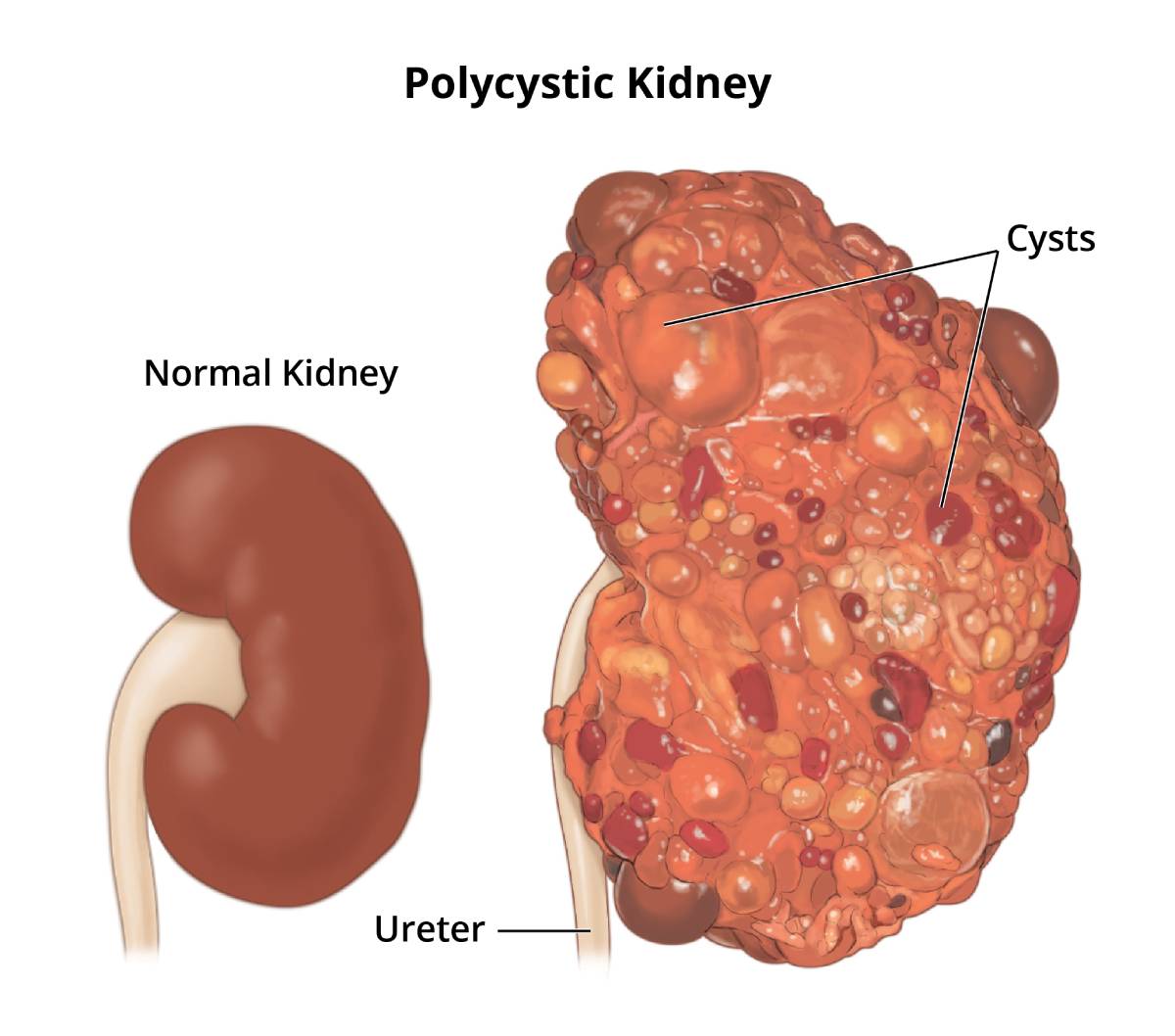
Autosomal Dominant Polycystic Kidney Disease (ADPKD) is a genetic disorder characterized by the development of numerous cysts in the kidneys. These cysts, fluid-filled sacs, can grow large enough to impair kidney function and lead to serious health complications. ADPKD is the most common inherited kidney disease, affecting approximately 1 in 500 to 1 in 1000 people worldwide. While it is a genetic condition, meaning it is passed down through families, the severity of the disease can vary significantly from person to person, even within the same family. Understanding ADPKD is crucial for early diagnosis, management, and the development of effective treatments.
The Genetic Basis of ADPKD
At its core, ADPKD is a disease of faulty genes. The condition is inherited in an autosomal dominant pattern, meaning that only one copy of the altered gene is needed for a person to develop the disease.
