The world of healthcare billing and coding can often feel like an intricate labyrinth. For medical professionals and administrative staff alike, navigating the complexities of assigning accurate codes for services rendered is paramount to ensuring proper reimbursement and maintaining the integrity of patient records. Among the most frequently encountered and sometimes perplexing of these codes are Evaluation and Management (E/M) codes. These codes form the bedrock of how physicians and other qualified healthcare professionals document and bill for the cognitive and clinical work involved in patient encounters. Understanding the nuances of E/M coding is not merely an administrative task; it’s a critical component of a functional healthcare system.
The Foundation of Evaluation and Management Coding
At its core, an E/M code represents the level of service provided to a patient during an office visit or other outpatient encounter. These codes are designed to reflect the complexity of the patient’s medical condition, the amount of time spent by the clinician, and the diagnostic reasoning involved. Unlike procedural codes that describe a specific intervention (like a surgery or diagnostic test), E/M codes capture the comprehensive nature of a patient visit, encompassing the history taken, the physical examination performed, and the medical decision-making process.
Evolution of E/M Coding Guidelines
The guidelines for E/M coding have undergone significant revisions over the years, aiming to streamline the process and better align with the realities of modern medical practice. Historically, E/M coding relied heavily on the “three key components”:
- History: The patient’s subjective account of their symptoms, past medical history, family history, and social history.
- Examination: The physician’s objective findings from a physical assessment of the patient.
- Medical Decision Making (MDM): The clinician’s thought process in diagnosing the patient’s condition, managing their care, and determining the necessary tests and treatments.
In addition to these three, the “number of diagnoses or management options,” “amount and/or complexity of data to be reviewed and analyzed,” and “risk of complications and/or mortality or morbidity of patient management” were also considered, as was the “time spent” with the patient.
The Shift Towards Medical Decision Making and Time
More recent updates have placed a stronger emphasis on Medical Decision Making (MDM) as the primary driver for determining the E/M code level for most outpatient visits. While history and examination remain important components of patient care, the coding level is now largely dictated by the complexity of the MDM. This shift acknowledges that the cognitive effort involved in diagnosing and managing a patient’s condition is often the most resource-intensive aspect of an encounter.
Additionally, the “time” component has become a more prominent factor, particularly for certain types of visits. For visits where the physician or qualified healthcare professional spends the majority of their time in counseling and coordinating care, time can be used as the sole determinant for selecting the appropriate E/M code level. This recognizes that not all patient encounters are best measured by the complexity of the medical decision-making alone; sometimes, the depth of patient education and shared decision-making requires significant clinician time.
Understanding the Different E/M Code Categories
E/M codes are not a monolithic entity. They are further categorized based on the patient’s status and the setting in which the services are rendered. This segmentation allows for more precise billing and reflects the different complexities and resources required for various types of patient encounters.
New vs. Established Patient Encounters
A fundamental distinction in E/M coding is between “New Patients” and “Established Patients.”
-
New Patients: These are individuals who have not received any professional services from the physician or a qualified healthcare professional of the same specialty and subspecialty within the past three years. The initial encounter with a new patient typically involves a more comprehensive history and examination to establish a baseline understanding of their health.
-
Established Patients: These are individuals who have received professional services from the physician or a qualified healthcare professional of the same specialty and subspecialty within the past three years. For established patients, the focus is generally on the management of their current health status and the progression of existing conditions or the development of new issues.
The complexity and documentation requirements for E/M codes often differ between new and established patients, with new patients generally requiring a higher level of documentation for comparable services.
Outpatient vs. Inpatient Services
The setting of care significantly influences the applicable E/M codes.

-
Outpatient Services: This broad category encompasses visits to physician offices, hospital outpatient departments, and other ambulatory care settings. The E/M codes for outpatient services are further divided into several subcategories, including:
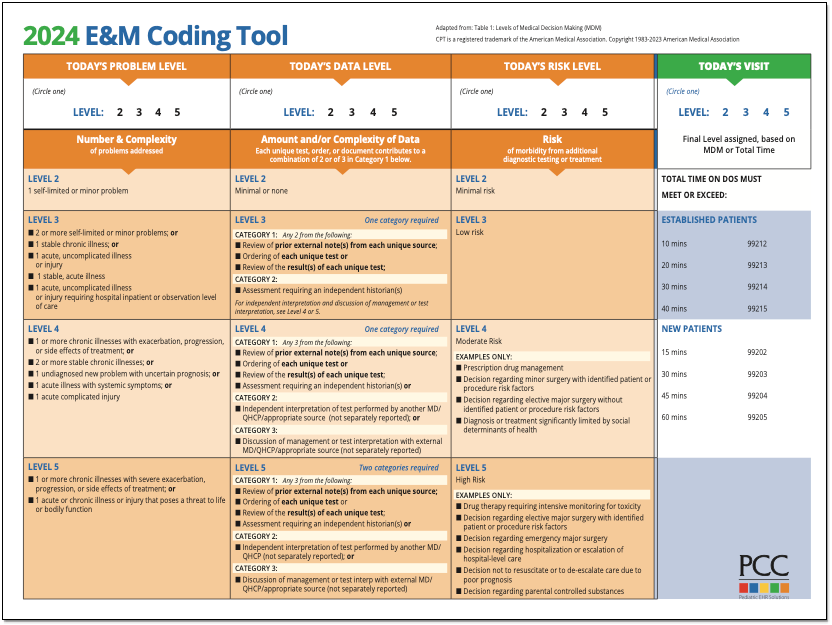
- Office or Other Outpatient Services (99202-99215): These are the most common E/M codes, used for routine office visits. The level of service (1-5) is determined by MDM or time.
