Myocardial ischemia, a critical condition where the heart muscle receives insufficient oxygenated blood, is a primary concern in cardiology. The electrocardiogram (ECG) serves as a frontline diagnostic tool, offering a dynamic, real-time window into the heart’s electrical activity. Subtle yet significant alterations in the ECG waveform can herald the onset of ischemia, allowing for timely intervention and potentially mitigating severe damage. Understanding these specific changes is paramount for clinicians interpreting ECGs and for any professional involved in cardiac monitoring and assessment.
The Electrocardiogram as a Window to Ischemia
The ECG records the electrical impulses that cause the heart to contract. These impulses originate in the sinoatrial (SA) node and travel through the atria, atrioventricular (AV) node, bundle of His, bundle branches, and Purkinje fibers, culminating in ventricular depolarization and repolarization. Each of these electrical events corresponds to a specific waveform on the ECG: the P wave (atrial depolarization), the QRS complex (ventricular depolarization), and the T wave (ventricular repolarization).
Ischemia, by definition, disrupts the normal metabolic processes within the cardiac myocytes. This disruption affects the ionic gradients across the cell membranes, leading to altered electrical potentials and, consequently, changes in the ECG waveform. The severity and duration of ischemia, as well as the specific region of the myocardium affected, will dictate the pattern and magnitude of these ECG changes. While transient ischemia may result in reversible changes, prolonged or severe ischemia can lead to irreversible myocardial injury, or infarction.
The ECG is particularly sensitive to changes in repolarization, which is an energy-dependent process. During ischemia, ATP stores are depleted, impairing the function of ion pumps such as the Na+/K+-ATPase. This leads to intracellular accumulation of sodium and extracellular accumulation of potassium, altering the resting membrane potential and the action potential duration. These electrophysiological changes are then translated into visible alterations on the ECG.
The Importance of Baseline ECGs
Interpreting ECG changes in the context of ischemia is significantly enhanced by having access to a patient’s previous ECGs. A baseline ECG provides a reference point, allowing clinicians to distinguish between new, acute changes and pre-existing abnormalities. For instance, certain Q waves or T wave inversions might be chronic findings due to old infarcts, whereas new, dynamic changes are more indicative of current ischemic events. The absence of a baseline ECG necessitates a more cautious and comprehensive interpretation, relying heavily on the classic signs of acute ischemia.
