The world of reconstructive surgery is constantly evolving, offering innovative solutions for individuals who have undergone mastectomies or experienced significant tissue loss due to trauma or other medical conditions. Among these advanced techniques, the DIEP (Deep Inferior Epigastric Perforator) flap procedure stands out as a remarkable achievement in breast reconstruction, offering a natural and aesthetically pleasing outcome. This surgical marvel leverages a patient’s own abdominal tissue to rebuild the breast mound, providing a durable and integrated solution that mimics the original anatomy. Understanding the intricacies of the DIEP flap is crucial for anyone considering breast reconstruction, as it represents a significant advancement in the field, prioritizing both form and function.
The Science Behind the DIEP Flap: Autologous Reconstruction
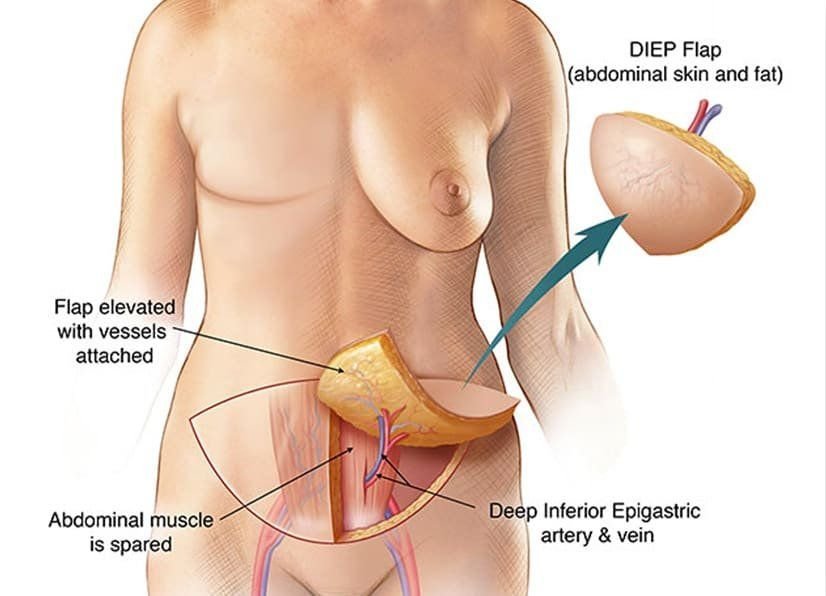
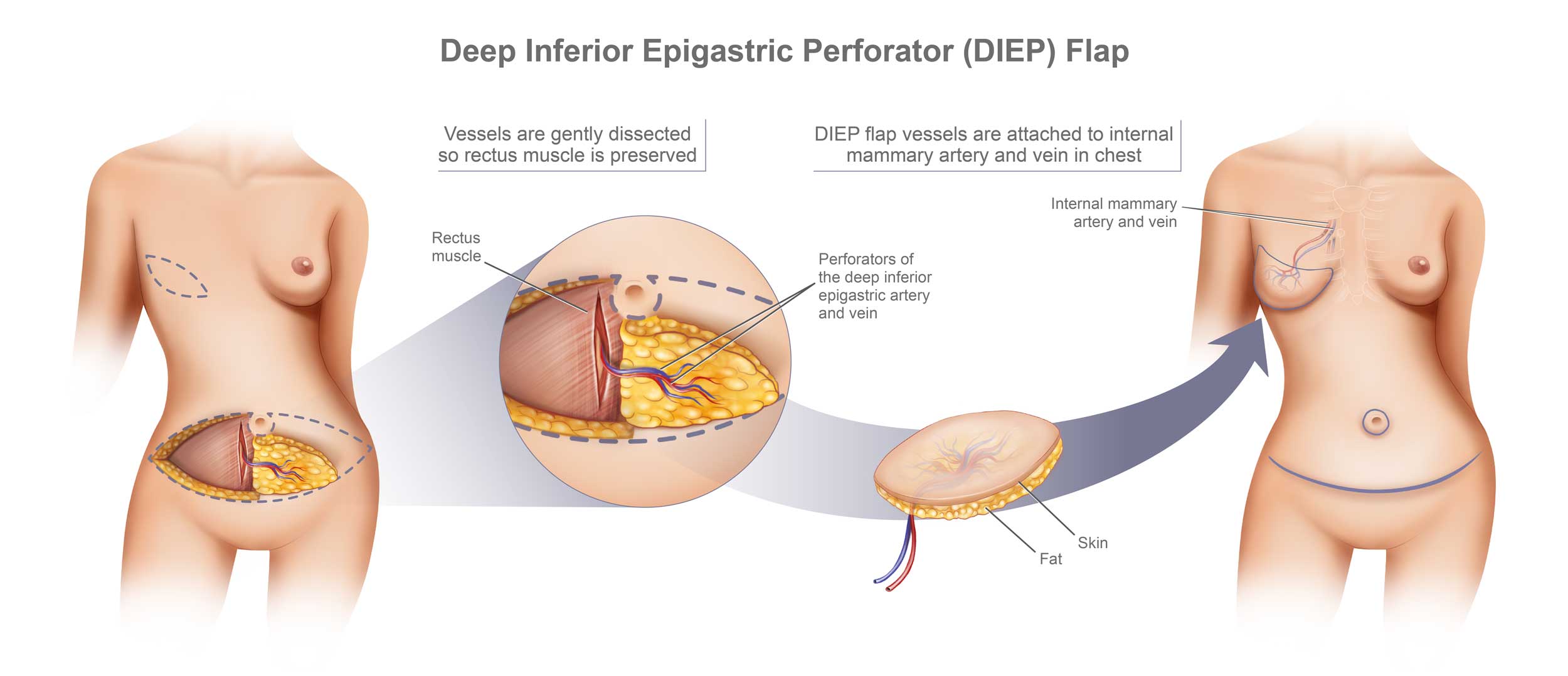
The core principle of the DIEP flap lies in its autologous nature, meaning it utilizes the patient’s own body tissues. This differentiates it from implant-based reconstructions, which involve foreign materials that can sometimes lead to complications or require eventual replacement. The DIEP flap specifically harvests skin, fat, and the blood vessels that supply this tissue from the lower abdomen. The key to the DIEP flap’s success is the meticulous dissection and preservation of the deep inferior epigastric perforator vessels. These are small arteries and veins that pass through the rectus abdominis muscle (the “six-pack” muscle) to nourish the overlying abdominal tissue.
Harvesting the Abdominal Tissue: A Delicate Dissection