- Observation Services: Codes used when a patient is admitted to a hospital for observation status, not yet formally admitted as an inpatient.
- Hospital Observation Services (99218-99220, 99224-99226): Used for initial and subsequent observation care.
- Emergency Department Services (99281-99285): Codes specific to evaluations and management in an emergency department setting.
-
Inpatient Services: These codes are used when a patient is formally admitted to a hospital for inpatient care. They reflect the increased complexity and intensity of services required for managing patients admitted to the hospital.
- Initial Hospital Care (99221-99223): For the first day of inpatient care.
- Subsequent Hospital Care (99231-99233): For subsequent days of inpatient care.
- Hospital Discharge Services (99238-99239): For the work involved in discharging a patient from the hospital.
Other Important E/M Categories
Beyond the primary distinctions, several other E/M code sets exist to capture specific types of encounters:
- Consultations (99446-99452): While often bundled or less frequently used due to payer policies, these codes were historically used when a physician requested the opinion and/or advice of another physician.
- Critical Care Services (99291-99292): These codes are for the evaluation and management of critically ill or injured patients in a dynamic life-threatening situation requiring immediate intervention.
- Prolonged Services (99354-99357): These codes are used in addition to other E/M codes when the physician spends an unusually long amount of time with a patient, providing direct patient contact beyond the typical duration for the E/M service.
- Care Management Services (99487, 99489, 99490, 99491): These codes are designed to capture the ongoing management of patients with chronic conditions, focusing on coordination of care, patient education, and monitoring.
Key Components for Determining E/M Code Level
As mentioned, the specific components used to determine the E/M code level vary slightly depending on the category of service and the applicable coding guidelines (e.g., the revised 2021 guidelines for office and outpatient visits). However, for many common encounters, the focus is on Medical Decision Making (MDM) and, in some cases, time.
Medical Decision Making (MDM)
MDM is assessed based on the number and complexity of problems addressed, the amount and/or complexity of data to be reviewed and analyzed, and the risk of complications and/or morbidity or mortality of patient management.
- Number and Complexity of Problems Addressed: This refers to the diagnoses or management options that the physician has to consider. A higher number of stable chronic illnesses, an acute illness with systemic symptoms, or an acute uncomplicated illness all contribute to the complexity.
- Amount and/or Complexity of Data to Be Reviewed and Analyzed: This includes reviewing and interpreting diagnostic test results (laboratory, radiology, pathology), discussing with another physician or qualified healthcare professional, and independently reviewing the patient’s old records.
- Risk of Complications and/or Morbidity or Mortality of Patient Management: This is assessed by the risks associated with the patient’s problems, the planned management (tests, procedures, medications), and the potential outcomes if management is delayed or not performed.
Each of these elements is assigned a level of complexity (e.g., straightforward, low, moderate, high). The highest level of MDM across the three elements dictates the overall MDM level, which then corresponds to a specific E/M code level (e.g., level 4 or 5).
Time
When time is used to determine the E/M code level (primarily for office and outpatient visits and sometimes for care management), it is defined as the total time spent by the physician and/or other qualified healthcare professional on the date of the encounter. This includes:
- Face-to-face time with the patient and/or family/caregiver.
- Non-face-to-face time spent performing activities related to the patient’s care, such as reviewing results, communicating with other providers, and documenting in the patient’s record.
- Time spent counseling and educating the patient.
It’s crucial to accurately document the total time spent and the activities performed to justify the selected code level based on time.

The Importance of Accurate E/M Coding
Accurate E/M coding is fundamental for several reasons:
- Reimbursement: Payers (like Medicare, Medicaid, and private insurance companies) use E/M codes to determine how much to reimburse healthcare providers for their services. Incorrect coding can lead to underpayment or overpayment, both of which can have significant financial implications for practices and health systems.
- Quality Reporting: E/M codes are used in various quality reporting programs that measure the effectiveness and efficiency of healthcare delivery. Accurate coding ensures that data used for these reports is reliable.
- Data Analysis and Research: The aggregated data from E/M codes provides valuable insights into healthcare utilization patterns, disease prevalence, and the types of services being delivered. This data is crucial for research, public health initiatives, and policy development.
- Compliance: Adhering to correct coding practices is a regulatory requirement. Billing for services that do not accurately reflect the work performed can result in audits, penalties, and even legal repercussions.
In conclusion, E/M codes are the sophisticated language of patient encounters in healthcare billing. They represent the intricate blend of clinical judgment, patient assessment, and management strategies employed by healthcare professionals. By understanding the structure, categories, and determining factors of E/M coding, providers can ensure accurate billing, contribute to robust healthcare data, and ultimately, maintain the financial health of their practices while focusing on delivering quality patient care.