The Activated Partial Thromboplastin Time (APTT) lab test, often referred to as the PTT test, is a crucial diagnostic tool used by healthcare professionals to evaluate the intrinsic and common pathways of the blood coagulation cascade. Essentially, it measures how long it takes for a blood clot to form in a sample of blood plasma after specific reagents have been added. This test is vital for diagnosing bleeding disorders, monitoring anticoagulant therapy, and assessing liver function. Understanding the nuances of the APTT test, including what it measures, why it’s performed, and how its results are interpreted, is fundamental to comprehending its significance in clinical practice.

Understanding Blood Clotting and the APTT Test
Blood clotting, or hemostasis, is a complex physiological process designed to prevent excessive blood loss when a blood vessel is injured. It involves a sophisticated cascade of proteins known as clotting factors. These factors, numbered and named systematically, interact in a specific sequence to form a stable fibrin clot that seals the injured site.
The coagulation cascade is broadly divided into two main pathways: the extrinsic pathway and the intrinsic pathway. The extrinsic pathway is activated by tissue factor released from damaged tissues outside the bloodstream. The intrinsic pathway is activated by contact with negatively charged surfaces within the bloodstream, such as the damaged lining of a blood vessel or, in a lab setting, the glass tube used for blood collection. Both pathways converge at a common pathway, ultimately leading to the formation of thrombin, an enzyme that converts fibrinogen into fibrin, the protein meshwork that forms the clot.
The APTT test specifically assesses the intrinsic pathway and the common pathway of this cascade. It does so by introducing reagents in the laboratory that bypass the extrinsic pathway’s initial activation step, thereby isolating the functionality of the intrinsic and common pathways.
The Coagulation Cascade in Detail
To fully appreciate the APTT test, a deeper understanding of the coagulation cascade is beneficial. The cascade begins with inactive precursor proteins, called zymogens. Upon activation, these zymogens transform into active enzymes that then activate the next component in the sequence.
- Intrinsic Pathway: This pathway involves factors XII, XI, IX, and VIII. It is initiated when blood comes into contact with negatively charged surfaces.
- Extrinsic Pathway: This pathway involves tissue factor and factor VII. It is primarily activated by tissue damage.
- Common Pathway: This pathway, involving factors X, V, II (prothrombin), and I (fibrinogen), is where both the intrinsic and extrinsic pathways converge. Thrombin is generated here, which then converts fibrinogen into fibrin.
The APTT test measures the time it takes for blood to clot when the intrinsic pathway is stimulated in vitro. It utilizes substances like silica or kaolin to activate factor XII, mimicking the contact activation that occurs in vivo. Calcium ions (often added as citrate or EDTA in the collection tube, then reversed with calcium chloride during testing) and phospholipids are also essential components added to the plasma sample to facilitate the clotting process.
How the APTT Test is Performed
The APTT test is a laboratory-based procedure. A blood sample is typically drawn from a vein, usually in the arm, and collected in a special tube containing an anticoagulant, most commonly sodium citrate. This anticoagulant prevents the blood from clotting in the tube.
Once the blood is collected, it is quickly taken to the laboratory. There, the plasma is separated from the red blood cells by centrifugation. The laboratory technician then adds specific reagents to a measured amount of the patient’s plasma. These reagents typically include:
- Activator: A substance like silica, kaolin, or celite is added to trigger the intrinsic pathway by activating factor XII.
- Phospholipids: These provide a surface for the clotting factors to assemble and react.
- Calcium Chloride: Since citrate or EDTA anticoagulants bind calcium ions, which are essential for clotting, calcium chloride is added to reverse the anticoagulant effect and allow the clotting cascade to proceed.
