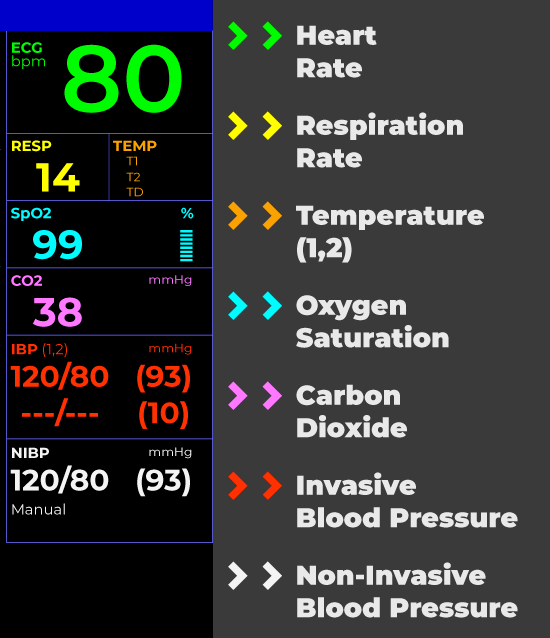
The acronym “RR” on a hospital monitor is a crucial indicator, and understanding its meaning is fundamental for healthcare professionals and informed patients alike. It stands for Respiratory Rate, which is the number of breaths a person takes per minute. This vital sign provides critical insights into the functioning of the respiratory system, a complex network responsible for the exchange of gases essential for life. Beyond a simple count, RR reflects the body’s ability to oxygenate the blood and eliminate carbon dioxide, processes that are meticulously regulated and highly sensitive to a wide array of physiological and pathological changes.

The respiratory system’s intricate dance of inhalation and exhalation is a finely tuned process, orchestrated by a sophisticated interplay of neurological signals, muscular activity, and mechanical principles. When this delicate balance is disrupted, the respiratory rate can deviate significantly from its normal range, signaling potential underlying health issues that demand immediate attention. Monitoring RR is therefore not merely a routine procedure; it is a cornerstone of patient assessment, diagnostic evaluation, and therapeutic management across a vast spectrum of medical conditions, from the acute emergencies of respiratory failure to the chronic complexities of pulmonary diseases.
The Physiology of Respiration and Normal Ranges
To fully appreciate the significance of RR on a hospital monitor, it is imperative to delve into the underlying physiology of respiration. The process begins in the brain, specifically in the respiratory centers located in the brainstem. These centers receive information from various sensors throughout the body, including chemoreceptors that detect levels of carbon dioxide and oxygen in the blood, as well as mechanoreceptors in the lungs and chest wall that monitor lung volume and airflow. Based on this information, the brainstem generates signals that travel down to the respiratory muscles, primarily the diaphragm and the intercostal muscles, prompting them to contract and relax.
During inhalation, the diaphragm contracts and flattens, while the intercostal muscles contract, lifting the rib cage upwards and outwards. This action increases the volume of the thoracic cavity, leading to a decrease in pressure within the lungs relative to the atmospheric pressure. As a result, air rushes into the lungs, a process known as inspiration. Exhalation, on the other hand, is typically a passive process at rest. The diaphragm and intercostal muscles relax, causing the thoracic cavity to decrease in volume. This increases the pressure within the lungs, forcing air out. During forceful exhalation, accessory muscles of respiration can be recruited to further expel air.
The normal respiratory rate varies depending on age and activity level. For adults at rest, a typical RR falls between 12 and 20 breaths per minute. Infants have a higher normal RR, often between 30 and 60 breaths per minute, reflecting their smaller lung capacity and higher metabolic rate. As children grow, their respiratory rate gradually decreases, approaching adult values by adolescence. Factors such as fever, pain, anxiety, and physical exertion can temporarily increase the RR. Conversely, certain medications, such as opioids, can suppress the respiratory drive and lower the RR.
The numerical value displayed for RR on a hospital monitor represents the number of complete breathing cycles—one inhalation followed by one exhalation—observed over a one-minute period. This measurement is usually obtained through various monitoring devices, including pulse oximeters that often incorporate a respiratory rate sensor, or through direct observation by trained healthcare personnel. The accuracy and consistency of this measurement are paramount, as even subtle deviations can herald significant physiological changes.
Interpreting Deviations: Tachypnea and Bradypnea
When the respiratory rate deviates from the normal range, it is categorized as either tachypnea or bradypnea. Tachypnea refers to an abnormally rapid breathing rate, typically exceeding 20 breaths per minute in adults. This can be a sign of the body attempting to compensate for various physiological insults. For instance, in conditions like pneumonia or acute respiratory distress syndrome (ARDS), the lungs may be inflamed or filled with fluid, impairing gas exchange. The body responds by increasing the breathing rate in an effort to bring in more oxygen and expel more carbon dioxide, thereby trying to maintain adequate oxygenation.
