The insidious damage wrought by smoking is a stark reality, and nowhere is this more evident than within the delicate architecture of the lungs. While the visible effects of smoking on the body are often discussed, the internal transformation of lung tissue is a complex and devastating process. Understanding what smokers’ lungs look like provides a powerful, albeit grim, visual testament to the destructive nature of tobacco smoke. This exploration delves into the macroscopic and microscopic changes that occur, detailing the progression of disease and the visual indicators that reveal the toll smoking takes on these vital organs.
Macroscopic Changes: The Visible Scars of Smoking
When examining the lungs of a smoker, particularly post-mortem or through advanced imaging techniques, several macroscopic changes become apparent. These are the broad, observable alterations that signify significant damage and disease. The color, texture, and overall appearance of a smoker’s lungs diverge dramatically from those of a healthy individual, offering a visceral representation of years of exposure to harmful toxins.
The Discoloration and Pigmentation
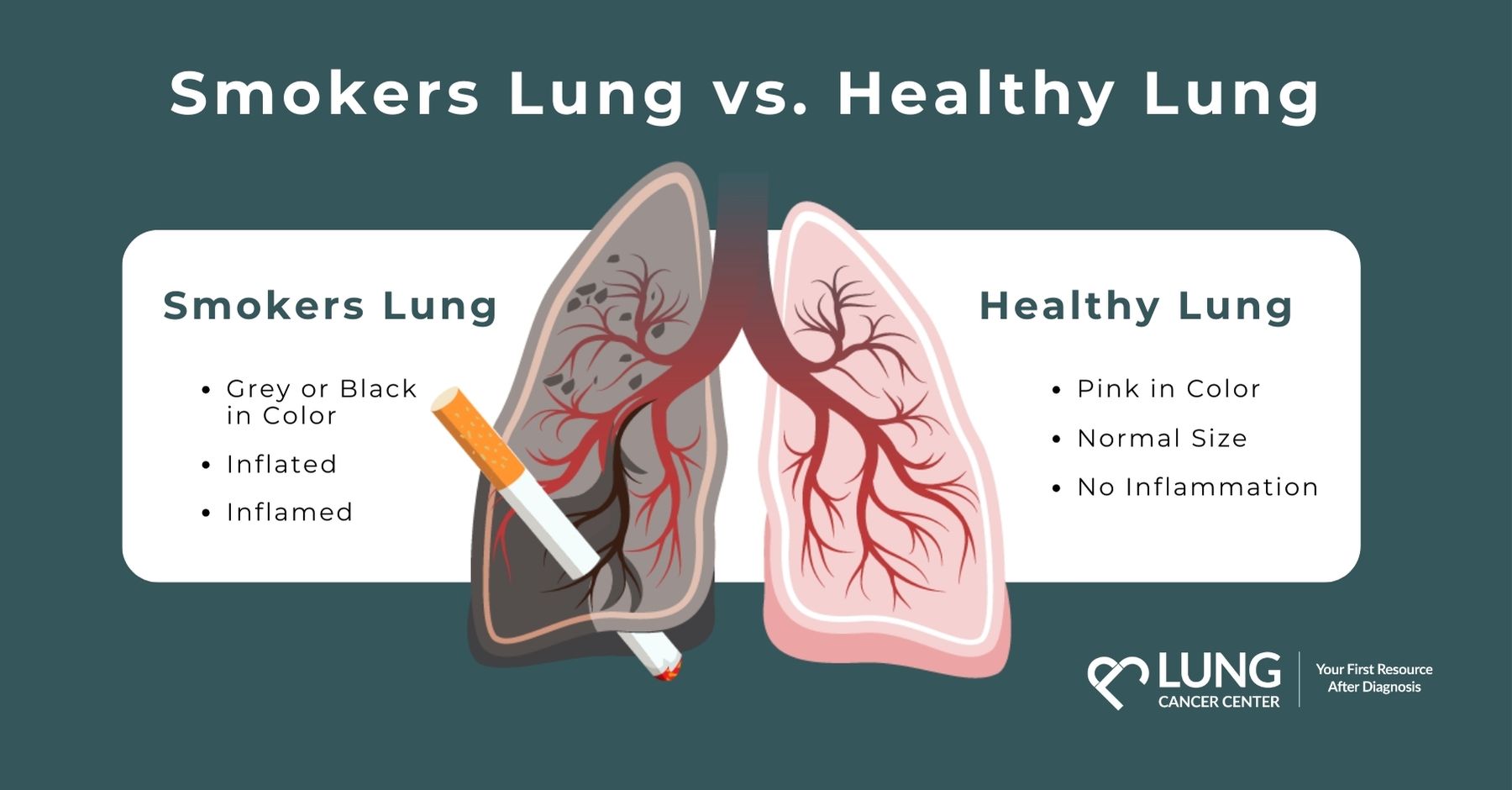
One of the most striking visual cues of a smoker’s lungs is their altered color. Healthy lung tissue is typically a pale pink, almost translucent color, allowing for efficient gas exchange. In contrast, the lungs of a long-term smoker are frequently stained with dark, tarry deposits. This blackish or brownish discoloration is a direct result of the tar and other particulate matter present in tobacco smoke accumulating within the lung airways and alveoli. This pigmentation isn’t just superficial; it permeates the lung tissue, indicating a deep-seated burden of inhaled carcinogens and irritants. The degree of discoloration often correlates with the duration and intensity of the smoking habit, serving as a grim historical record of exposure.