Gene Mutations and Protein Dysfunction
ADPKD is primarily caused by mutations in two genes: PKD1 and PKD2.
The Role of the PKD1 Gene
Mutations in the PKD1 gene are responsible for approximately 85% of ADPKD cases. The PKD1 gene provides instructions for making a protein called polycystin-1. This protein is thought to play a vital role in the development and function of the kidneys, particularly in the cells lining the renal tubules. Polycystin-1 is part of a complex that interacts with another protein, polycystin-2, encoded by the PKD2 gene. This complex is believed to be involved in sensing fluid flow and mechanical stress within the renal tubules, as well as in regulating calcium levels within cells. When the PKD1 gene is mutated, the polycystin-1 protein is either not produced, or it is produced in a form that is non-functional. This dysfunction disrupts normal kidney development and function, leading to the formation of cysts.
The Impact of the PKD2 Gene
Mutations in the PKD2 gene account for the remaining 15% of ADPKD cases. The PKD2 gene provides instructions for making a protein called polycystin-2. Polycystin-2 is a component of the same protein complex as polycystin-1 and acts as a channel that allows calcium to pass in and out of cells. When the PKD2 gene is mutated, the polycystin-2 protein is also non-functional, leading to similar cellular dysfunctions as seen with PKD1 mutations. While the overall disease presentation is similar between PKD1 and PKD2 mutations, patients with PKD1 mutations tend to develop more severe disease with an earlier onset and a faster progression towards kidney failure.
Inheritance Patterns and Familial Risk
The autosomal dominant inheritance pattern of ADPKD means that a child of an affected parent has a 50% chance of inheriting the gene mutation and developing the disease. This risk is independent of the sex of the parent or child. If a parent has ADPKD, each of their children has a 1 in 2 probability of having inherited the mutated gene. If an individual does not inherit the mutated gene from an affected parent, they will not develop ADPKD and cannot pass it on to their children. This contrasts with autosomal recessive conditions, where both parents must carry a mutated gene for their child to be affected.
The Pathophysiology of Cyst Formation
The hallmark of ADPKD is the development and growth of renal cysts. This process is complex and involves a cascade of cellular events triggered by the genetic mutations.
Early Cellular Changes
The initial cellular changes in ADPKD occur in the renal tubules, which are responsible for filtering waste products from the blood and producing urine. When polycystin-1 or polycystin-2 proteins are dysfunctional, several cellular processes go awry. These include:
- Aberrant Cell Proliferation: Cells lining the renal tubules begin to divide and multiply uncontrollably. This excessive proliferation contributes to the thickening of the tubule walls.
- Fluid Secretion: There is an increased secretion of fluid into the lumen of the renal tubules. This fluid accumulation further distends the tubules.
- Apoptosis Dysregulation: Apoptosis, or programmed cell death, is a normal process that is essential for tissue maintenance. In ADPKD, the regulation of apoptosis can be disrupted, leading to abnormal cell survival.
These combined cellular abnormalities lead to the formation of small, fluid-filled outpouchings from the renal tubules. These outpouchings are the nascent cysts.
Cyst Growth and Expansion
Once formed, these cysts do not remain static; they grow and expand over time. The mechanisms driving this expansion are multifaceted:
- Continued Cell Proliferation: The rate of cell division within the cyst lining remains elevated, adding more cells to the cyst wall.
- Increased Fluid Secretion: The cells within the cyst lining continue to secrete fluid into the cyst lumen. This fluid is rich in various electrolytes and organic molecules.
- Reduced Apoptosis: A lack of programmed cell death within the cyst wall allows the cyst to persist and enlarge.
- Inflammation: Chronic inflammation within the kidney tissue surrounding the cysts plays a role in their growth and in the overall progression of kidney damage. Inflammatory mediators can stimulate cell proliferation and contribute to tissue fibrosis.
As these cysts enlarge, they put pressure on the surrounding kidney tissue, compressing healthy nephrons (the functional units of the kidney). This compression can lead to the loss of functioning nephrons, gradually diminishing the kidney’s ability to filter waste products and maintain fluid and electrolyte balance.
Extratubular Manifestations
While the primary pathology of ADPKD is in the kidneys, cysts can also form in other organs. The most common extratubular manifestation is in the liver. Hepatic cysts are present in a significant proportion of individuals with ADPKD, particularly women, and can range from a few small cysts to hundreds of large ones, potentially leading to liver enlargement, pain, and impaired liver function. Cysts can also develop in the pancreas, spleen, and seminal vesicles, though these are less common and typically asymptomatic.
Clinical Manifestations and Complications
The clinical presentation of ADPKD can vary widely, with symptoms often not appearing until adulthood, typically between the ages of 30 and 60. The progression of the disease is also highly individualized.
