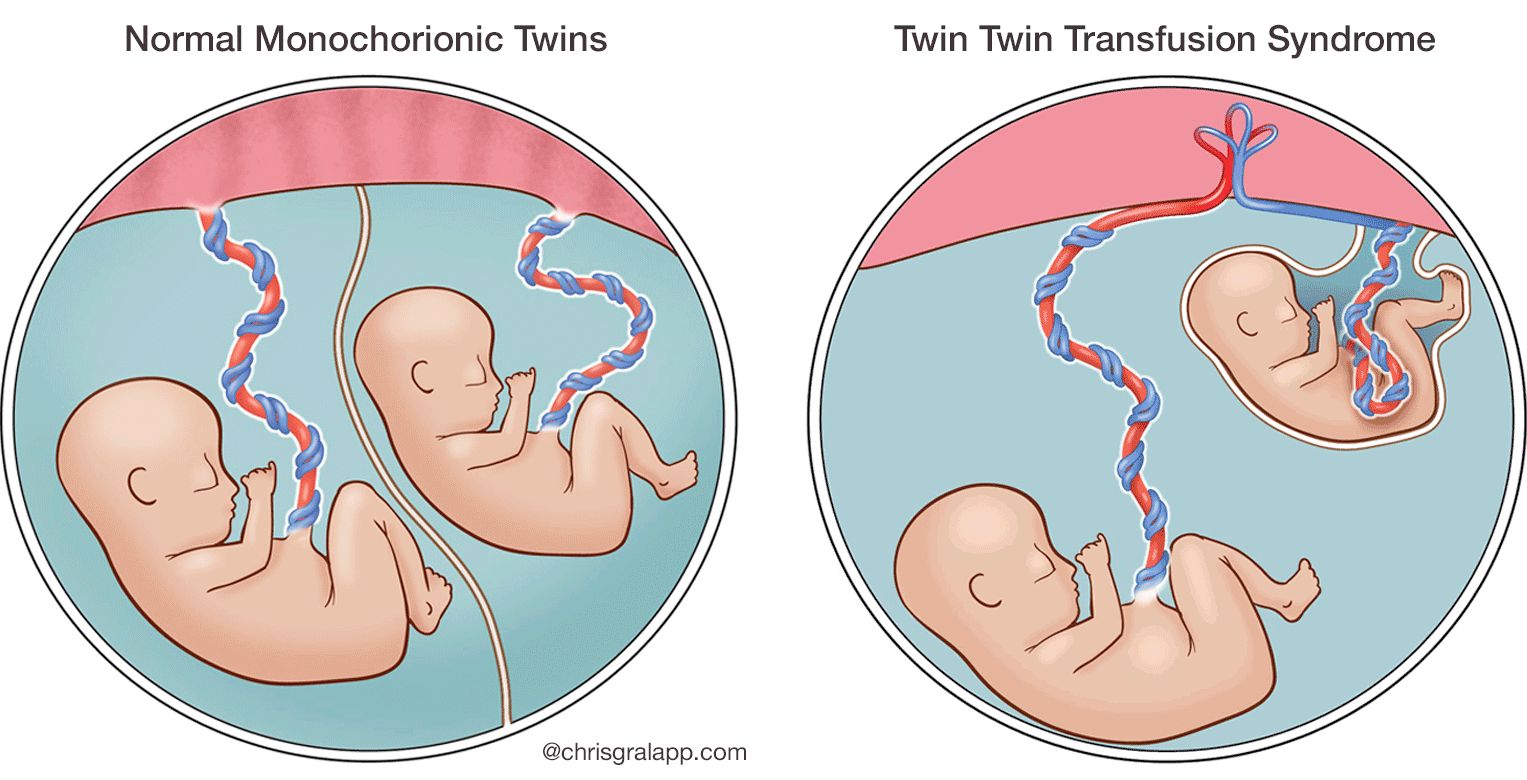
Twin to twin transfusion syndrome (TTTS) is a rare and serious complication that can occur in pregnancies with identical twins, also known as monochorionic twins. These twins share a placenta, which is a vital organ that provides them with oxygen and nutrients from the mother. In TTTS, an abnormal connection develops between the blood vessels of the placenta, leading to an unequal distribution of blood flow between the twins. One twin, known as the “donor,” sends too much blood to the other twin, while the other twin, known as the “recipient,” receives too much blood. This imbalance can have significant and potentially life-threatening consequences for both babies.