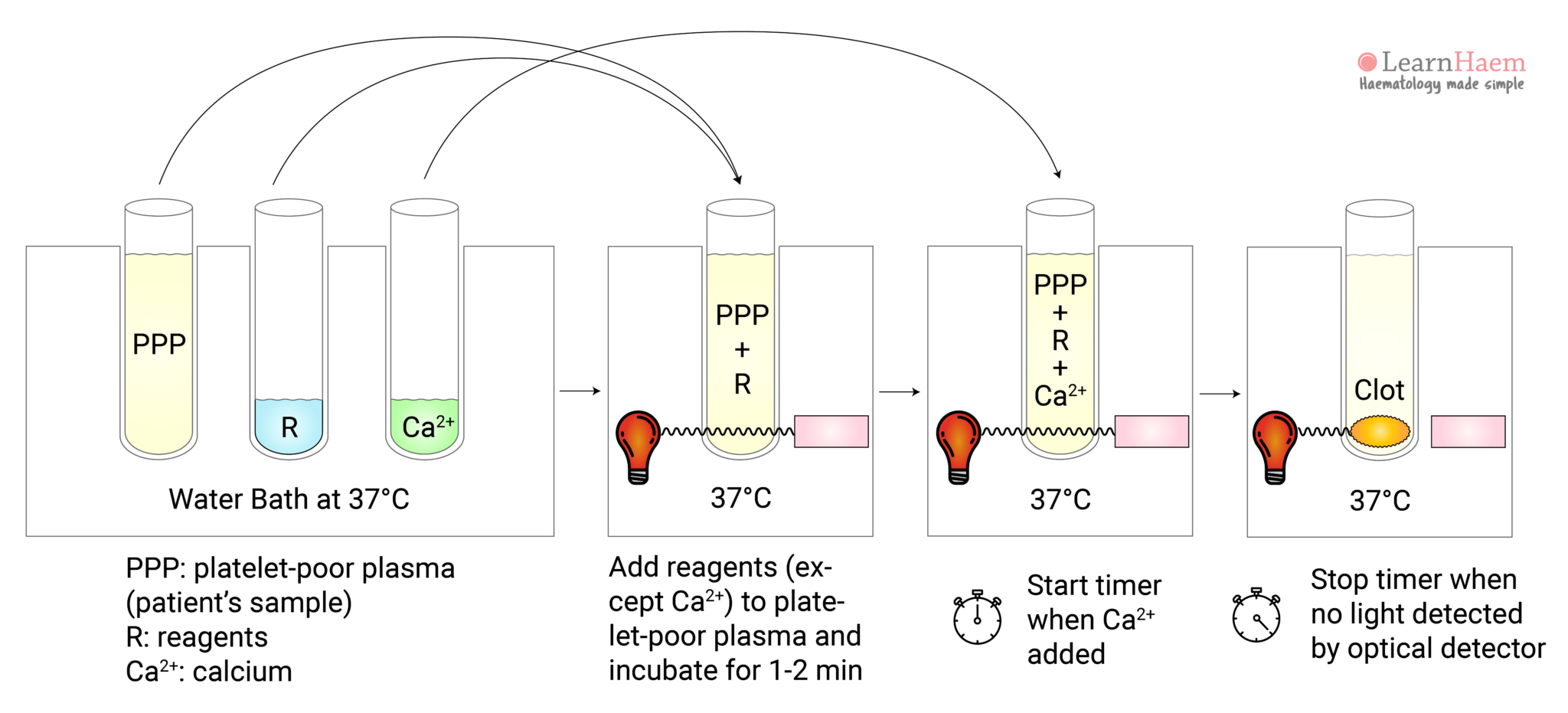
The mixture is then incubated at a controlled temperature (usually 37°C). At specific intervals, a reagent that activates the common pathway (such as thromboplastin or a tissue factor preparation) is added, and the time taken for a clot to form is precisely measured. Modern automated analyzers use optical or mechanical methods to detect clot formation. The time elapsed from the addition of the activating reagents to the formation of a visible clot is the APTT value, reported in seconds.
Why is the APTT Test Performed?
The APTT test serves several critical clinical purposes, primarily related to the evaluation of bleeding and clotting tendencies.
Diagnosing Bleeding Disorders
One of the primary uses of the APTT test is to investigate the cause of unexplained bleeding. If a patient experiences symptoms such as easy bruising, prolonged bleeding after injury or surgery, or heavy menstrual bleeding, an APTT test can help determine if a defect in the intrinsic or common pathways of coagulation is responsible.
