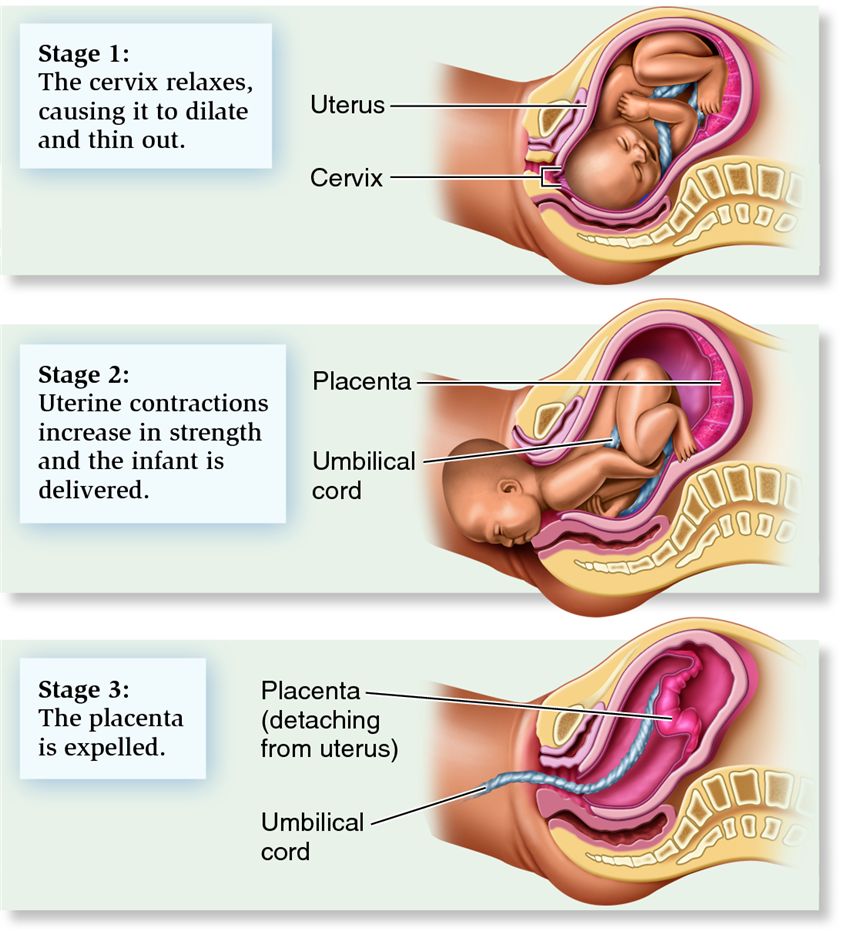
The journey of childbirth is often depicted as a dramatic and swift event, but it is, in reality, a complex and multi-phased process. While the first and second stages – labor and birth – receive the most attention, the third stage of labor is equally vital for both the mother’s and the baby’s well-being. This crucial phase, often overlooked in popular narratives, involves the delivery of the placenta, also known as the afterbirth. Understanding this stage is paramount for expectant parents and healthcare providers alike, as it marks the completion of the birthing process and initiates the mother’s recovery.

The Crucial Role of the Placenta
Before delving into the intricacies of the third stage of labor, it is essential to appreciate the profound significance of the placenta throughout pregnancy. This remarkable organ, which grows and develops within the uterus during gestation, serves as the lifeline between the mother and the fetus. Its primary functions include:
- Nutrient and Oxygen Exchange: The placenta facilitates the transfer of oxygen and vital nutrients from the mother’s bloodstream to the baby. Simultaneously, it removes waste products, such as carbon dioxide and urea, from the baby’s blood and transfers them back to the mother for elimination.
- Hormone Production: The placenta is a temporary endocrine gland, producing hormones essential for maintaining the pregnancy. These include progesterone, which helps to relax the uterine muscles and prevent premature contractions, and estrogen, which supports the growth of the uterus and mammary glands.
- Immune System Support: The placenta provides a barrier against certain infections and transfers antibodies from the mother to the baby, offering passive immunity that protects the newborn during the early months of life.
The placenta is a highly vascularized organ, intricately connected to the uterine wall via the umbilical cord. Upon the birth of the baby, its primary role is fulfilled, and it is then expelled from the uterus. This expulsion process constitutes the third stage of labor.