Common Symptoms and Signs
The presence and growth of renal cysts lead to a range of symptoms and complications:
- Hypertension (High Blood Pressure): This is one of the earliest and most common complications of ADPKD, often preceding a significant decline in kidney function. The exact mechanisms are complex but are thought to involve the activation of the renin-angiotensin-aldosterone system due to changes in blood flow and sodium balance.
- Hematuria (Blood in the Urine): This can occur due to bleeding from cyst walls or urinary tract infections. It can be microscopic or gross, and often resolves spontaneously.
- Flank Pain or Abdominal Pain: This is frequently caused by enlarged cysts, bleeding into cysts, kidney stones, or urinary tract infections. The pain can be acute and severe or chronic and dull.
- Kidney Stones: Individuals with ADPKD have a higher risk of developing kidney stones, which can cause significant pain and obstruct urine flow.
- Urinary Tract Infections (UTIs): Cysts can provide a breeding ground for bacteria, making UTIs more frequent and potentially more severe. Infected cysts can lead to fever, chills, and intense pain.
- Loss of Kidney Function (Chronic Kidney Disease – CKD): As cysts enlarge and damage nephrons, the kidneys’ ability to filter waste products and regulate bodily fluids declines. This progression leads to CKD, which can eventually necessitate dialysis or kidney transplantation.
Other Potential Complications
Beyond the direct effects of renal cysts, ADPKD is associated with several other serious health issues:
- Cerebral Aneurysms: There is an increased risk of developing aneurysms (weakened areas in blood vessel walls) in the arteries of the brain. These aneurysms can rupture, leading to a subarachnoid hemorrhage, a life-threatening condition. Screening for brain aneurysms is often recommended for individuals with a family history of ADPKD or a personal history of certain complications.
- Cardiovascular Disease: Individuals with ADPKD have a higher risk of heart valve abnormalities, such as mitral valve prolapse, and other cardiovascular issues, including aortic aneurysms.
- Diverticula: Outpouchings in the colon (diverticula) are more common in people with ADPKD, particularly in the sigmoid colon. These can lead to complications such as diverticulitis.
Diagnosis and Management of ADPKD
Early diagnosis and proactive management are critical for slowing the progression of ADPKD and improving the quality of life for affected individuals.
Diagnostic Approaches
The diagnosis of ADPKD typically involves a combination of medical history, physical examination, and imaging studies.
- Family History: A thorough family history is essential, as ADPKD is a hereditary condition. Identifying affected relatives can raise suspicion.
- Imaging Studies:
- Ultrasound: Renal ultrasound is often the initial imaging modality. It can detect kidney enlargement and the presence of multiple cysts, typically when cysts have grown to a certain size. It is non-invasive and widely accessible.
- CT Scan and MRI: Computed Tomography (CT) scans and Magnetic Resonance Imaging (MRI) provide more detailed images of the kidneys and can detect smaller cysts or assess the extent of cyst involvement and other potential complications such as aneurysms.
- Genetic Testing: In some cases, particularly when imaging is inconclusive or in individuals considering family planning, genetic testing for mutations in PKD1 or PKD2 can confirm the diagnosis.
Current Management Strategies
There is currently no cure for ADPKD, but management focuses on slowing disease progression, alleviating symptoms, and preventing complications.
- Blood Pressure Control: Aggressive management of hypertension is paramount. Medications such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are often the first-line treatments, as they not only lower blood pressure but also have been shown to reduce cyst growth and preserve kidney function.
- Pain Management: Treatment for pain varies depending on the cause and severity. This can include over-the-counter pain relievers, prescription medications, and in severe cases, procedures to address complications like infected cysts or bleeding.
- Hydration: Maintaining adequate fluid intake is important. While the exact mechanism is not fully understood, some studies suggest that high water intake may help slow cyst growth by reducing vasopressin levels, which are thought to stimulate cyst formation.
- Dietary Modifications: A healthy diet low in sodium is recommended to help manage blood pressure.
- Monitoring and Screening: Regular monitoring of kidney function, blood pressure, and screening for complications like brain aneurysms are essential components of care.
- Tolvaptan: In recent years, tolvaptan has emerged as the first medication approved to specifically slow cyst growth and preserve kidney function in adults with moderate to rapidly progressing ADPKD. Tolvaptan works by blocking the action of vasopressin, a hormone that plays a role in cyst formation and growth.

Future Directions and Research
Research into ADPKD is ongoing, with a focus on understanding the underlying molecular mechanisms of cystogenesis and developing novel therapeutic strategies. This includes exploring targeted therapies that address specific cellular pathways involved in cyst growth, as well as potential gene therapies to correct the underlying genetic defects. The goal is to find more effective ways to halt or even reverse the progression of this debilitating disease.