Thrombosis of the vein, a condition often misunderstood yet critically important in global health, represents a significant challenge in medical diagnostics and treatment. It involves the formation of a blood clot (thrombus) within a vein, obstructing normal blood flow and potentially leading to severe complications. Far from a rare occurrence, venous thrombosis affects millions worldwide annually, spanning a spectrum from uncomfortable swelling to life-threatening embolisms. Understanding this intricate physiological process, its causes, symptoms, and the innovative approaches to its management is paramount for both healthcare professionals and the general public. As technology and medical science continually advance, our ability to detect, prevent, and treat thrombosis becomes ever more sophisticated, embedding this medical challenge firmly within the domain of ongoing “Tech & Innovation” in healthcare.
This comprehensive overview aims to demystify venous thrombosis, delving into its fundamental nature, the factors that predispose individuals to it, the diverse ways it manifests, and the cutting-edge strategies employed to mitigate its impact. By shedding light on this crucial medical condition, we underscore the continuous need for research, technological integration, and informed public awareness to enhance patient outcomes and improve quality of life.
The Foundation of Venous Thrombosis: Understanding the Clot
At its core, thrombosis is a disruption of the body’s finely tuned hemostatic balance – the process that prevents excessive bleeding while ensuring blood remains fluid within vessels. When this balance tips, a clot forms where it shouldn’t, inside a vein. This seemingly simple event is a complex cascade of molecular and cellular interactions, influenced by a myriad of factors.
Virchow’s Triad: The Pillars of Clot Formation
For over a century and a half, Virchow’s Triad has served as the seminal framework for understanding the pathophysiology of thrombosis. Proposed by Rudolph Virchow in the mid-19th century, this triad identifies three primary factors contributing to thrombus formation:
- Endothelial Injury: The endothelium is the smooth inner lining of blood vessels. Damage to this lining, whether from trauma, surgery, inflammation, or certain medical conditions, exposes the underlying collagen and tissue factor, initiating the clotting cascade. This is akin to a road being damaged, making it uneven and prone to blockages.