The exact cause of TTTS is not fully understood, but it is believed to be related to the way the placenta develops and the way the blood vessels connect. It typically occurs in the second trimester of pregnancy, when the twins’ circulatory systems are becoming more developed. The condition can progress rapidly, so early detection and intervention are crucial for improving outcomes.
The Delicate Balance of a Monochorionic Pregnancy
Monochorionic pregnancies, where identical twins share a single placenta, are inherently more complex than pregnancies involving fraternal twins or singletons. This shared placental unit, while providing a common source of sustenance, also creates the potential for a critical imbalance in blood flow. Understanding the intricacies of this shared environment is key to comprehending the development and impact of TTTS.
The Placenta: A Shared Lifeline
The placenta is a remarkable organ that facilitates the exchange of gases, nutrients, and waste products between the mother and her developing fetuses. In monochorionic pregnancies, this single placenta serves two developing babies. Ideally, the vascularization of the placenta is distributed equitably, ensuring that each twin receives adequate blood supply. However, in a subset of these pregnancies, the intricate network of blood vessels within the placenta can develop anomalous connections.
Vascular Connections: The Crucial Juncture
Within the shared placenta, there exist two main types of vascular connections: artery-to-vein (AV) and artery-to-artery (AA) anastomoses. Artery-to-artery connections are generally considered less problematic as they tend to equalize blood flow. Artery-to-vein anastomoses, however, are the primary culprits in the development of TTTS. In these connections, an artery from one twin directly connects to a vein of the other. This direct shunting of blood creates a unidirectional flow, bypassing the normal physiological regulation and leading to the unequal distribution of blood volume and pressure.
The Donor Twin: Giving Too Much
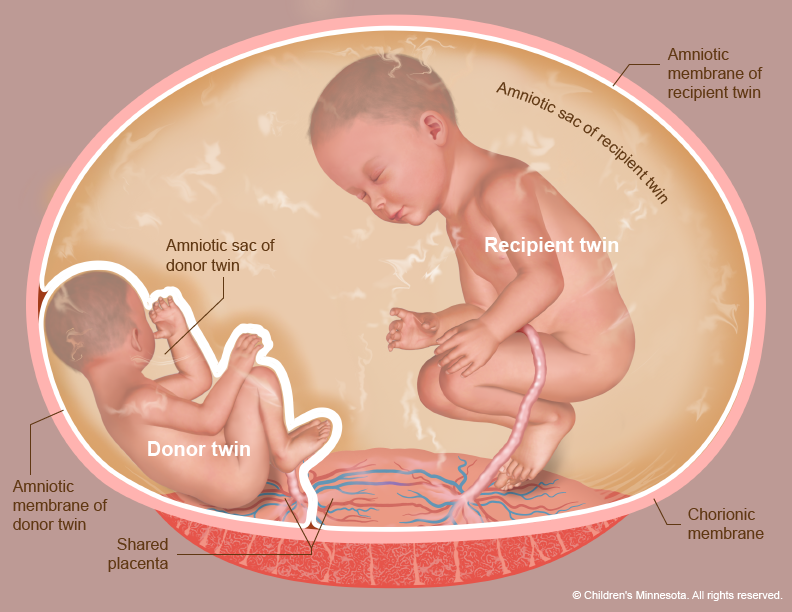
The twin that pumps blood into the shared placental circulation and loses an excessive amount to the recipient twin is known as the donor. This twin experiences a relative hypovolemia, meaning a decrease in blood volume. As a consequence, the donor twin’s kidneys produce less urine, leading to a reduced volume of amniotic fluid – the fluid that surrounds and protects the baby in the womb. This condition is termed oligohydramnios. The reduced amniotic fluid can impede lung development and restrict fetal movement, potentially leading to skeletal abnormalities.
The Recipient Twin: Receiving Too Much
Conversely, the recipient twin is the one that receives an excessive volume of blood from the donor twin via the placental vascular connections. This results in hypervolemia, an increased blood volume, and often leads to polycythemia, a condition where the blood has a higher concentration of red blood cells. The increased blood volume puts a strain on the recipient twin’s cardiovascular system, leading to a condition known as hydrops fetalis, characterized by significant fluid accumulation in various body tissues. The recipient twin’s kidneys also work overtime to excrete the excess fluid, leading to an overproduction of amniotic fluid, a condition called polyhydramnios. This excessive amniotic fluid can contribute to premature labor and other complications.