The surgical team begins by carefully mapping out the perforator vessels in the patient’s abdomen. This often involves advanced imaging techniques to ensure precise identification and planning. Once the optimal perforators are identified, the surgeon embarks on a highly delicate dissection. The goal is to isolate a sufficient amount of skin and fat, along with these crucial blood vessels, without compromising the integrity of the rectus abdominis muscle. This is a critical distinction from older flap techniques, such as the TRAM (Transverse Rectus Abdominis Myocutaneous) flap, which often involved sacrificing a significant portion of the rectus muscle. By preserving the muscle, the DIEP flap offers several advantages, including improved abdominal wall strength and a reduced risk of hernia formation. The harvested abdominal tissue is then carefully shaped to resemble the natural contour of a breast.
Microsurgical Anastomosis: Reconnecting the Blood Supply
The most technically demanding aspect of the DIEP flap procedure is the microsurgical anastomosis, or connection, of the harvested perforator vessels to recipient blood vessels in the chest wall. This requires the expertise of a skilled microsurgeon who can use specialized instruments and a microscope to meticulously suture the tiny arteries and veins. The harvested flap needs to be revascularized, meaning its blood supply must be re-established to ensure the survival of the transplanted tissue. The artery of the flap is connected to an artery in the chest, and the vein of the flap is connected to a vein in the chest. This intricate reconnection is vital for the long-term success of the reconstruction, allowing the flap to receive oxygenated blood and nutrients and to drain deoxygenated blood, thereby preventing tissue necrosis. The success of this anastomosis is closely monitored throughout the surgery and in the immediate post-operative period.