- Factor Deficiencies: The APTT test is particularly sensitive to deficiencies in factors XII, XI, IX, and VIII, all of which are part of the intrinsic pathway. A prolonged APTT can indicate a deficiency in one or more of these factors. For instance, a significantly prolonged APTT in conjunction with a normal prothrombin time (PT) often points towards a deficiency in one of these intrinsic pathway factors.
- Hemophilia: Hemophilia A (deficiency of factor VIII) and Hemophilia B (deficiency of factor IX) are classic examples of bleeding disorders diagnosed and monitored using APTT tests. In these conditions, the APTT is typically prolonged due to the impaired function of the intrinsic pathway.
- Von Willebrand Disease: While Von Willebrand disease primarily affects platelet function and factor VIII levels (as Von Willebrand factor protects factor VIII), it can sometimes lead to a mildly prolonged APTT, particularly if factor VIII levels are significantly reduced.
Monitoring Anticoagulant Therapy
The APTT test is extensively used to monitor patients receiving anticoagulant medications, most notably unfractionated heparin.
- Heparin Therapy: Unfractionated heparin is a potent anticoagulant that works by accelerating the activity of antithrombin III, which in turn inhibits thrombin (factor IIa) and factor Xa. Because heparin’s effect is primarily on the intrinsic and common pathways, the APTT test is the standard laboratory test for monitoring its therapeutic dosage. The goal is to achieve an APTT value within a specific therapeutic range, typically 1.5 to 2.5 times the patient’s baseline or control APTT, to ensure effective anticoagulation while minimizing the risk of bleeding. If the APTT is too low, it suggests insufficient anticoagulation, and the heparin dose may need to be increased. If the APTT is too high, it indicates excessive anticoagulation, increasing the risk of hemorrhage, and the heparin dose may need to be reduced or temporarily stopped.
- Other Anticoagulants: While less common, APTT may also be used to monitor other anticoagulants that affect the intrinsic pathway, although specific assays are often preferred for newer oral anticoagulants.
Assessing Liver Function
The liver plays a crucial role in synthesizing most of the clotting factors (factors I, II, V, VII, IX, X, XI, and XII). Therefore, severe liver disease can impair the production of these factors, leading to a tendency for bleeding.
- Liver Disease: A prolonged APTT, especially when combined with a prolonged PT, can be an indicator of impaired synthetic function of the liver. This is because the liver’s inability to produce adequate amounts of clotting factors compromises both the intrinsic and extrinsic pathways.
Detection of Specific Inhibitors
APTT can also help detect the presence of circulating anticoagulants, such as lupus anticoagulants and inhibitors against specific clotting factors.
- Lupus Anticoagulant: These are antibodies that interfere with phospholipid-dependent coagulation reactions, leading to a prolonged APTT and an increased risk of thrombosis (blood clots). Despite their name, they are associated with an increased risk of clotting, not bleeding.
- Factor Inhibitors: In some individuals, particularly those with hemophilia who have been treated with clotting factor concentrates, antibodies (inhibitors) can develop against specific clotting factors (e.g., factor VIII inhibitors). These inhibitors neutralize the activity of the factor, leading to a prolonged APTT and resistance to treatment with replacement therapy. Mixing studies, where patient plasma is mixed with normal plasma, can help differentiate between a factor deficiency and the presence of an inhibitor.
Interpreting APTT Test Results
Interpreting APTT test results requires a comprehensive understanding of the patient’s clinical history, medications, and other laboratory findings.
Normal APTT Ranges
The normal range for APTT can vary slightly between laboratories due to differences in reagents and testing methods. However, a typical normal range for adults is generally between 25 and 35 seconds. For infants, normal ranges may be slightly longer. It is crucial to always refer to the reference range provided by the specific laboratory performing the test.
Prolonged APTT
A prolonged APTT (longer than the normal range) indicates that it is taking longer than usual for a blood clot to form. This can be due to several reasons:
- Medications: The most common cause of a prolonged APTT is the use of unfractionated heparin. Other medications, such as direct thrombin inhibitors (e.g., dabigatran) and some direct factor Xa inhibitors, can also affect APTT, although specific assays are often used for monitoring these.