Architectural Distortion and Enlargement of Airspaces
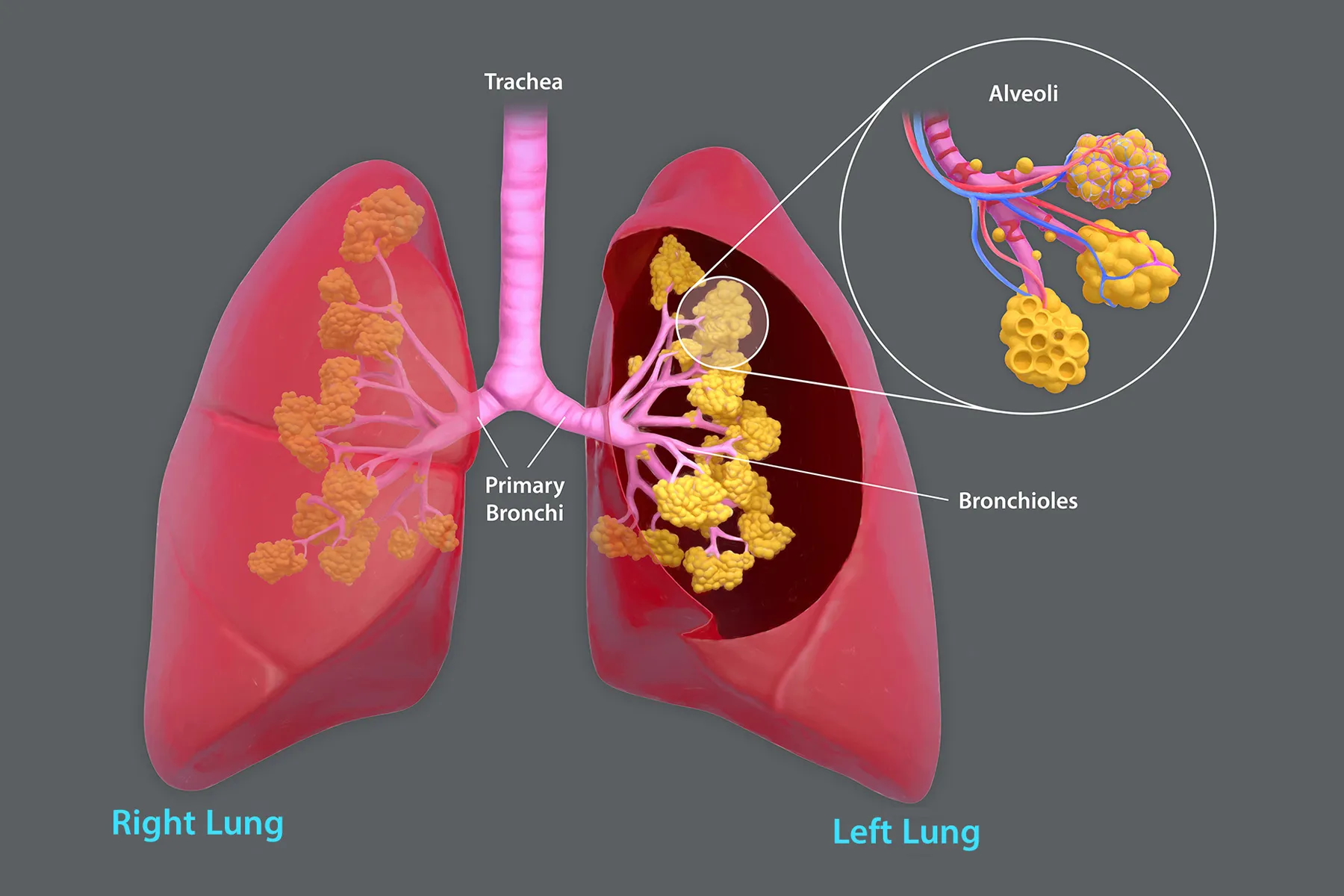
Beyond discoloration, the physical structure of the lungs undergoes significant distortion. Chronic inflammation and damage lead to the destruction of the delicate walls of the alveoli, the tiny air sacs responsible for oxygen and carbon dioxide exchange. This destruction results in the merging of multiple small air sacs into larger, irregular cavities. This process, known as emphysema, leads to a loss of lung elasticity and surface area for gas exchange.
