Anemia of chronic disease (ACD), also known as anemia of inflammation, is a common type of anemia that develops in people with certain long-term medical conditions. It is characterized by a reduced red blood cell count or a lower than normal amount of hemoglobin, the protein in red blood cells that carries oxygen throughout the body. While it shares some similarities with other types of anemia, ACD has a distinct underlying mechanism, making its diagnosis and management unique. Understanding ACD is crucial for healthcare professionals and patients alike, as it can impact the progression of underlying diseases and the overall well-being of individuals.
Understanding the Pathophysiology of Anemia of Chronic Disease
At its core, anemia of chronic disease is a disorder of iron metabolism and red blood cell production. It is not caused by a direct deficiency of iron in the body’s stores, but rather by an impaired ability to utilize that iron effectively for erythropoiesis (red blood cell formation). This impairment stems from the inflammatory processes associated with chronic diseases.
The Role of Inflammation in Iron Dysregulation
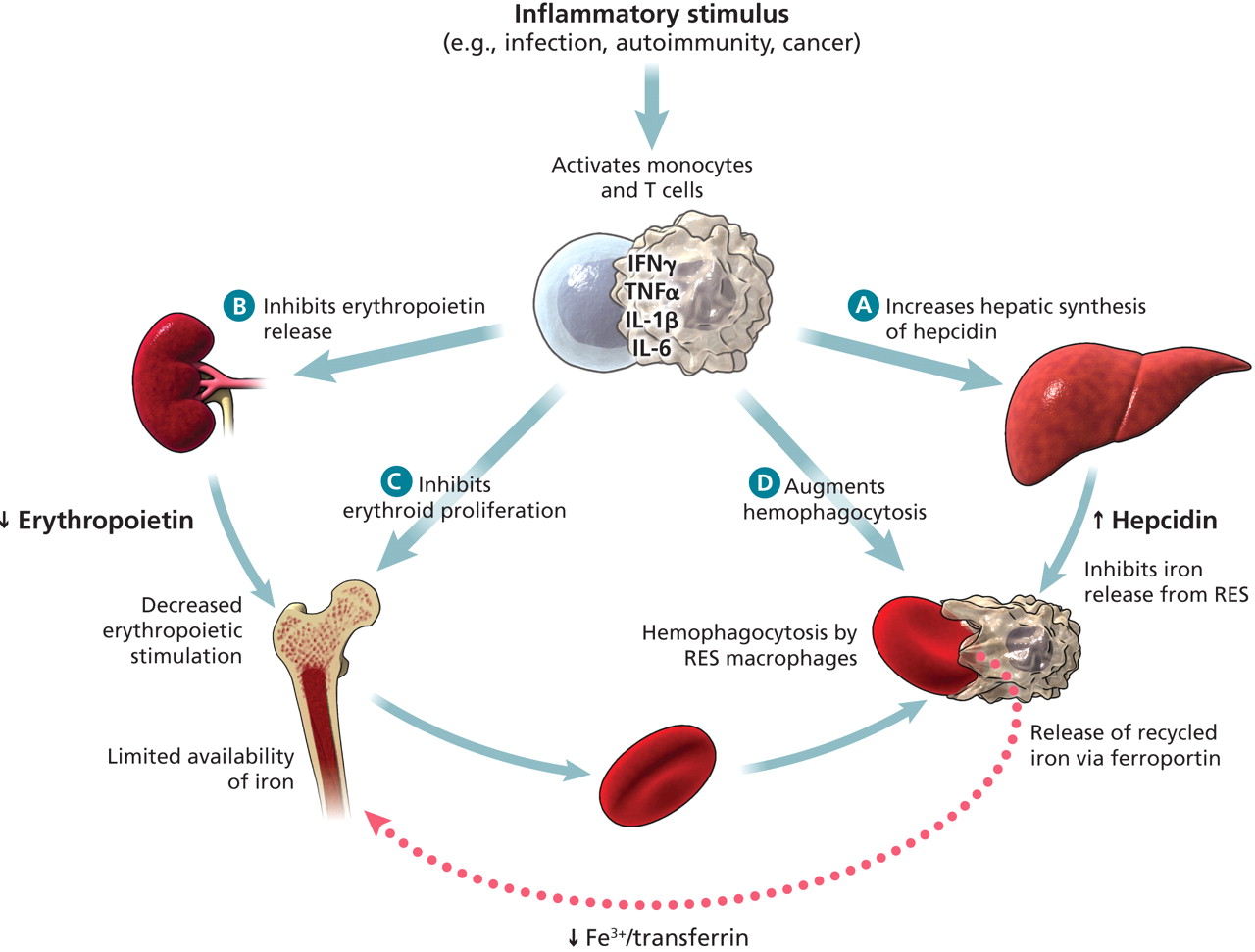
Chronic diseases, whether infectious, autoimmune, or malignant, trigger a sustained inflammatory response. During this response, the body releases pro-inflammatory cytokines, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). These cytokines play a central role in the pathogenesis of ACD through several key mechanisms:
-
Hepcidin Upregulation: Pro-inflammatory cytokines, particularly IL-6, stimulate the liver to produce more hepcidin. Hepcidin is the master regulator of systemic iron metabolism. It works by binding to ferroportin, the sole known cellular iron exporter, leading to its degradation. Ferroportin is found on the surface of enterocytes (intestinal cells that absorb iron), macrophages (which recycle iron from senescent red blood cells), and hepatocytes (liver cells that store iron). By degrading ferroportin, hepcidin effectively locks iron within these cells, preventing its release into the bloodstream. This leads to:
- Reduced Intestinal Iron Absorption: When hepcidin is high, less iron is absorbed from the diet in the small intestine.
- Impaired Macrophage Iron Release: Macrophages that engulf old red blood cells normally release iron for reuse. High hepcidin prevents this release, trapping iron within macrophages.
- Decreased Serum Iron: As iron is sequestered within cells, the amount of iron available in the serum (the liquid component of blood) decreases.
-