Initiating the Third Stage: The Placental Separation
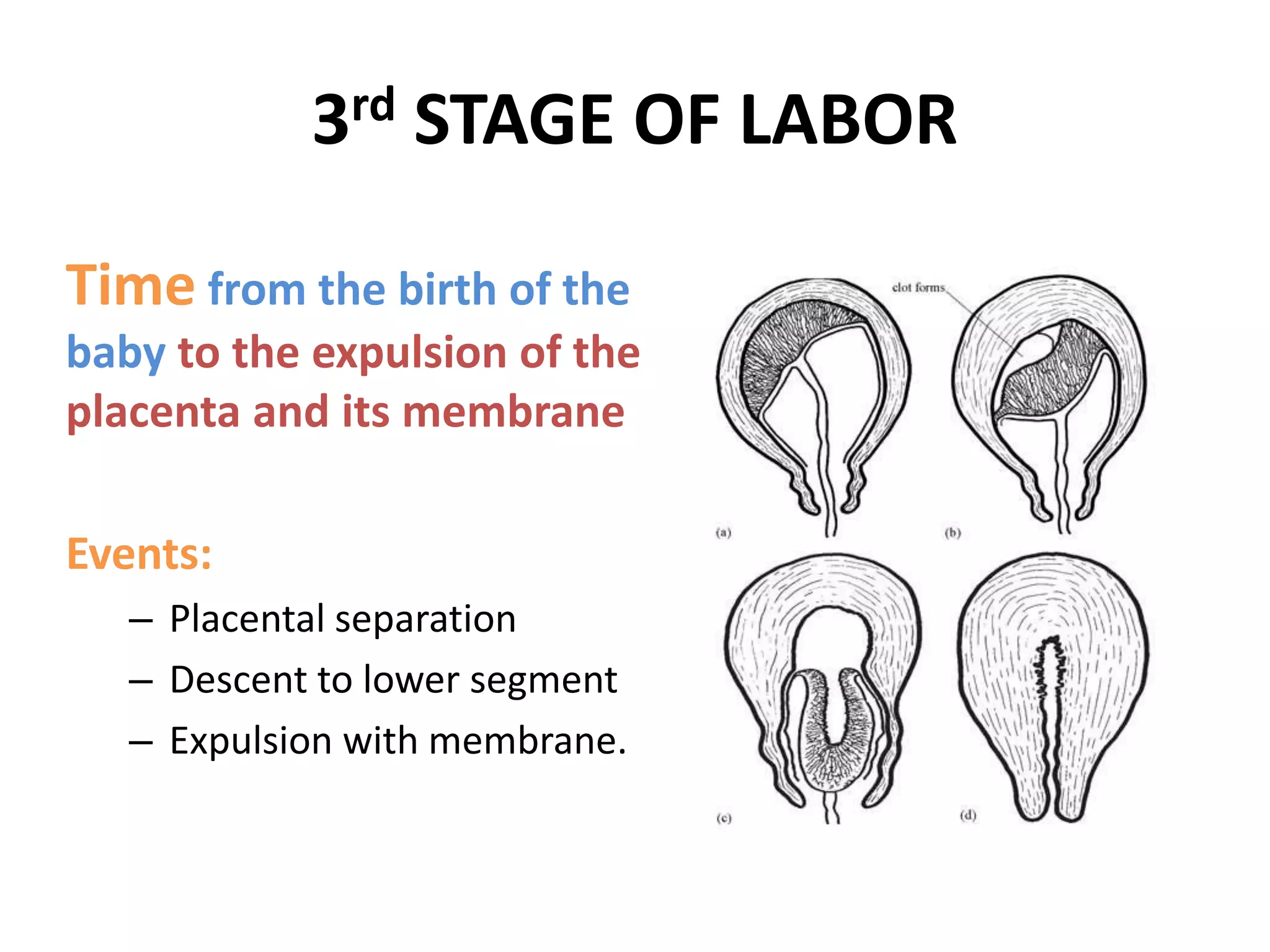
Once the baby has been born and the umbilical cord has typically been clamped and cut, the uterus, which has been contracting throughout labor to expel the baby, continues to contract. These post-birth contractions are smaller and less intense than those experienced during active labor, but they are crucial for the safe detachment and delivery of the placenta.
Physiological Mechanisms of Separation
The separation of the placenta from the uterine wall is a natural physiological process. Several mechanisms contribute to this detachment:
- Uterine Contractions: As the uterus contracts, it decreases in size. This reduction in the uterine cavity puts pressure on the placenta, which is no longer as intimately attached. The myometrium (the muscular layer of the uterus) contracts and retracts, effectively squeezing the placental site and leading to separation.
- Reduced Blood Volume: With the baby delivered, the placental circulation drastically reduces. The volume of blood within the placenta decreases, making it more pliable and susceptible to detachment.
- Hematoma Formation: As the placental villi begin to pull away from the uterine decidua (the inner lining of the uterus), small bleeds can occur. These bleeds form a hematoma (a collection of blood) behind the placenta, further aiding its separation from the uterine wall.
The onset of placental separation is typically indicated by physical signs that are closely monitored by healthcare providers. These signs, often referred to as “signs of placental separation,” usually appear within 5 to 30 minutes after the baby’s birth.
Signs of Placental Separation
Healthcare professionals are trained to recognize these key indicators, which suggest that the placenta is ready to be delivered:
- Changes in the Uterus: The uterus, which may have been soft and somewhat flaccid immediately after birth, begins to firm up and become more globular. It typically rises in the abdomen.
- Lengthening of the Umbilical Cord: If the umbilical cord is still attached and exposed, a healthcare provider may observe that it visibly lengthens as it protrudes further from the vagina.
- Gush of Blood: A moderate gush of blood may be seen as the placenta begins to separate. This is a sign that the placental site is no longer sealed by the placenta.