Macroscopically, this manifests as a loss of the finely lobulated texture of healthy lung tissue. The lungs may appear enlarged and “floppy” due to the loss of their structural integrity. In severe cases, the lungs can become hyperinflated, as air becomes trapped within the damaged airspaces, making it difficult for the individual to exhale effectively. This architectural breakdown is a fundamental reason for the debilitating shortness of breath experienced by many smokers. Furthermore, the airways themselves, the bronchi and bronchioles, become thickened and inflamed due to chronic irritation. This can lead to a narrowed lumen, further impeding airflow and contributing to wheezing and coughing.
Presence of Tumors and Lesions
Perhaps the most feared macroscopic consequence of smoking is the development of lung cancer. While not all smokers develop cancer, the risk is dramatically elevated compared to non-smokers. Tumors in smokers’ lungs can vary significantly in size, shape, and location. They often appear as irregular masses, nodules, or infiltrates within the lung parenchyma. The presence of one or more tumors is a clear and devastating indicator of the carcinogenic effects of tobacco smoke.
Beyond overt tumors, smokers’ lungs may also exhibit other pathological lesions. These can include areas of fibrosis, where scar tissue replaces healthy lung tissue, further impairing function. Precancerous lesions, known as dysplasia or carcinoma in situ, may also be present, representing an intermediate stage in the development of invasive cancer. These microscopic changes, when accumulating over time, contribute to the macroscopic abnormalities observed.
Microscopic Changes: The Cellular Battleground
While the macroscopic view reveals the gross damage, a microscopic examination of smokers’ lung tissue unveils the intricate cellular battle that takes place with every inhaled puff of smoke. This cellular level reveals the ongoing inflammatory processes, the breakdown of tissue, and the initial stages of cellular transformation that can lead to disease.
Inflammation and Cellular Infiltration
The constant bombardment of irritants and toxins from cigarette smoke triggers a robust inflammatory response within the lungs. Under the microscope, this is evident by the increased presence of inflammatory cells, such as neutrophils, macrophages, and lymphocytes, infiltrating the lung tissue. These cells are part of the body’s defense mechanism, attempting to clear foreign particles and repair damaged cells. However, in the context of chronic smoking, this inflammatory response becomes persistent and dysregulated, leading to ongoing tissue damage rather than effective resolution.
The lining of the airways, the bronchial epithelium, undergoes significant changes. The normal ciliated cells, responsible for sweeping mucus and debris out of the lungs, are often damaged or replaced by goblet cells, which produce more mucus. This leads to an overproduction of mucus and a reduced ability to clear it, contributing to the characteristic smoker’s cough and an increased susceptibility to infections. The underlying connective tissue also shows signs of inflammation and edema.
Alveolar Destruction and Macrophage Activity
At the microscopic level, the destruction of alveolar walls is a hallmark of emphysema. The septa, the thin walls that divide the alveoli, begin to break down. This is partly driven by the release of enzymes by inflammatory cells, particularly macrophages, which are activated by the inhaled toxins. These macrophages engulf tar particles and cellular debris, but in doing so, they also release proteases that can degrade the elastic fibers and collagen that provide structural support to the alveolar walls.