Erythropoietin Resistance: While the kidneys are responsible for producing erythropoietin (EPO), the hormone that stimulates the bone marrow to produce red blood cells, inflammation can render the bone marrow less responsive to EPO’s signals. This means that even if EPO levels are adequate, the bone marrow may not effectively produce new red blood cells. This resistance can be attributed to:
- Direct Inhibitory Effects of Cytokines: Some inflammatory cytokines can directly inhibit erythroid progenitor cells in the bone marrow.
- Reduced EPO Production: In some chronic conditions, kidney function may be compromised, leading to reduced EPO production. However, in ACD, EPO resistance is a more prominent factor than EPO deficiency itself.
-
Reduced Red Blood Cell Lifespan: Inflammatory mediators can also lead to a shortened lifespan of red blood cells. This means that red blood cells are destroyed at a faster rate than they can be replaced, further contributing to the anemia.
Impaired Erythropoiesis
The combination of iron sequestration, reduced iron availability for hemoglobin synthesis, and EPO resistance culminates in impaired erythropoiesis. The bone marrow is unable to produce enough mature red blood cells to compensate for the normal rate of red blood cell destruction, resulting in a decrease in the overall red blood cell count and hemoglobin concentration. This state of ineffective erythropoiesis is a hallmark of ACD.
Clinical Manifestations and Diagnosis of Anemia of Chronic Disease
The symptoms of anemia of chronic disease are often insidious and can be easily overlooked, especially when they occur in the context of a more significant underlying illness. The diagnosis relies on a combination of clinical assessment, laboratory findings, and the exclusion of other causes of anemia.
Recognizing the Symptoms
The symptoms of anemia are generally related to reduced oxygen-carrying capacity of the blood. In ACD, these symptoms can be mild to moderate and may be masked by the signs and symptoms of the primary chronic disease. Common manifestations include:
- Fatigue and Weakness: This is the most common symptom, often described as a persistent tiredness that doesn’t improve with rest.
- Pallor: The skin, conjunctiva (lining of the eyelids), and nail beds may appear paler than usual due to decreased hemoglobin.
- Shortness of Breath (Dyspnea): Especially with exertion, as the body struggles to deliver sufficient oxygen to tissues.
- Headaches and Dizziness: Reduced oxygen supply to the brain can cause these symptoms.
- Cold Hands and Feet: Poor circulation due to reduced oxygen transport.
- Chest Pain: In severe cases, the heart may have to work harder to compensate for low oxygen levels, leading to chest discomfort.