Advantages of the DIEP Flap
The DIEP flap offers a multitude of advantages that have made it a gold standard in autologous breast reconstruction. Primarily, it provides a very natural feel and appearance. Because it uses the patient’s own tissue, the reconstructed breast is soft, warm, and moves with the body, closely resembling a natural breast. Furthermore, the reconstruction is permanent and does not require future replacements, unlike breast implants which can rupture, deflate, or require revision surgery over time. The abdominal tissue used for the flap is essentially a “free” flap, meaning it is completely detached from its original blood supply and reattached in a new location. This “free” nature contributes to its excellent blood supply and viability.
Another significant benefit is the simultaneous improvement of the abdominal contour. Since excess skin and fat are removed from the abdomen to create the flap, patients often experience a flattening of their abdominal wall, akin to a tummy tuck. This dual benefit of breast reconstruction and abdominal rejuvenation is a highly attractive aspect of the DIEP flap for many patients. The long-term durability of the DIEP flap is also a key advantage. Unlike implants that can change over time, the DIEP flap is living tissue that will age with the rest of the body. This means the reconstructed breast will naturally change in size and shape as the patient gains or loses weight, maintaining a more consistent and natural look.
The Patient Journey: From Consultation to Recovery
Undergoing a DIEP flap procedure is a significant undertaking, and the patient journey involves several distinct phases, each requiring careful attention and planning. The process begins long before the surgery itself and extends well into the recovery period.
Initial Consultation and Candidacy Assessment
The first step for any patient considering breast reconstruction is a thorough consultation with a plastic surgeon specializing in reconstructive surgery. During this initial meeting, the surgeon will discuss the patient’s medical history, assess their overall health, and review their reasons for seeking reconstruction. For the DIEP flap, specific criteria are evaluated to determine candidacy. This includes the availability of adequate abdominal tissue, the presence of healthy perforator vessels, and the absence of certain medical conditions that could compromise surgical outcomes, such as significant vascular disease or uncontrolled diabetes. The surgeon will explain the procedure in detail, outline the potential benefits and risks, and answer all of the patient’s questions. Realistic expectations will be set regarding the aesthetic outcome and the recovery process.
Surgical Procedure and Hospital Stay
The DIEP flap surgery is a complex procedure that typically takes several hours to complete, often performed by a team of highly trained microsurgeons. Patients will remain in the hospital for a period of several days following the surgery, allowing for close monitoring of the flap’s viability and management of pain. During this time, nurses and medical staff will carefully assess the color, temperature, and capillary refill of the reconstructed breast to ensure adequate blood flow. Patients will also receive pain medication and be advised on early mobilization to prevent complications such as blood clots. The abdominal donor site will be closed, and a drain may be placed to manage fluid accumulation.
![]()
Post-Operative Recovery and Rehabilitation
The recovery period after a DIEP flap is a gradual process that requires patience and adherence to the surgeon’s instructions. Immediately after surgery, patients will experience some discomfort and swelling in both the breast and abdominal areas. It is crucial for patients to avoid strenuous activity and heavy lifting for several weeks to allow the tissues to heal properly. Gentle movement and stretching will be encouraged to regain mobility and prevent stiffness.
The surgical team will schedule regular follow-up appointments to monitor the healing progress, remove any drains, and assess the flap’s integration. Patients may be advised to wear a supportive bra to aid in healing and provide comfort. As the swelling subsides and the tissues mature, the reconstructed breast will begin to take on its final shape. Over time, sensation may return to the reconstructed breast, although it may differ from the original sensation. The abdominal scar will also gradually fade.
Long-Term Outcomes and Potential Adjustments
The long-term outcomes of a DIEP flap are generally excellent, with most patients reporting high satisfaction with their reconstructed breasts. The reconstructed breast is living tissue and will change with the patient’s body weight, just like a natural breast. Some patients may opt for nipple and areola reconstruction, which can be performed as a separate procedure once the initial breast reconstruction has healed. This can be achieved through tattooing or further surgical techniques.
