Typhlitis, a critical medical condition, presents a significant challenge in healthcare, particularly within specialized fields that might interact with or be affected by its sequelae. While not directly a technological or drone-related topic, understanding typhlitis is crucial for professionals who might encounter patients with this condition or those involved in its management, especially in contexts where rapid diagnosis and transport are paramount. This article aims to demystify typhlitis, exploring its definition, causes, symptoms, diagnosis, and treatment, with a specific focus on its implications within the broader context of medical emergencies and patient care.
Understanding Typhlitis: Definition and Pathophysiology
Typhlitis, also known as neutropenic enterocolitis, is a severe inflammatory process of the intestine, primarily affecting the cecum, but it can extend to the colon and ileum. It is characterized by inflammation, edema, and hemorrhage of the bowel wall. The hallmark of typhlitis is its strong association with neutropenia, a condition where the number of neutrophils (a type of white blood cell crucial for fighting infection) is abnormally low. This deficiency significantly compromises the body’s ability to combat bacterial and fungal pathogens that normally reside in the gastrointestinal tract.

The exact pathophysiology of typhlitis is complex and not fully understood, but it is believed to involve a combination of factors:
The Role of Neutropenia
The most significant predisposing factor is neutropenia. Patients undergoing chemotherapy, bone marrow transplantation, or those with certain hematological malignancies are particularly at risk. The compromised immune system allows commensal bacteria, which are usually harmless, to proliferate and invade the weakened intestinal mucosa.
Mucosal Damage
Chemotherapy and radiation therapy, commonly used in cancer treatment, can directly damage the intestinal lining. This damage creates breaches in the mucosal barrier, making it easier for bacteria to penetrate the deeper layers of the intestinal wall.
Bacterial Translocation
Once the mucosal barrier is compromised and the immune system is weakened, bacteria can translocate from the gut lumen into the intestinal wall and even into the bloodstream, leading to sepsis. Common culprits include Gram-negative bacteria like Escherichia coli, Pseudomonas aeruginosa, and Klebsiella species, as well as Candida species.
Inflammatory Response
The body’s immune response to this bacterial invasion, even in the setting of neutropenia, can contribute to the inflammation, edema, and necrosis of the bowel wall. Cytokines and other inflammatory mediators play a role in the destructive process.
Ischemia
Edema and inflammation within the bowel wall can lead to compression of blood vessels, compromising blood flow to the affected segments. This can result in ischemic injury and necrosis, further exacerbating the damage.
Clinical Presentation: Recognizing the Symptoms
The clinical presentation of typhlitis can be insidious or rapid, and often mimics other gastrointestinal emergencies. Prompt recognition is vital for timely intervention. The classic triad of symptoms includes:
Gastrointestinal Manifestations
- Abdominal Pain: This is typically the most prominent symptom, often localized to the right lower quadrant or periumbilical area, corresponding to the cecum and ascending colon. The pain can be severe and constant.
- Diarrhea: While not always present, diarrhea can range from mild to severe and watery. It may contain blood or mucus.
- Nausea and Vomiting: These symptoms can occur due to bowel inflammation and obstruction.
- Abdominal Distension: Swelling of the abdomen can be a sign of ileus or fluid accumulation.
- Tenderness: Palpation of the abdomen, particularly the right lower quadrant, elicits significant tenderness. Rebound tenderness and guarding may indicate peritoneal involvement.
Systemic Signs of Illness
- Fever: Fever is a common sign of infection and inflammation. However, in severely neutropenic patients, a fever may be absent or low-grade, making diagnosis more challenging.
- Chills and Malaise: General feelings of unwellness, fatigue, and shaking chills can accompany the infection.
- Hypotension and Tachycardia: In severe cases, particularly with sepsis or significant fluid loss, patients may develop low blood pressure and a rapid heart rate.
- Electrolyte Imbalances: Diarrhea and fluid shifts can lead to electrolyte disturbances, such as hypokalemia and hyponatremia.
It is crucial to note that in immunocompromised individuals, the absence of certain typical signs of infection (like high fever or significant leukocytosis) does not rule out a serious condition like typhlitis. A high index of suspicion is paramount.
Diagnostic Approaches: Identifying Typhlitis
The diagnosis of typhlitis relies on a combination of clinical suspicion, laboratory findings, and imaging studies.
Laboratory Investigations
- Complete Blood Count (CBC): This is essential to identify neutropenia. A neutrophil count below 1.5 x 10^9/L is generally considered neutropenia, with lower counts posing a higher risk. A low platelet count (thrombocytopenia) may also be present.
- Electrolytes and Renal Function Tests: To assess for dehydration and electrolyte imbalances.
- Liver Function Tests: May be abnormal in cases of severe sepsis or disseminated infection.
- Blood Cultures: To identify the causative organism(s) if sepsis is suspected.
- Stool Studies: While not always diagnostic, stool cultures can help identify infectious pathogens if diarrhea is present.
Imaging Modalities
Imaging plays a pivotal role in confirming the diagnosis and assessing the extent of bowel involvement.