The alveoli, which are normally small and numerous, coalesce into larger airspaces. This significantly reduces the total surface area available for gas exchange, meaning less oxygen can enter the bloodstream and less carbon dioxide can be removed. The capillaries that surround the alveoli also become damaged, further compromising the efficiency of oxygen transfer.
Cellular Atypia and Carcinogenesis
Perhaps the most alarming microscopic finding in the lungs of smokers is the presence of cellular atypia and the early stages of carcinogenesis. Tobacco smoke contains a cocktail of over 7,000 chemicals, of which at least 70 are known carcinogens. These carcinogens interact with the DNA of lung cells, causing mutations.
Under the microscope, these mutations can lead to cellular atypia, where cells exhibit abnormal size, shape, and nuclear characteristics. This can range from mild dysplasia to severe dysplasia, which is considered a precancerous condition. If these mutations accumulate and the cells evade the body’s natural repair mechanisms and immune surveillance, they can progress to invasive carcinoma, where the abnormal cells grow uncontrollably and invade surrounding tissues. The identification of these microscopic changes is crucial for early detection and intervention, although the prognosis for advanced lung cancer remains challenging.
Progression of Damage: A Timeline of Destruction
The changes observed in a smoker’s lungs are not instantaneous; they represent a cumulative process of damage that unfolds over years of exposure. The progression from initial exposure to severe lung disease is a grim timeline that underscores the importance of quitting smoking at any stage.
Early Stages: Irritation and Inflammation
In the initial years of smoking, the macroscopic changes may be minimal. However, at the microscopic level, the lungs are already under assault. The bronchial epithelium is irritated, leading to increased mucus production and inflammation. Cilia function may begin to be impaired. Smokers often experience a persistent cough, known as “smoker’s cough,” as their lungs attempt to clear the accumulating irritants. This early inflammation, while not immediately life-threatening, sets the stage for more significant damage to occur.
Mid-Stages: Chronic Bronchitis and Early Emphysema
As smoking continues, the inflammatory response becomes chronic. This leads to chronic bronchitis, characterized by persistent cough and mucus production for at least three months of the year for two consecutive years. Microscopically, the airways become thickened, and the goblet cells proliferate. The initial stages of alveolar wall destruction may also begin to be visible microscopically, with some loss of elasticity and early emphysematous changes. Lung function tests may start to show a decline, although the individual might not yet experience significant shortness of breath.
Advanced Stages: COPD and Lung Cancer
In the advanced stages of smoking, the damage becomes profound and often irreversible. Chronic Obstructive Pulmonary Disease (COPD), a broad term encompassing chronic bronchitis and emphysema, severely impairs lung function. Macroscopically, the lungs show significant architectural distortion, extensive discoloration, and enlarged airspaces. Microscopically, there is widespread alveolar destruction, significant inflammation, and cellular changes that can lead to the development of lung cancer. Shortness of breath becomes severe, limiting daily activities. The risk of developing lung cancer becomes exceedingly high, with the presence of tumors being a grim reality for many long-term smokers. The cumulative damage at this stage is extensive, making recovery of full lung function highly unlikely, even with cessation.
The Impact of Quitting: Reversing the Tide
While the damage inflicted by smoking can be severe and, in some cases, irreversible, quitting smoking at any point can initiate a process of healing and repair. The body’s capacity for regeneration, though limited in severely damaged lungs, can still lead to significant improvements in lung health.
Initial Improvements: Clearing Airways and Reduced Inflammation
Within days and weeks of quitting, the body begins to respond positively. The cilia in the airways start to regain their function, improving the ability to clear mucus and debris. The inflammatory markers within the lungs begin to decrease, leading to reduced swelling and irritation. The cough associated with smoking may initially worsen as the lungs actively clear accumulated mucus, but this is a sign of healing.

Long-Term Benefits: Reduced Risk and Improved Function
Over the long term, quitting smoking significantly reduces the risk of developing smoking-related diseases, including lung cancer, heart disease, and stroke. While the scarring from emphysema may not disappear, the progression of the disease slows down or stops. For individuals with chronic bronchitis, symptoms can improve, leading to a better quality of life. Lung function may stabilize or even show modest improvements, particularly in younger individuals who quit. The microscopic changes associated with precancerous lesions can also regress, lowering the risk of developing invasive cancer. The decision to quit smoking is a powerful intervention that can dramatically alter the trajectory of lung health and overall well-being.