- Stasis of Blood Flow: When blood flow slows down significantly, known as stasis, platelets and clotting factors accumulate, increasing their chances of interacting and forming a clot. This is particularly common in deep veins of the legs during prolonged immobility (e.g., long flights, bed rest, paralysis) or due to venous insufficiency. Imagine a river with slow-moving water; debris is more likely to settle and accumulate.
- Hypercoagulability: This refers to an increased propensity of the blood to clot, often due to an imbalance in clotting proteins or genetic predispositions. Conditions like inherited thrombophilias (e.g., Factor V Leiden mutation), cancer, pregnancy, hormone therapy, and certain autoimmune diseases can render the blood “stickier,” increasing the risk of thrombosis. This is like having too much cement mix in the water, making it prone to hardening.
Understanding these three pillars is crucial for assessing an individual’s risk and implementing effective preventive and therapeutic strategies. The interplay of these factors often dictates the severity and location of the thrombus.
Types of Venous Thrombosis
Venous thrombosis can occur in various parts of the body, with distinct implications for diagnosis and treatment:
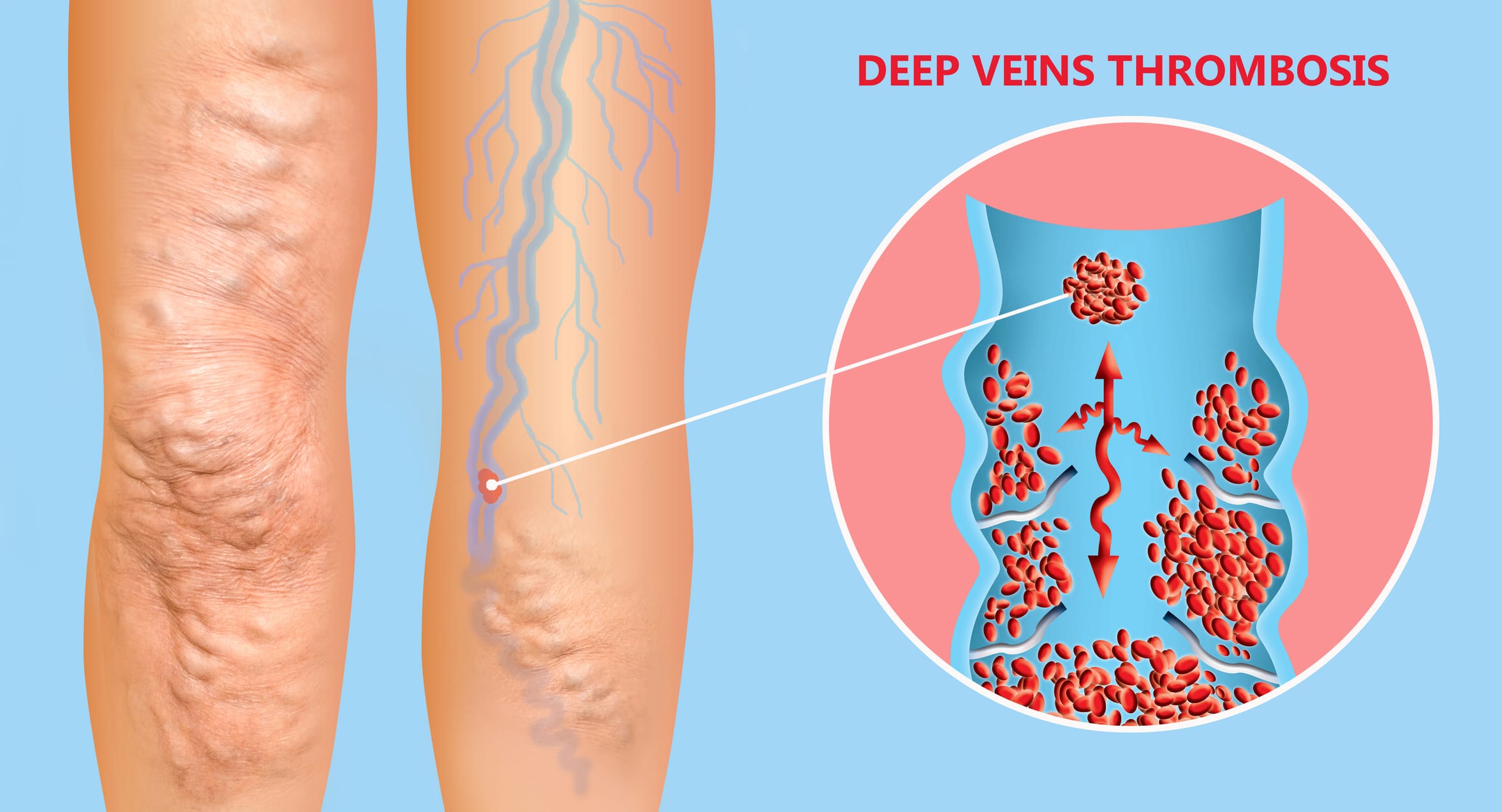
- Deep Vein Thrombosis (DVT): This is the most common and clinically significant form, typically affecting the deep veins of the legs (e.g., femoral, popliteal, iliac veins). DVT is dangerous not only because it obstructs blood flow but also because a piece of the clot can break off and travel to the lungs, causing a pulmonary embolism (PE).
- Superficial Vein Thrombosis (SVT): Also known as superficial thrombophlebitis, this involves clot formation in veins close to the skin’s surface. While generally less serious than DVT, SVT can be painful and, in some cases, may extend into the deep venous system or signal an underlying hypercoagulable state.
- Other Venous Thromboses: Clots can also form in other venous systems, such as cerebral venous sinus thrombosis (in the brain), portal vein thrombosis (in the liver), renal vein thrombosis (in the kidneys), or upper extremity DVT (in the arms, often associated with central venous catheters). Each location presents unique diagnostic and management challenges.
Recognizing the Signs: Symptoms and Diagnosis
Early recognition of venous thrombosis is critical for preventing complications and ensuring timely intervention. However, the symptoms can vary widely depending on the location and size of the clot, and in some cases, thrombosis can be entirely asymptomatic, making diagnosis particularly challenging.