Other common causes of tachypnea include fever, where an elevated body temperature increases the metabolic rate and consequently the demand for oxygen, leading to increased respiratory effort. Pain, especially severe pain, can also stimulate the respiratory centers and cause rapid breathing. Anxiety and panic attacks are well-known triggers for tachypnea, often accompanied by hyperventilation, where the breathing rate and depth are significantly increased, leading to a decrease in carbon dioxide levels in the blood.
Cardiovascular conditions can also manifest as tachypnea. In heart failure, the heart’s inability to pump blood effectively can lead to fluid accumulation in the lungs (pulmonary edema), making breathing difficult and causing an increased respiratory rate. Metabolic acidosis, a condition where the body’s pH becomes too acidic, can also trigger tachypnea as the respiratory system attempts to blow off excess carbon dioxide, which acts as an acid in the blood. This compensatory mechanism is known as Kussmaul breathing, characterized by deep, rapid respirations.
Conversely, bradypnea is defined as an abnormally slow breathing rate, typically below 12 breaths per minute in adults. This can be a more concerning sign as it suggests a diminished respiratory drive or impairment in the mechanics of breathing. Opioid overdose is a classic cause of bradypnea, as these medications suppress the central nervous system’s respiratory centers, leading to dangerously slow and shallow breaths. Other central nervous system depressants, such as sedatives and anesthetics, can also induce bradypnea.
Hypothyroidism, a condition where the thyroid gland produces insufficient thyroid hormones, can lead to a slowed metabolism and, consequently, a reduced respiratory rate. Severe hypothermia, or dangerously low body temperature, can also depress respiratory function. In certain neurological conditions, such as brain injuries or strokes affecting the brainstem, the respiratory control centers can be damaged, leading to bradypnea. Obstructive sleep apnea, a condition where breathing repeatedly stops and starts during sleep, can sometimes be associated with episodes of bradypnea between apneic events.
The presence of tachypnea or bradypnea on a hospital monitor is a significant alert that necessitates a thorough clinical evaluation to identify the underlying cause. Prompt diagnosis and intervention are crucial to prevent complications and improve patient outcomes.
Factors Influencing Respiratory Rate Monitoring
The accurate and reliable monitoring of respiratory rate on a hospital monitor is influenced by a multitude of factors, ranging from the sophistication of the monitoring technology to the physiological state of the patient and the environmental conditions. Healthcare providers must be acutely aware of these influencing factors to ensure the data they are interpreting is as precise as possible.
Technological Considerations
The method used to measure RR can significantly impact its accuracy. Manual counting by healthcare professionals, while foundational, is prone to subjective error and variability, especially during periods of irregular breathing. Modern hospital monitors often employ sophisticated technologies to automate RR measurement. These can include:
- Impedance Pneumography: This method uses electrodes placed on the patient’s chest to measure subtle changes in electrical impedance caused by the expansion and contraction of the chest wall during breathing. It is commonly integrated into electrocardiogram (ECG) leads.
- Capnography: This technology measures the concentration of carbon dioxide in the exhaled breath (end-tidal carbon dioxide, or EtCO2). The waveform generated by capnography directly reflects the breathing cycle, allowing for accurate RR calculation. It is considered one of the most reliable methods for RR monitoring, particularly in critically ill patients.
- Acoustic Monitoring: Some advanced systems use microphones to detect the sounds of airflow and breathing.
- Sensor Integration with Pulse Oximeters: Many pulse oximeters now incorporate a plethysmographic variability index that correlates with respiratory rate, offering a non-invasive estimation.

Each of these technologies has its strengths and limitations. For instance, impedance pneumography can be affected by patient movement or changes in electrode contact. Capnography, while highly accurate, requires an airway connection and may not be suitable for all patients. The selection of the appropriate monitoring technology often depends on the patient’s clinical condition, the criticality of their status, and the specific monitoring goals. Regular calibration and maintenance of these devices are paramount to ensure ongoing accuracy.
Patient-Specific Factors
The inherent physiological characteristics of the patient play a pivotal role in RR monitoring.
- Breathing Pattern Irregularities: Conditions that cause irregular breathing patterns, such as Cheyne-Stokes respiration (alternating periods of apnea and hyperpnea) or ataxic breathing, can make automated RR counting challenging. Healthcare providers may need to intervene with manual counts or rely on specialized algorithms designed to interpret such patterns.
- Patient Movement and Artifacts: Fidgeting, coughing, or intentional breath-holding can create artifacts that interfere with the sensor’s ability to accurately detect breaths, leading to erroneous readings. Strategies to minimize movement and distinguish true breaths from artifacts are essential.