Recognizing the Signs and Symptoms of TTTS
The diagnosis of TTTS relies on a combination of clinical suspicion, ultrasound findings, and sometimes Doppler studies. Early recognition is paramount, as prompt intervention can significantly improve outcomes. While some cases are diagnosed during routine prenatal care, others may present with more overt symptoms.
Ultrasound: The Primary Diagnostic Tool
Ultrasound plays a pivotal role in the diagnosis and management of TTTS. During a routine obstetric ultrasound, particularly in monochorionic pregnancies, meticulous attention is paid to the placental anatomy and the growth and well-being of each twin. Key ultrasound findings indicative of TTTS include:
- Discrepancy in Amniotic Fluid Volume: The most common and consistent sign is the difference in amniotic fluid levels between the sacs of the twins. The donor twin will have significantly less amniotic fluid (oligohydramnios), while the recipient twin will have an excess (polyhydramnios). This is often quantified using the deepest vertical pocket (DVP) measurement.
- Fetal Growth Discordance: A significant difference in the estimated fetal weight between the twins, typically greater than 20%, can be a sign of TTTS. The donor twin may be smaller, while the recipient twin may be larger due to fluid overload.
- Bladder Visualization: In the donor twin, the bladder may be absent or significantly smaller, reflecting reduced urine production. The recipient twin’s bladder, on the other hand, will likely be distended.
- Doppler Velocimetry: Doppler ultrasound can assess blood flow within the umbilical arteries and veins, as well as in specific fetal vessels. Abnormal Doppler waveforms, such as reversed end-diastolic flow or absent end-diastolic flow in the umbilical artery of the donor twin, are concerning signs.
Clinical Manifestations in the Mother
While the primary impact of TTTS is on the fetuses, the mother can also experience symptoms. These are often related to the excessive amniotic fluid in the recipient twin’s sac, which can lead to:
- Rapid Increase in Fundal Height: The uterus grows at an accelerated rate due to the increased amniotic fluid, which can cause discomfort and pressure.
- Shortness of Breath: The enlarged uterus can press on the diaphragm, making breathing more difficult.
- Abdominal Pain or Tightness: This can be a symptom of uterine stretching and overdistension.
- Early Contractions or Braxton Hicks: The uterine distension can sometimes trigger premature contractions.
Stages and Management of Twin to Twin Transfusion Syndrome
The severity of TTTS is categorized into stages, which guide the treatment approach. The most widely used staging system is the Quintero staging system, which assesses several ultrasound parameters to determine the severity.
The Quintero Staging System
The Quintero staging system categorizes TTTS into five stages:
- Stage I: Oligohydramnios in the donor sac and polyhydramnios in the recipient sac, but all Doppler studies are normal, and the bladder is visible in the donor twin.
- Stage II: Absence or non-visualization of the donor twin’s bladder, despite oligohydramnios, and polyhydramnios in the recipient sac. Doppler studies may show abnormalities.
- Stage III: Abnormal Doppler flow studies in the umbilical arteries, veins, or ductus venosus of either twin. This indicates significant compromise of blood flow.
- Stage IV: Hydrops fetalis in one or both twins. This is a severe condition characterized by generalized edema (swelling) and fluid accumulation.
- Stage V: Fetal demise of one or both twins. This is the most tragic outcome.
Treatment Options: A Multi-faceted Approach
The management of TTTS is complex and depends on the stage of the syndrome, gestational age, and the overall condition of the fetuses and mother. The goal of treatment is to rebalance blood flow, improve fetal well-being, and prolong the pregnancy to allow for fetal maturation.
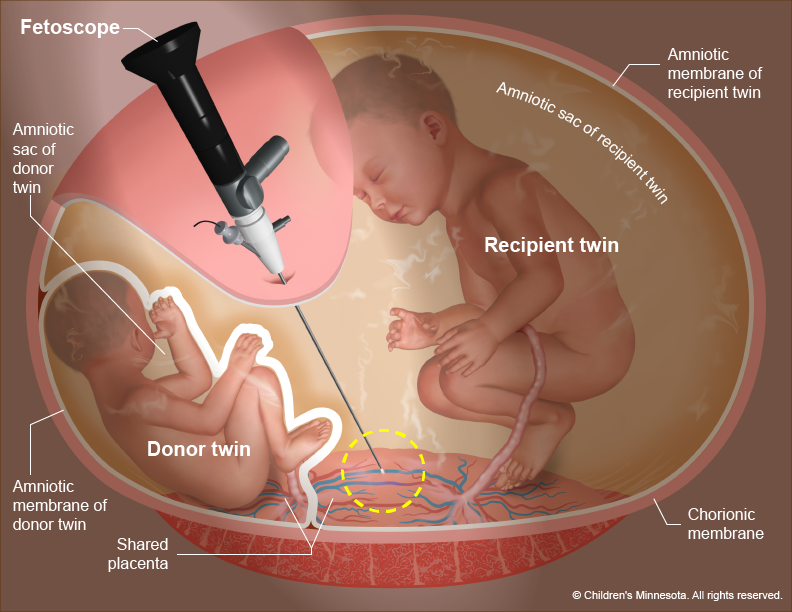
Laser Ablation of Placental Vessels
This is the most common and effective treatment for moderate to severe TTTS (Stages II-V). It is a minimally invasive surgical procedure performed under local anesthesia. A fetoscope (a small camera and laser fiber) is inserted through the mother’s abdomen and uterus into the amniotic sac. The surgeon carefully identifies and ablates (destroys) the abnormal vascular connections on the surface of the shared placenta, effectively blocking the unequal blood flow. This procedure aims to stop the transfusion and re-establish a more balanced circulation between the twins.