Key ECG Manifestations of Ischemia
The ECG is a sensitive detector of myocardial ischemia, primarily reflecting changes in repolarization and, in more severe cases, depolarization. The hallmark changes are typically observed in the ST segment and the T wave.
ST-Segment Changes
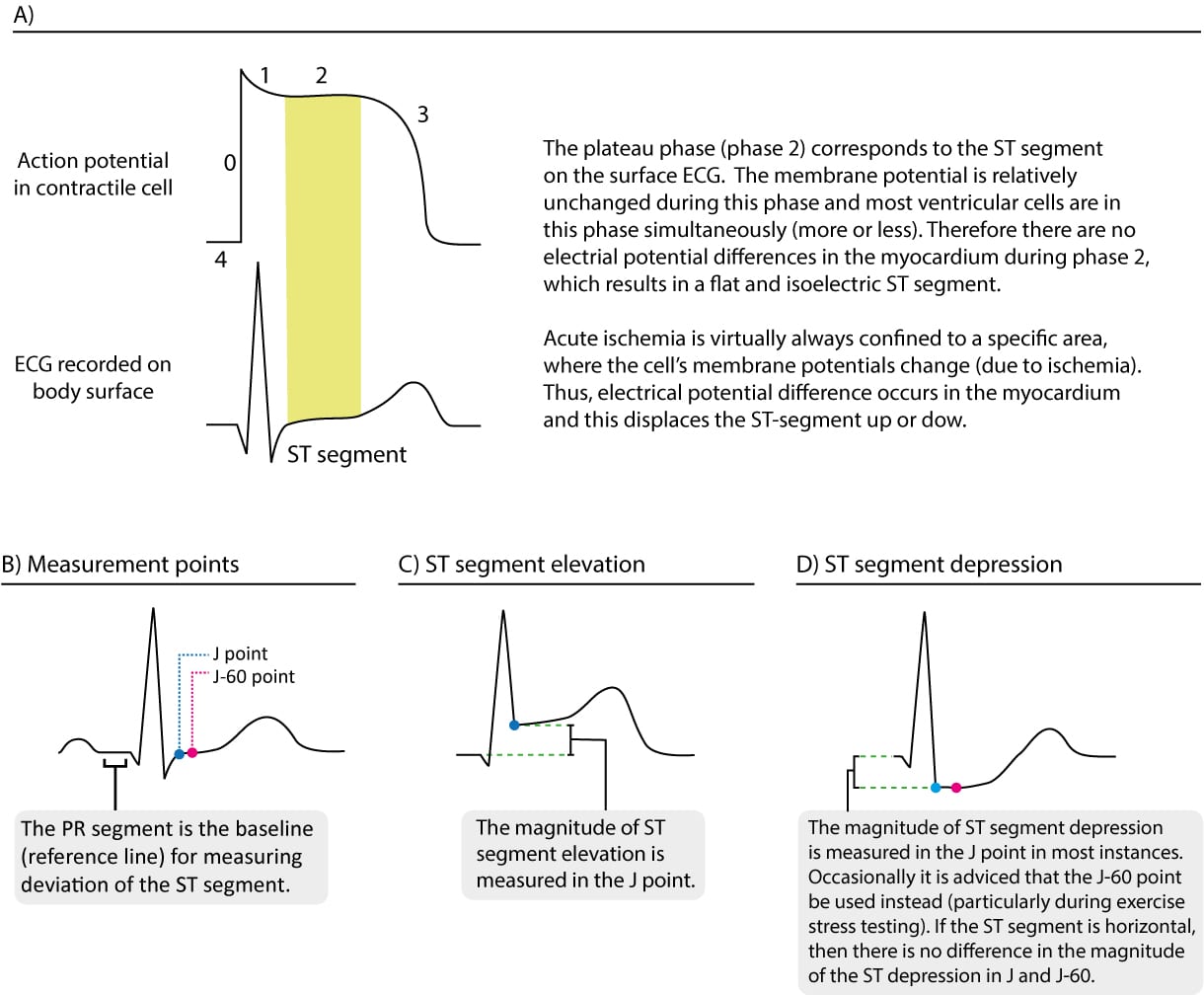
The ST segment represents the period between ventricular depolarization (QRS complex) and repolarization (T wave). It is normally isoelectric, meaning it lies on the baseline. Ischemia significantly impacts the ST segment, leading to deviations from this baseline.
ST-Segment Elevation
ST-segment elevation is a critical sign of acute myocardial injury, most commonly associated with transmural ischemia or infarction. In transmural ischemia, the entire thickness of the myocardial wall is affected, leading to a significant electrical potential difference across the ischemic zone.
- Morphology: The elevated ST segment typically appears convex (dome-shaped) and is often accompanied by reciprocal ST depression in leads that are electrically opposite to the ischemic area. The degree of elevation is a significant indicator; elevations of 1 mm (0.1 mV) or more in at least two contiguous leads are generally considered significant.
- Location: The leads showing ST elevation pinpoint the affected region of the myocardium. For example, ST elevation in leads II, III, and aVF suggests inferior wall ischemia, while elevation in V1-V4 points to anterior wall involvement. Anterolateral, posterior, and lateral wall ischemia also have characteristic patterns of ST elevation.
- Evolution: In the early stages of acute myocardial infarction (AMI), ST elevation is a prominent feature. As the infarction evolves, the ST segment may gradually return to baseline, followed by the development of Q waves and T wave inversions. Persistent ST elevation can sometimes indicate a non-Q wave myocardial infarction or a ventricular aneurysm.
ST-Segment Depression
ST-segment depression is a sensitive indicator of subendocardial ischemia, where the inner layers of the heart muscle are affected, but the full thickness is not compromised. This is often seen in unstable angina and non-ST-elevation myocardial infarction (NSTEMI).