- Underlying Medical Conditions: As discussed, conditions affecting the respiratory or cardiovascular systems, as well as neurological disorders, can profoundly influence RR. The interpretation of RR must always be done in the context of the patient’s overall medical history and current clinical status.
- Medications: Certain medications, particularly sedatives, analgesics (like opioids), and neuromuscular blockers, can directly suppress respiratory drive, leading to slower and shallower breaths that may be harder to detect accurately.
Environmental and Situational Factors
Beyond the patient and the technology, external factors can also influence RR readings and their interpretation.
- Noise and Distractions: A noisy environment can interfere with acoustic monitoring and may also increase patient anxiety, leading to altered breathing patterns.
- Positioning of Monitoring Equipment: Incorrect placement of sensors or electrodes can lead to poor signal quality and inaccurate readings.
- Interactions with Other Monitoring Parameters: RR is often monitored alongside other vital signs like heart rate, blood pressure, and oxygen saturation. Changes in one parameter can influence another, and a holistic view is crucial for accurate interpretation. For example, a sudden drop in SpO2 might trigger an increase in RR as the body attempts to compensate.
The effective use of RR data from a hospital monitor hinges on a comprehensive understanding of these influencing factors. It requires not only an appreciation of the numbers displayed but also a critical assessment of how these numbers are generated and what they truly represent in the context of the individual patient.
Clinical Significance and Management Implications
The respiratory rate displayed on a hospital monitor is far more than just a number; it is a dynamic and invaluable piece of clinical information that directly informs diagnosis, guides treatment decisions, and serves as a critical indicator of patient prognosis. Its clinical significance spans the entire spectrum of patient care, from routine monitoring in general wards to intensive surveillance in critical care units.
Early Detection of Deterioration
One of the most profound implications of RR monitoring is its role in the early detection of patient deterioration. Changes in RR, particularly subtle increases or decreases that precede more obvious signs of distress, can serve as an early warning system. For instance, a gradual increase in RR in a post-operative patient might indicate developing hypoxia, pain, or the onset of an infection, allowing for timely intervention before a crisis ensues. Similarly, a slow and shallow breathing pattern in a patient receiving sedatives could signal impending respiratory depression. This proactive approach enabled by continuous RR monitoring is fundamental to preventing adverse events and improving patient safety.
Guiding Treatment Strategies
The RR value significantly influences treatment strategies across various medical disciplines. In the context of respiratory illnesses like asthma exacerbations or COPD flares, RR is a key parameter for assessing the severity of bronchoconstriction and the effectiveness of bronchodilator therapy. An improving RR in response to treatment suggests that the intervention is working. Conversely, a persistent or worsening RR may necessitate escalation of therapy, such as the addition of steroids or the need for mechanical ventilation.
In critical care settings, RR is a central component of managing patients on ventilators. The ventilator’s settings are adjusted based on the patient’s spontaneous respiratory efforts, gas exchange parameters, and overall clinical status, with RR being a primary target. For patients not on mechanical ventilation, a dangerously high or low RR can be an indication for non-invasive ventilation (NIV) or the urgent need for intubation and mechanical support.
Prognostic Value and Risk Stratification
The respiratory rate also holds significant prognostic value. Studies have consistently shown that an elevated RR is an independent predictor of adverse outcomes, including increased morbidity and mortality, across a wide range of patient populations. In patients presenting to the emergency department with conditions like sepsis or pneumonia, a high RR is associated with a greater risk of requiring intensive care, developing organ dysfunction, and experiencing mortality. This makes RR a crucial element in risk stratification tools used to prioritize care and allocate resources.
Impact on Other Vital Signs and Systemic Function
It is essential to recognize that RR does not operate in isolation. It is intimately linked with other vital signs and systemic functions. For example, an increased RR often accompanies an elevated heart rate (tachycardia) as the body attempts to compensate for reduced oxygen delivery or increased metabolic demand. Conversely, profound respiratory depression can lead to bradycardia and a decrease in blood pressure. Understanding these interrelationships is vital for a comprehensive interpretation of the patient’s physiological status. Furthermore, inadequate ventilation (low RR) leads to CO2 retention (hypercapnia), which can affect the body’s acid-base balance and have widespread systemic effects.
In conclusion, the “RR” on a hospital monitor signifies respiratory rate, a vital sign that provides a critical window into the efficiency of a patient’s breathing and the overall health of their respiratory system. Its accurate monitoring and interpretation, coupled with an understanding of the physiological principles and influencing factors, are indispensable for effective clinical practice, enabling early intervention, guiding therapeutic decisions, and ultimately contributing to improved patient care and outcomes.