While the DIEP flap is a highly successful procedure, like any surgery, there are potential long-term considerations. Over time, some degree of asymmetry might develop, or changes in breast shape may occur due to weight fluctuations or aging. In such cases, minor adjustments or touch-up procedures may be considered. However, the fundamental advantage of using one’s own living tissue for reconstruction ensures a durable and aesthetically pleasing result that can last a lifetime. The DIEP flap represents a significant leap forward in breast reconstruction, offering hope and renewed confidence to individuals navigating the challenges of mastectomy.
Alternatives and Considerations
While the DIEP flap is a highly regarded option, it is not the sole solution for breast reconstruction. Understanding the alternatives and the specific considerations associated with the DIEP flap can help patients make informed decisions that best align with their individual needs and circumstances.
Implant-Based Reconstruction
Implant-based breast reconstruction is another common approach. This method involves using silicone or saline implants to create the breast mound. There are two main types: immediate reconstruction, performed at the time of mastectomy, and delayed reconstruction, performed months or years after mastectomy. Often, a tissue expander is used initially to gradually stretch the skin and muscle before an implant is placed.
- Pros: Generally a shorter surgical procedure with a potentially quicker initial recovery compared to flap procedures.
- Cons: Implants are foreign bodies and can lead to complications such as capsular contracture, rupture, infection, or rippling. They may also require revision surgery or replacement over time. The feel and movement of the breast can be less natural than with autologous tissue.
Other Autologous Flaps
Beyond the DIEP flap, other autologous flap procedures utilize a patient’s own tissue. These include:
- TRAM (Transverse Rectus Abdominis Myocutaneous) Flap: Similar to the DIEP flap, this also uses abdominal tissue. However, older TRAM flap techniques often involved taking a portion of the rectus abdominis muscle along with the skin and fat. This can lead to a weaker abdominal wall and a higher risk of hernias. Variations like the pedicled TRAM flap still connect the tissue to the chest via its original blood supply, while free TRAM flaps involve reconnecting blood vessels, similar to the DIEP flap, but with muscle involvement.
- SIEA (Superficial Inferior Epigastric Artery) Flap: This flap also uses abdominal tissue but relies on superficial blood vessels rather than the deeper perforators. It is less commonly performed than the DIEP flap because the blood supply can sometimes be less robust, and not all patients have suitable superficial vessels.
- Other Body Site Flaps (e.g., Gluteal, Thigh): For patients without sufficient abdominal tissue, flaps can be harvested from other areas of the body, such as the buttocks (SGAP/IGAP flap) or the inner thigh (TUG/TBP flap). These procedures also involve microsurgical techniques to revascularize the flap.
Factors Influencing DIEP Flap Candidacy
While the DIEP flap offers numerous benefits, certain factors can make a patient unsuitable for this procedure:
- Insufficient Abdominal Tissue: Patients who have undergone previous abdominal surgeries that have damaged the perforator vessels or removed too much abdominal tissue may not be ideal candidates.
- Previous Abdominal Surgery: Extensive prior surgeries in the abdominal region, such as multiple C-sections or abdominoplasties, can potentially compromise the blood supply to the abdominal flap.
- Smoking: Smoking significantly impairs circulation and wound healing, increasing the risk of flap failure. Surgeons typically require patients to quit smoking well in advance of the surgery.
- Certain Medical Conditions: Conditions like uncontrolled diabetes, peripheral vascular disease, or severe obesity can increase surgical risks.
- Radiation Therapy: While not an absolute contraindication, prior radiation to the chest area can sometimes affect the recipient blood vessels, requiring careful assessment.
The decision to pursue a DIEP flap is a personal one, best made in consultation with a qualified plastic surgeon. A comprehensive discussion of all available options, coupled with a thorough evaluation of the patient’s individual anatomy and medical history, will guide the selection of the most appropriate and effective reconstructive approach.