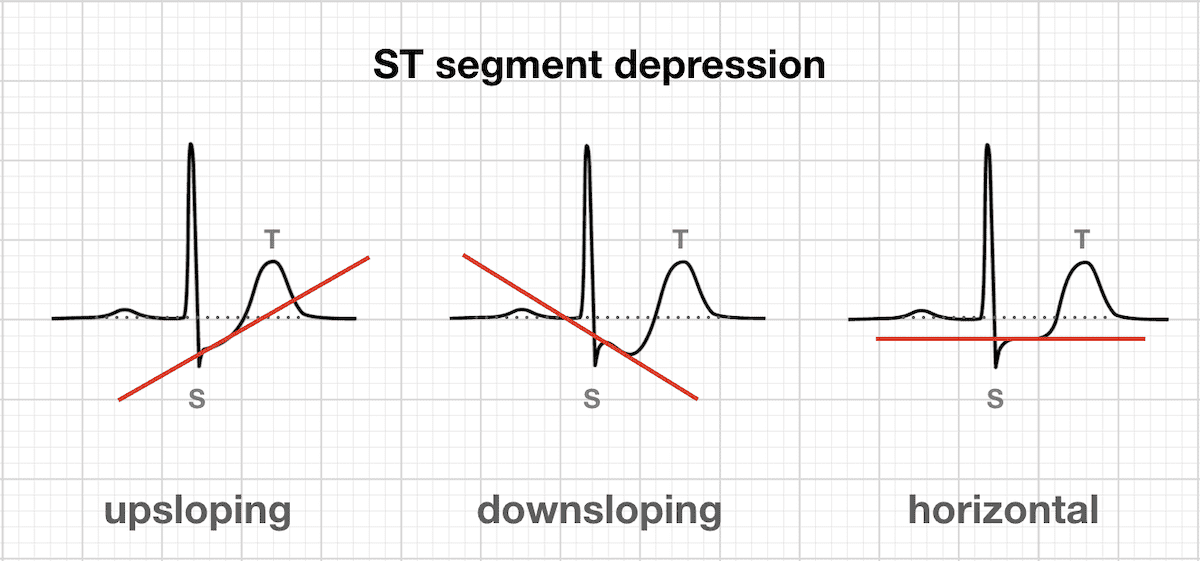
- Morphology: ST depression can be either horizontal, downsloping, or upsloping. Horizontal and downsloping ST depression are considered more significant and suggestive of ischemia than upsloping ST depression. A depression of 0.5 mm (0.05 mV) or more in at least two contiguous leads is generally considered significant.
- Reciprocal Changes: ST depression can also occur as a reciprocal change to ST elevation in leads opposite the area of infarction. However, in the context of ischemia without STEMI, ST depression itself is the primary ischemic manifestation.
- Differential Diagnosis: While ST depression can strongly suggest ischemia, it’s crucial to consider other causes, such as digoxin effect, left ventricular hypertrophy (LVH) with strain, or hypokalemia.
T-Wave Changes
The T wave represents ventricular repolarization. Ischemia profoundly affects this process, leading to characteristic T wave alterations.
T-Wave Inversion
T wave inversion is a common finding in myocardial ischemia. It can occur in both acute and chronic conditions.
- Subacute Ischemia/Angina: T wave inversion often appears after ST depression or in the absence of significant ST deviation, particularly in cases of unstable angina or NSTEMI. Initially, these T waves may be biphasic (partially positive, partially negative) before becoming completely inverted.
- Reciprocal Changes: Similar to ST depression, T wave inversion in certain leads can be a reciprocal change to ST elevation in contiguous leads.
- Symmetry: Ischemic T wave inversions are often deep and symmetrically inverted, contrasting with the typically asymmetrical T waves seen in other conditions.
- Resolution: In reversible ischemia, T wave inversion may resolve as blood flow is restored. However, persistent deep T wave inversions can be a sign of significant myocardial damage or a previous infarction.
Peaked T Waves (Hyperacute T Waves)
In the very early stages of acute transmural ischemia, before significant ST elevation occurs, T waves may become abnormally tall and peaked, often with a narrow base. These are known as hyperacute T waves.
