Personalized Medicine
The increasing understanding of granulocyte biology is translating into promising therapeutic applications. G-CSF remains a cornerstone in treating neutropenia, particularly in cancer patients undergoing chemotherapy. However, newer strategies are exploring more precise targeting. For example, specific inhibitors of neutrophil chemoattractant receptors are being investigated for treating inflammatory conditions where neutrophil infiltration is detrimental. In allergic diseases, therapies that target eosinophil activation or deplete eosinophil numbers are showing efficacy.
The future likely holds more personalized approaches, where granulocyte profiles and functional states could serve as biomarkers for disease prognosis and therapeutic response. Tailoring treatments based on an individual’s specific granulocyte dysfunction or dysregulation represents a significant step towards precision medicine, ultimately aiming to harness the protective power of these essential immune cells while mitigating their pathological contributions. The dynamic world of granulocytes continues to be a fertile ground for discovery, promising advances that will reshape our approach to infectious diseases, inflammation, and beyond.