It is important to note that in many individuals with ACD, the anemia is mild and may not cause noticeable symptoms. The degree of anemia often correlates with the severity and duration of the underlying chronic disease.
Diagnostic Workup for ACD
Diagnosing ACD involves a comprehensive approach to differentiate it from other types of anemia, particularly iron deficiency anemia. Key laboratory tests include:
- Complete Blood Count (CBC): This fundamental test measures red blood cells, white blood cells, and platelets. In ACD, the CBC typically shows a normocytic, normochromic anemia, meaning the red blood cells are of normal size and hemoglobin content. However, in later stages or if there are coexisting iron deficiency, a microcytic, hypochromic anemia can be observed.
- Serum Iron: This test measures the amount of iron circulating in the blood. In ACD, serum iron levels are typically low due to the sequestration of iron by inflammatory mediators.
- Total Iron-Binding Capacity (TIBC) or Transferrin Saturation: TIBC measures the blood’s capacity to bind iron with transferrin, the main iron transport protein. Transferrin saturation is the percentage of transferrin that is actually carrying iron. In ACD, TIBC is usually low or normal, and transferrin saturation is also low. This pattern (low serum iron, low TIBC/transferrin saturation) helps distinguish ACD from iron deficiency anemia, where TIBC is typically high and transferrin saturation is low or normal.
- Serum Ferritin: Ferritin is the primary iron storage protein. In ACD, serum ferritin levels are typically normal or elevated. This is a crucial distinguishing feature from iron deficiency anemia, where ferritin is significantly low. The elevated ferritin in ACD reflects the increased iron stores within macrophages and the liver, even though this iron is not readily available for erythropoiesis.
- C-Reactive Protein (CRP) or Erythrocyte Sedimentation Rate (ESR): These are markers of inflammation. Elevated CRP or ESR levels support the diagnosis of an underlying inflammatory condition contributing to the anemia.
- Erythropoietin (EPO) Levels: Measuring EPO levels can help assess the bone marrow’s response. In ACD, EPO levels are often inappropriately low for the degree of anemia, or the bone marrow is resistant to its effects.
- Peripheral Blood Smear: This microscopic examination of blood can reveal the morphology of red blood cells and other blood cells, providing further clues to the diagnosis.
The diagnostic process often involves excluding other common causes of anemia, such as vitamin B12 deficiency, folate deficiency, and hemolytic anemias. A thorough medical history, physical examination, and a systematic approach to laboratory testing are essential for accurate diagnosis.
Underlying Conditions Associated with Anemia of Chronic Disease
Anemia of chronic disease is not a standalone diagnosis but rather a consequence of an underlying chronic inflammatory condition. The spectrum of these conditions is broad, encompassing a variety of disease categories. Identifying and managing the primary disease is paramount for improving the anemia.

Infectious Diseases
Persistent or recurring infections can trigger the inflammatory cascades that lead to ACD. Examples include:
- Tuberculosis (TB): A chronic bacterial infection that can induce significant inflammation.
- HIV/AIDS: The chronic inflammation associated with HIV infection can contribute to ACD.
- Endocarditis: Long-standing bacterial infections of the heart valves.
- Osteomyelitis: Chronic bone infections.
- Viral Hepatitis: Chronic viral infections of the liver.
Inflammatory and Autoimmune Disorders
Conditions characterized by dysregulated immune responses and chronic inflammation are frequent culprits for ACD. These include:
- Rheumatoid Arthritis (RA): An autoimmune disease that attacks the joints, leading to systemic inflammation.
- Systemic Lupus Erythematosus (SLE): A multisystem autoimmune disease.
- Inflammatory Bowel Disease (IBD): Conditions like Crohn’s disease and ulcerative colitis cause chronic inflammation of the gastrointestinal tract.
- Vasculitis: Inflammation of blood vessels.
- Ankylosing Spondylitis: A type of arthritis that affects the spine.
Malignancies
Cancer itself, and the inflammatory response it elicits, can lead to ACD. This is particularly common in:
- Lymphomas: Cancers of the lymphatic system.
- Leukemias: Cancers of the blood-forming tissues.