- Ballottement of the Uterus: When the provider presses on the upper part of the uterus, it may feel as if the placenta is floating and can be pushed back up into the uterus, indicating it has detached.
These signs are carefully observed to ensure that the placenta is separating correctly and to prevent potential complications such as retained placenta.
The Delivery of the Placenta
Once signs of placental separation are evident, the healthcare provider will assist in the delivery of the placenta. This process can occur spontaneously with further uterine contractions, or it may require gentle assistance.
Active Management of the Third Stage (AMTS)
In many modern obstetric settings, Active Management of the Third Stage (AMTS) is the standard of care. AMTS involves a set of interventions designed to expedite the delivery of the placenta and minimize the risk of excessive bleeding (postpartum hemorrhage). Key components of AMTS include:
- Administration of Uterotonics: A common intervention is the administration of a uterotonic medication, such as oxytocin (often given intramuscularly or intravenously shortly after the baby’s birth). Uterotonics stimulate stronger and more frequent uterine contractions, which help to expel the placenta efficiently and constrict blood vessels at the placental site, reducing bleeding.
- Controlled Cord Traction (CCT): This technique involves applying gentle, controlled traction to the umbilical cord while simultaneously supporting the uterus. The aim is to guide the placenta out of the uterus without causing excessive trauma to the mother or tearing the cord. CCT is usually initiated once clear signs of placental separation are observed.
- Uterine Massage: Following the delivery of the placenta, the uterus is typically massaged vigorously to encourage it to contract firmly and remain so. This helps to prevent secondary bleeding.
Physiological Management of the Third Stage
In some circumstances, particularly in low-risk pregnancies where the mother desires a more natural approach and there are no immediate concerns for excessive bleeding, physiological management may be employed. This approach relies primarily on the mother’s body to deliver the placenta with minimal intervention. Interventions are only introduced if there are signs of prolonged third stage or excessive bleeding. This might involve:
- Delayed Cord Clamping: While not directly part of placental delivery, delayed cord clamping is a common practice in physiological management and can allow for continued transfer of blood from the placenta to the baby.
- Waiting for Spontaneous Expulsion: The mother is allowed to rest and her body is permitted to expel the placenta naturally with the help of uterine contractions.
- Gentle Fundal Pressure: If needed, gentle upward pressure on the uterus (fundal pressure) may be applied to assist expulsion once separation has occurred.
The choice between AMTS and physiological management is typically discussed with the expectant parents during prenatal care, taking into account their preferences, medical history, and the specific circumstances of the birth.
Post-Delivery Examination and Potential Complications
Once the placenta has been delivered, it is crucial for the healthcare provider to examine it thoroughly. This examination serves two important purposes:
- Confirmation of Completeness: The placenta should be intact. Healthcare providers will inspect it to ensure that all of its lobes are present and that no fragments have been retained within the uterus. A retained placental fragment can lead to serious complications, including infection and heavy bleeding.
- Assessment of Fetal Well-being: The appearance of the placenta can sometimes offer clues about the health of the pregnancy and the fetus. Any abnormalities in its structure, such as calcifications or infarcts, might be noted.
Complications of the Third Stage
While the third stage of labor is generally safe and uneventful, there are potential complications that can arise:
- Retained Placenta: This occurs when the placenta does not detach or deliver within a reasonable timeframe (typically after 30 minutes to an hour after the baby’s birth). It can be caused by a failure of the placental muscles to contract effectively, or if the placenta is abnormally attached to the uterine wall. Management may involve manual removal of the placenta by the healthcare provider or, in some cases, a surgical procedure.
- Postpartum Hemorrhage (PPH): This is the most significant risk associated with the third stage of labor, defined as excessive bleeding from the uterus after childbirth. PPH can occur if the uterus does not contract adequately after the placenta has delivered (uterine atony), if there are tears or lacerations in the birth canal that were not repaired, or if placental fragments are retained. AMTS, particularly the use of uterotonics and controlled cord traction, is designed to minimize the risk of PPH.
- Inversion of the Uterus: This is a rare but serious complication where the uterus turns inside out. It can happen spontaneously or as a result of excessive traction on the umbilical cord before the placenta has separated. It requires immediate medical intervention.
- Placenta Accreta Spectrum: This is a condition where the placenta attaches too deeply into the uterine wall. It can lead to severe bleeding during or after delivery and often requires a hysterectomy. While typically identified during pregnancy through imaging, it can present as a complication of the third stage if not previously diagnosed.
The Significance of the Third Stage for Recovery
The successful and complete delivery of the placenta is not merely the end of a phase; it is the crucial first step in the mother’s postpartum recovery. As the uterus contracts down, it begins to seal the blood vessels that were attached to the placenta, significantly reducing the risk of hemorrhage. The uterus also gradually returns to its pre-pregnant state, a process known as involution.
The third stage of labor is a testament to the body’s remarkable capacity for healing and adaptation. By understanding its processes, the signs to look for, and the potential complications, expectant parents can feel more informed and empowered as they navigate the incredible journey of bringing new life into the world. This often-unsung stage is a vital component of a healthy birth and a smooth transition into motherhood.