- Coagulation Factor Deficiencies: As discussed, deficiencies in factors XII, XI, IX, or VIII (e.g., Hemophilia) will lead to a prolonged APTT. Deficiencies in factors in the common pathway (X, V, II, I) will also prolong APTT, but usually, the PT will also be prolonged.
- Liver Disease: Severe impairment of liver function can lead to reduced synthesis of clotting factors.
- Vitamin K Deficiency: Vitamin K is essential for the synthesis of factors II, VII, IX, and X. While a deficiency primarily affects the extrinsic pathway (indicated by a prolonged PT), severe deficiency can impact common pathway factors, leading to a prolonged APTT.
- Disseminated Intravascular Coagulation (DIC): In the early stages of DIC, clotting factors are consumed, leading to a prolonged APTT and PT, alongside a low platelet count.
- Lupus Anticoagulant: The presence of a lupus anticoagulant will prolong the APTT.
- Von Willebrand Disease (severe types): In some cases, particularly with severe factor VIII deficiency, APTT can be prolonged.
- Rare Inherited Disorders: Certain rare inherited disorders affecting intrinsic pathway factors can cause prolonged APTT.
Shortened APTT
A shortened APTT (shorter than the normal range) is less common and typically less clinically significant than a prolonged APTT. However, it can sometimes indicate:
- Hypercoagulable States: Conditions where the blood has an increased tendency to clot.
- High Levels of Certain Clotting Factors: Rare conditions can lead to abnormally high levels of some clotting factors, which might slightly shorten the APTT.
- Sample Contamination or Testing Errors: This is often the most likely cause of a significantly shortened APTT.
The Role of the PT Test
It is crucial to interpret the APTT results in conjunction with the Prothrombin Time (PT) test. The PT test measures the extrinsic and common pathways of coagulation.
- Prolonged APTT, Normal PT: This strongly suggests a problem within the intrinsic pathway (factors XII, XI, IX, VIII) or a specific inhibitor of the intrinsic pathway.
- Prolonged PT, Normal APTT: This points to an issue in the extrinsic pathway (factor VII) or severe Vitamin K deficiency affecting factors II, VII, IX, X.
- Prolonged APTT and Prolonged PT: This indicates a problem in the common pathway (factors X, V, II, I), severe liver disease, Vitamin K deficiency, or DIC.

Limitations and Considerations
While the APTT test is an invaluable diagnostic tool, it has certain limitations and requires careful consideration of various factors:
- Sensitivity Variations: The sensitivity of the APTT test to specific factor deficiencies varies. For instance, it is highly sensitive to severe deficiencies of factors VIII and IX but less sensitive to mild deficiencies of factor XII.
- Medication Interference: Many medications can affect APTT results, necessitating a thorough review of the patient’s medication list.
- Sample Quality: Improper sample collection, handling, or storage can lead to inaccurate results. For example, a clotted sample or a sample with insufficient anticoagulant can yield falsely short clotting times.
- Laboratory Variability: Differences in reagents and methodologies across laboratories can lead to variations in reported normal ranges and results.
- Inhibitors: The presence of specific inhibitors (antibodies) against clotting factors can lead to falsely prolonged APTT, which may be misinterpreted as a severe deficiency. Mixing studies are often performed in such cases to elucidate the underlying cause.
- Fibrinogen Levels: Very low fibrinogen levels (afibrinogenemia or severe dysfibrinogenemia) can also lead to a prolonged APTT, as fibrinogen is the final substrate for clot formation.
In conclusion, the APTT lab test is a cornerstone of hemostasis laboratory testing, providing critical insights into the functioning of the intrinsic and common pathways of blood coagulation. Its applications range from diagnosing bleeding disorders and monitoring anticoagulant therapy to assessing liver function and detecting specific inhibitors. A thorough understanding of the test’s principles, indications, and interpretation, alongside other coagulation tests and clinical context, is essential for its effective utilization in patient care.