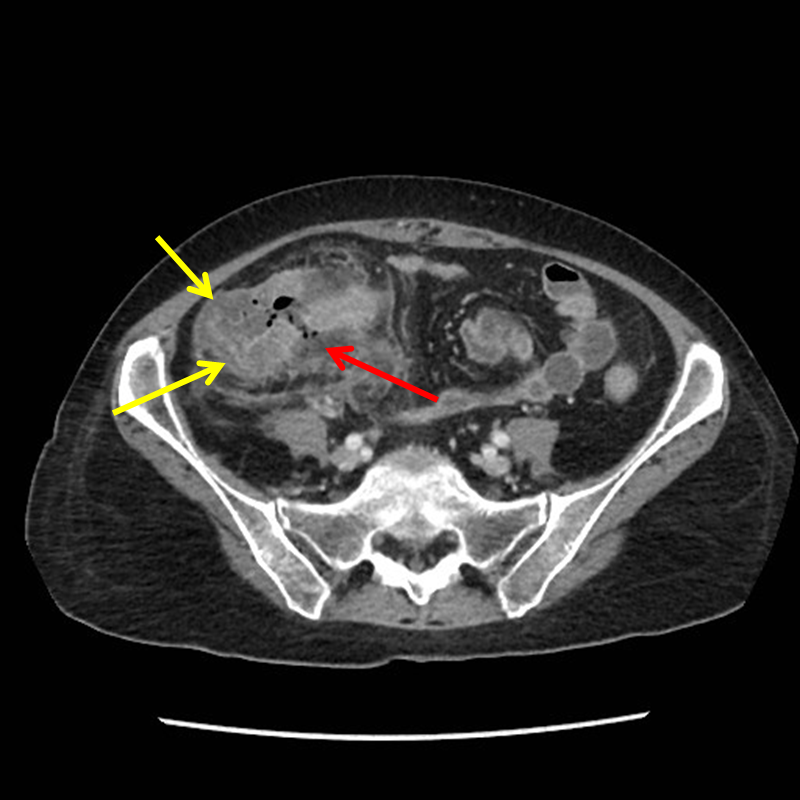
Computed Tomography (CT) Scan
- Gold Standard: CT scan of the abdomen and pelvis with intravenous and oral contrast is considered the imaging modality of choice for diagnosing typhlitis.
- Typical Findings: CT typically reveals thickening of the cecal and ascending colon walls, submucosal edema, and luminal narrowing. Extraluminal findings such as pericolic fat stranding, ascites, and even abscess formation or perforation can also be identified.
- Advantages: CT is highly sensitive and specific for typhlitis, can detect complications like perforation or abscess, and helps differentiate typhlitis from other conditions like appendicitis or diverticulitis.
Ultrasound
- Limited Role: Ultrasound can sometimes reveal bowel wall thickening and edema, but it is less sensitive and specific than CT, especially in obese patients or when there is significant bowel gas. It may be used as an initial assessment tool in some settings.
Plain Radiographs
- Limited Value: Plain abdominal X-rays are generally not helpful in diagnosing typhlitis but may show signs of bowel obstruction or ileus if present. They are primarily used to rule out free air if perforation is strongly suspected.
Management and Treatment Strategies
The management of typhlitis is largely supportive and aimed at stabilizing the patient, controlling infection, and allowing the bowel to heal.
Medical Management
- Bowel Rest: This is a cornerstone of treatment. Patients are kept nil per os (NPO) to prevent further irritation and damage to the inflamed bowel.
- Intravenous Fluid Resuscitation: Aggressive intravenous fluid administration is crucial to correct dehydration, electrolyte imbalances, and maintain hemodynamic stability.
- Parenteral Nutrition: If prolonged bowel rest is anticipated, parenteral nutrition (TPN) is initiated to provide essential nutrients and prevent malnutrition.
- Analgesia: Effective pain management is critical for patient comfort and to prevent physiological stress.
- Antiemetics: To control nausea and vomiting.
Antibiotic Therapy
- Broad-Spectrum Coverage: Empiric broad-spectrum antibiotic therapy is initiated promptly, targeting Gram-negative and anaerobic bacteria, as well as fungi. The choice of antibiotics will depend on local resistance patterns and the patient’s clinical status.
- De-escalation: Antibiotics are adjusted based on blood culture results and clinical response.
- Duration: The duration of antibiotic therapy is typically guided by the resolution of symptoms and improvement in neutropenia.
Role of Growth Factors
- Granulocyte Colony-Stimulating Factor (G-CSF): In patients with severe neutropenia, G-CSF may be administered to stimulate the bone marrow to produce more neutrophils, thereby improving the immune defense against infection.
Surgical Intervention
- Reserved for Complications: Surgery is generally reserved for cases where medical management fails or when complications arise, such as bowel perforation, abscess formation requiring drainage, or uncontrolled hemorrhage.
- Resection of Necrotic Bowel: If a segment of the bowel becomes necrotic and is deemed non-viable, surgical resection may be necessary. However, surgeons often attempt to avoid extensive bowel resection in neutropenic patients due to the high risks of complications and impaired healing.
Prognosis and Implications
The prognosis for typhlitis depends on several factors, including the severity of neutropenia, the extent of bowel involvement, the presence of complications, and the promptness of diagnosis and treatment. With aggressive supportive care and appropriate medical management, many patients can recover. However, typhlitis can be a life-threatening condition, with significant morbidity and mortality if not managed effectively.
Recurrence and Prevention
- Risk of Recurrence: Patients who have experienced typhlitis may be at risk of recurrence, particularly if they require further immunosuppressive therapy.
- Preventive Measures: Strategies to prevent typhlitis include meticulous bowel care, prophylactic antibiotics in certain high-risk populations, and prompt management of neutropenia.

Broader Medical Context
While typhlitis is a specific medical entity, understanding its characteristics is important for a range of healthcare professionals. For instance, in emergency medical services (EMS), the ability to recognize severe abdominal pain and systemic signs of illness in a patient who may be immunocompromised is critical. Rapid transport to a facility capable of advanced diagnostic imaging and critical care is paramount. Furthermore, in discussions around patient safety and quality improvement within hospitals, understanding conditions like typhlitis highlights the importance of interdisciplinary collaboration between oncology, hematology, surgery, and critical care teams. The complex management often requires a coordinated approach, where even seemingly unrelated technological advancements, such as rapid diagnostic tools or advanced patient monitoring systems, can indirectly contribute to better outcomes by enabling quicker and more precise interventions.