- Solid Tumors: Such as lung cancer, colon cancer, and breast cancer. The tumor burden and associated inflammation contribute significantly.
Other Chronic Conditions
Beyond infections, autoimmune disorders, and cancers, other chronic conditions can also predispose individuals to ACD:
- Chronic Kidney Disease (CKD): While CKD can cause anemia due to EPO deficiency, it can also contribute to ACD due to underlying inflammation.
- Congestive Heart Failure (CHF): Chronic inflammation and reduced organ perfusion in CHF can lead to ACD.
- Chronic Obstructive Pulmonary Disease (COPD): The persistent inflammation in the lungs associated with COPD can contribute to anemia.
- Diabetes Mellitus: While not always directly inflammatory, diabetes can be associated with low-grade chronic inflammation and can exacerbate ACD.
The underlying condition dictates the treatment strategy. For instance, treating a bacterial infection with antibiotics, managing an autoimmune disease with immunosuppressants, or treating cancer with chemotherapy or radiation therapy can all help resolve the inflammation and, consequently, improve the anemia of chronic disease.
Management and Treatment Strategies for Anemia of Chronic Disease
The management of anemia of chronic disease centers on two main pillars: treating the underlying chronic condition and, in some cases, directly addressing the anemia itself. The goal is to reduce inflammation and restore normal iron metabolism and red blood cell production.
Addressing the Underlying Chronic Condition
This is the cornerstone of ACD management. Without effective control of the primary disease, any treatment aimed solely at the anemia is unlikely to be successful in the long term. The specific approach will vary greatly depending on the diagnosis:
- Infectious Diseases: Prompt and appropriate antimicrobial therapy is essential.
- Autoimmune and Inflammatory Disorders: Management often involves disease-modifying antirheumatic drugs (DMARDs), biologics, corticosteroids, or other immunosuppressive agents to reduce inflammation.
- Malignancies: Treatment typically involves chemotherapy, radiation therapy, surgery, or immunotherapy, aiming to reduce tumor burden and associated inflammation.
- Chronic Kidney Disease: Management includes addressing underlying causes, controlling blood pressure, and managing complications.
Effective treatment of the primary condition often leads to a decrease in inflammatory cytokines, a reduction in hepcidin production, and a subsequent improvement in iron availability and erythropoiesis, thereby resolving the anemia.
Strategies for Anemia Correction
In cases where the anemia is severe, symptomatic, or not responding adequately to treatment of the underlying condition, additional interventions may be considered.
- Iron Supplementation: While ACD is characterized by iron dysregulation, not necessarily iron deficiency, judicious use of iron supplements can sometimes be beneficial. However, oral iron supplements may be poorly absorbed in the presence of high hepcidin levels. Intravenous (IV) iron therapy is often more effective because it bypasses the intestinal absorption barrier and directly replenishes iron stores. IV iron can be particularly helpful in patients with inflammatory bowel disease or those undergoing chemotherapy. Careful monitoring is required to avoid iron overload.
- Erythropoiesis-Stimulating Agents (ESAs): ESAs, such as recombinant human erythropoietin (epoetin alfa) and darbepoetin alfa, are synthetic versions of the hormone EPO. They stimulate the bone marrow to produce more red blood cells. ESAs are typically reserved for patients with moderate to severe anemia who are symptomatic and for whom other treatments have been insufficient. They are most effective when iron stores are adequate. Their use requires careful monitoring of hemoglobin levels to avoid overproduction, which can increase the risk of thrombotic events.
- Blood Transfusions: In cases of severe, symptomatic anemia where rapid correction is needed, blood transfusions may be administered to quickly raise hemoglobin levels and improve oxygen delivery to tissues. This is a supportive measure rather than a curative treatment for ACD itself.

Prognosis and Long-Term Outlook
The prognosis for patients with anemia of chronic disease is largely dependent on the underlying condition. Successful management of the primary disease often leads to improvement or resolution of the anemia. However, in cases of severe or progressive chronic diseases, ACD can persist and contribute to morbidity. Regular monitoring of hemoglobin levels and iron parameters is important to assess the effectiveness of treatment and detect any recurrence. By understanding the complex interplay between inflammation and iron metabolism, healthcare providers can effectively diagnose and manage anemia of chronic disease, improving the quality of life for affected individuals.