Amnioreduction
In cases of severe polyhydramnios in the recipient twin’s sac, a procedure called amnioreduction may be performed. This involves draining excess amniotic fluid from the recipient’s sac using a needle inserted through the mother’s abdomen. The aim is to reduce the pressure within the uterus and alleviate the risk of preterm labor and other complications associated with overdistension. Amnioreduction is often performed in conjunction with laser ablation or as a standalone treatment for less severe cases.
Selective Feticide
In very rare and severe cases, when one twin is severely compromised and poses a significant risk to the survival of the other twin, selective feticide may be considered. This involves terminating the pregnancy of the severely affected twin to improve the chances of survival for the other. This is an extremely difficult decision with profound emotional implications.
Serial Monitoring and Supportive Care
For mild cases of TTTS (Stage I) or when intervention is not immediately indicated, serial ultrasound monitoring is crucial. This involves frequent ultrasounds to assess fetal growth, amniotic fluid levels, and Doppler flow studies. Supportive care for the mother may include rest and close supervision for any signs of preterm labor.
Prognosis and Long-Term Outcomes
The prognosis for babies diagnosed with TTTS has significantly improved with advances in diagnostic techniques and treatment modalities. However, the outcomes can vary widely depending on the severity of the syndrome, the gestational age at diagnosis, the type of treatment received, and the presence of any co-existing complications.
Factors Influencing Prognosis
Several factors play a crucial role in determining the long-term outlook for infants affected by TTTS:
- Stage at Diagnosis: The earlier and more severe the stage of TTTS, the higher the risk of complications and poorer outcomes.
- Gestational Age at Intervention/Delivery: Pregnancies that can be continued to later gestational ages generally have better outcomes. Premature birth is a significant risk factor for many neonatal complications.
- Success of Treatment: The effectiveness of laser ablation or other interventions in rebalancing blood flow is a major determinant of survival and well-being.
- Development of Complications: The presence of hydrops fetalis, fetal anemia, or other severe complications during pregnancy can negatively impact outcomes.
- Neurological Development: While survival rates have improved, some infants who have experienced TTTS may be at an increased risk of long-term neurodevelopmental challenges, such as learning disabilities, motor deficits, or attention disorders. This is often related to the effects of anemia or the circulatory imbalances on brain development.
Potential Long-Term Challenges
While many survivors of TTTS thrive, some may face ongoing health issues. These can include:
- Cerebral Palsy: A group of disorders affecting movement, muscle tone, and posture, which can be related to brain injury during pregnancy or birth.
- Learning Disabilities and Developmental Delays: Some children may experience difficulties with cognitive functions, academic achievement, or developmental milestones.
- Vision and Hearing Impairments: These can occur due to the effects of anemia or other pregnancy-related complications.
- Cardiovascular Issues: In some cases, the recipient twin may have experienced significant strain on their cardiovascular system, potentially leading to long-term heart concerns.
- Growth and Behavioral Concerns: Some individuals may experience slower growth rates or behavioral challenges.
The Importance of Comprehensive Follow-Up
For families affected by TTTS, long-term follow-up care is essential. This typically involves regular pediatric check-ups, developmental assessments, and specialized evaluations as needed. Early identification and intervention for any developmental or health concerns can significantly improve a child’s quality of life and help them reach their full potential. The journey for families navigating TTTS is often challenging, but with continued advancements in medical care and dedicated support, the outlook for these precious twins is increasingly hopeful.