Common Symptoms and Atypical Presentations
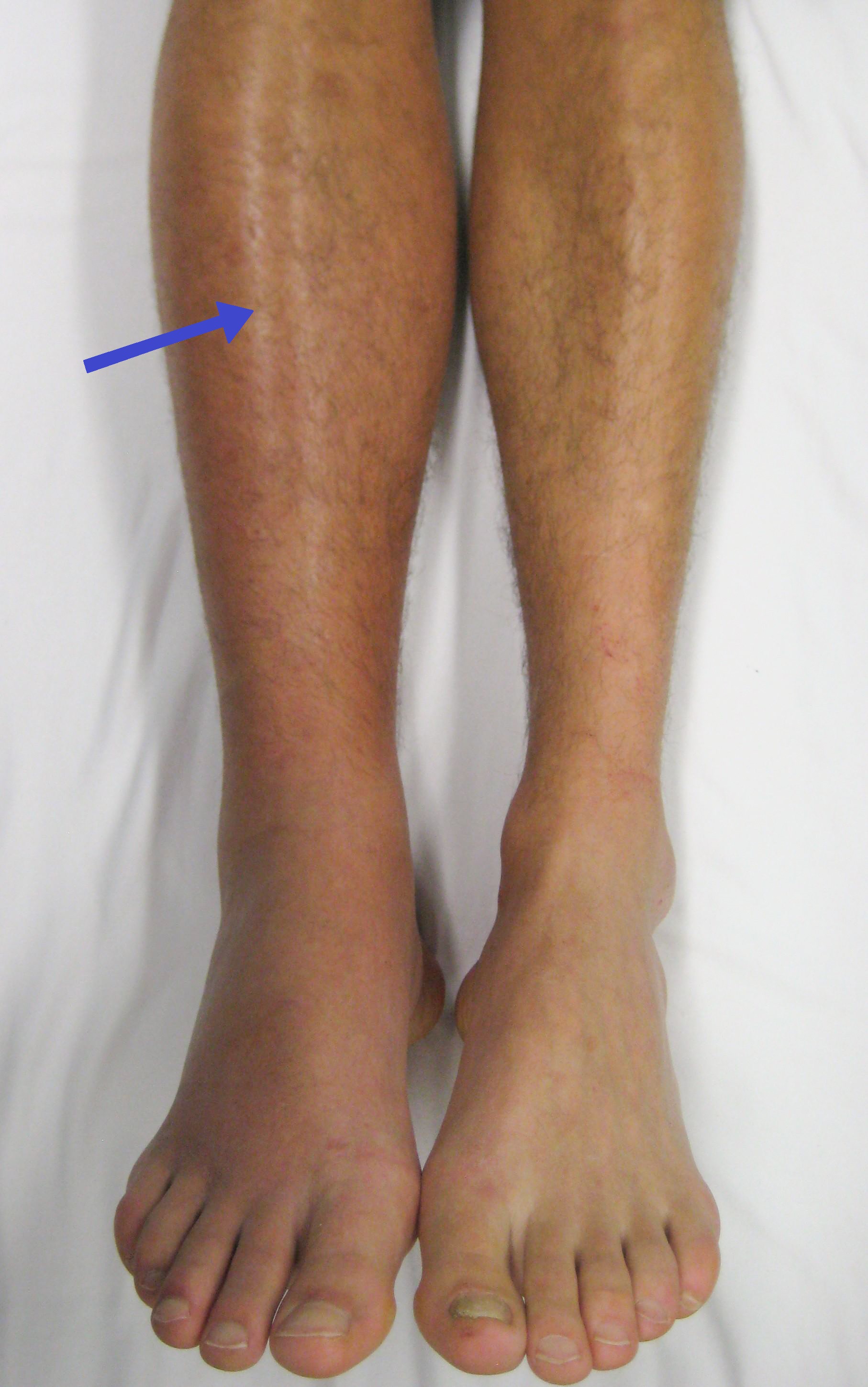
For DVT, the most common symptoms usually affect the limb where the clot is located, typically the leg:
- Swelling: Often localized to the affected limb, sometimes extending to the entire leg or arm.
- Pain or Tenderness: May feel like a cramp or soreness, often worsening with movement or standing.
- Warmth: The skin over the affected area may feel warmer than surrounding skin.
- Redness or Discoloration: The skin may appear reddish or bluish.
- Distended Superficial Veins: Veins near the surface may become more prominent due to increased pressure.
Superficial vein thrombosis often presents as a painful, red, hardened cord just under the skin. Cerebral venous sinus thrombosis can cause headaches, seizures, vision changes, or stroke-like symptoms. Pulmonary embolism, a complication of DVT, presents with sudden shortness of breath, chest pain, rapid heart rate, or coughing up blood, demanding immediate medical attention.
Diagnostic Technologies and Protocols
The diagnosis of venous thrombosis relies on a combination of clinical suspicion, risk assessment, and objective imaging techniques.
- Clinical Assessment and D-dimer Test: Initial assessment often involves evaluating risk factors and applying clinical prediction scores (e.g., Well’s score for DVT). A blood test measuring D-dimer, a degradation product of fibrin, can be very useful. A negative D-dimer generally rules out DVT in low-risk patients, but a positive result necessitates further imaging.
- Duplex Ultrasonography: This is the gold standard for diagnosing DVT and SVT. It uses sound waves to visualize blood flow within veins and detect clots. It is non-invasive, widely available, and highly accurate for clots in the proximal veins.
- CT Venography and MR Venography: For thrombosis in less accessible areas (e.g., pelvic veins, cerebral sinuses, portal vein) or when ultrasound is inconclusive, CT or MR venography can provide detailed images of the venous system and identify clots. These advanced imaging techniques are crucial for complex cases.