- Significance: Their presence is a critical early warning sign of impending infarction. They indicate altered repolarization due to early ischemia.
- Evolution: Hyperacute T waves typically evolve into ST elevation over minutes to hours. Their recognition is crucial for initiating prompt reperfusion therapy.
- Differential Diagnosis: Peaked T waves can also be seen in hyperkalemia, but ischemic T waves often have a different morphology and occur in specific lead distributions.
Q Waves
Q waves represent the initial depolarization of the septum and are normally narrow and small. The development of significant Q waves (often defined as a Q wave width of >0.04 seconds or a depth of >25% of the R wave amplitude in a specific lead) is a hallmark of myocardial infarction, indicating irreversible myocardial necrosis.
- Pathological Q Waves: These indicate that a portion of the myocardium has died and is no longer electrically active. The electrical current then flows through the scar tissue, creating a negative deflection.
- Timing: Pathological Q waves usually develop several hours to days after the onset of infarction. Their presence signifies a completed infarct rather than acute, ongoing ischemia, although they can persist indefinitely.
- Absence in Ischemia: While Q waves are indicative of infarction, their absence does not rule out ischemia. Transient ischemic episodes typically do not cause the myocyte death required for Q wave formation.
Other ECG Clues Suggesting Ischemia
Beyond the primary changes in the ST segment and T wave, several other ECG findings can support the diagnosis of myocardial ischemia.
U Waves
U waves are small, positive deflections that sometimes follow the T wave. Their exact origin is debated, but they are thought to represent repolarization of the Purkinje fibers or papillary muscles.
- Prominent U Waves: Prominent U waves can be associated with hypokalemia, but they can also be observed in conditions of myocardial ischemia, particularly with certain drug effects like those of digoxin or in bradycardic rhythms where they become more visible.
- Ischemic Association: While not a primary sign of ischemia, their prominence in the context of other suggestive ECG findings or clinical symptoms can add weight to the suspicion of ischemia.
Arrhythmias
Ischemia disrupts the normal electrical conductivity and excitability of the heart, predisposing it to various arrhythmias.
- Ventricular Arrhythmias: Ischemia can trigger premature ventricular contractions (PVCs), ventricular tachycardia (VT), and ventricular fibrillation (VF), particularly in the context of transmural ischemia or infarction. These can be life-threatening.
- Atrial Arrhythmias: Atrial fibrillation (AF) and atrial flutter can also occur, especially with ischemia affecting the atria or as a consequence of reduced cardiac output and atrial stretch.
- Conduction Blocks: Ischemia can impair conduction through the AV node, leading to various degrees of heart block, from first-degree AV block to complete heart block. This is especially common with inferior wall ischemia affecting the AV node.
- Sinus Bradycardia: Particularly with inferior wall ischemia, parasympathetic stimulation can lead to sinus bradycardia.
Changes in Heart Rate and Rhythm
While not direct indicators of myocardial cell injury, alterations in heart rate and rhythm can be associated with ischemic events.
- Tachycardia: The sympathetic nervous system often upregulates in response to cardiac stress, including ischemia, leading to sinus tachycardia.
- Bradycardia: As mentioned, inferolateral ischemia can sometimes lead to significant bradycardia due to increased vagal tone.
Conclusion
The ECG remains an indispensable tool in the diagnosis and management of myocardial ischemia. Recognizing the subtle yet critical changes in the ST segment, T wave, and the potential development of Q waves, along with associated arrhythmias, is fundamental for effective clinical practice. While ST-segment elevation remains the most definitive indicator of acute transmural injury, ST-segment depression and T wave abnormalities are crucial for identifying subendocardial ischemia and unstable angina. A thorough understanding of these ECG manifestations, coupled with careful clinical correlation and consideration of a patient’s baseline ECG, allows for prompt and accurate diagnosis, facilitating timely interventions to preserve myocardial function and improve patient outcomes. Continuous monitoring and serial ECGs are often essential, as ischemic changes can evolve rapidly.