- Pulmonary Angiography (CTPA): If a pulmonary embolism is suspected, a CT pulmonary angiography (CTPA) is the primary diagnostic tool, visualizing the pulmonary arteries to detect clots.
The continuous refinement of these diagnostic technologies, coupled with the development of AI-driven predictive models for risk stratification, represents a significant area of innovation aimed at improving diagnostic accuracy and speed.
Managing the Condition: Treatment and Prevention Strategies
The management of venous thrombosis involves a multi-faceted approach aimed at preventing clot extension, reducing the risk of embolism, alleviating symptoms, and preventing recurrence. This includes both acute treatment and long-term preventive measures, often informed by personalized risk assessment and the latest pharmacological and interventional innovations.
Pharmacological Interventions: Anticoagulation
The cornerstone of thrombosis treatment is anticoagulation, often referred to as “blood thinners.” These medications do not dissolve existing clots but prevent them from growing larger and inhibit the formation of new ones, allowing the body’s natural fibrinolytic system to gradually break down the existing thrombus.
- Heparins (Unfractionated and Low Molecular Weight): Often used initially, especially in acute DVT, administered intravenously or subcutaneously.
- Warfarin: An oral anticoagulant that has been a standard for long-term treatment, requiring regular monitoring of blood clotting levels (INR).
- Direct Oral Anticoagulants (DOACs): A newer class of drugs (e.g., rivaroxaban, apixaban, dabigatran, edoxaban) that are increasingly preferred due to their predictable effects, fewer drug interactions, and not requiring routine blood monitoring. These represent a major pharmaceutical innovation, simplifying treatment for many patients.
The choice of anticoagulant, dosage, and duration of therapy depend on the location and extent of the thrombus, underlying risk factors, and patient specific characteristics.
Non-Pharmacological and Interventional Treatments
In certain situations, additional treatments may be necessary:
- Compression Stockings: Graduated compression stockings can help reduce swelling and post-thrombotic syndrome (a long-term complication of DVT) by improving venous flow in the legs.
- Thrombolysis: For massive DVT or PE that severely compromises circulation, thrombolytic agents (“clot busters”) may be used to rapidly dissolve the clot. This can be systemic or catheter-directed, a minimally invasive interventional procedure.
- Vena Cava Filters: In patients who cannot take anticoagulants or whose DVT recurs despite adequate anticoagulation, an inferior vena cava (IVC) filter may be placed to trap clots before they reach the lungs. This is generally a last resort due to potential complications.
- Thrombectomy: Surgical or catheter-based removal of the clot, typically reserved for severe cases where other treatments are insufficient.
Prevention: A Proactive Approach
Preventing venous thrombosis is as crucial as treating it, especially in high-risk individuals. Preventive strategies include:
- Early Ambulation: Encouraging movement after surgery or during periods of immobility.
- Mechanical Prophylaxis: Using graduated compression stockings or intermittent pneumatic compression devices (IPCDs) for hospitalized patients at risk.
- Pharmacological Prophylaxis: Administering prophylactic doses of anticoagulants to high-risk patients (e.g., after major surgery, in certain cancer patients).
- Lifestyle Modifications: Maintaining a healthy weight, regular physical activity, avoiding prolonged sitting or standing, and staying hydrated.

The Future of Thrombosis Management: Driven by Tech & Innovation
The field of thrombosis management is continuously evolving, driven by relentless innovation in diagnostics, pharmacology, and interventional techniques. Future advancements are likely to include:
- AI-Powered Risk Prediction: Sophisticated algorithms analyzing vast datasets of patient information to predict individual thrombosis risk with greater accuracy.
- Novel Anticoagulants: Development of new drugs with improved safety profiles, fewer side effects, and tailored mechanisms of action.
- Advanced Imaging: Real-time, higher-resolution imaging techniques and integration with augmented reality for guiding interventional procedures.
- Personalized Medicine: Tailoring prevention and treatment strategies based on an individual’s genetic makeup and specific risk factors, moving beyond one-size-fits-all approaches.
- Remote Monitoring Technologies: Wearable devices and telemedicine platforms for monitoring patient adherence to therapy and detecting early signs of recurrence or complications.
Thrombosis of the vein remains a formidable medical challenge, but the synergy of scientific discovery and technological innovation is steadily transforming our capacity to combat it. From elucidating its molecular mechanisms to deploying smart diagnostic tools and personalized therapies, the journey to eradicate the threat of thrombosis is a testament to the ongoing advancements in medicine and healthcare technology, firmly rooting its ongoing evolution within the dynamic landscape of “Tech & Innovation.” Continued research, public education, and collaboration across disciplines will be vital in further reducing its burden on global health.