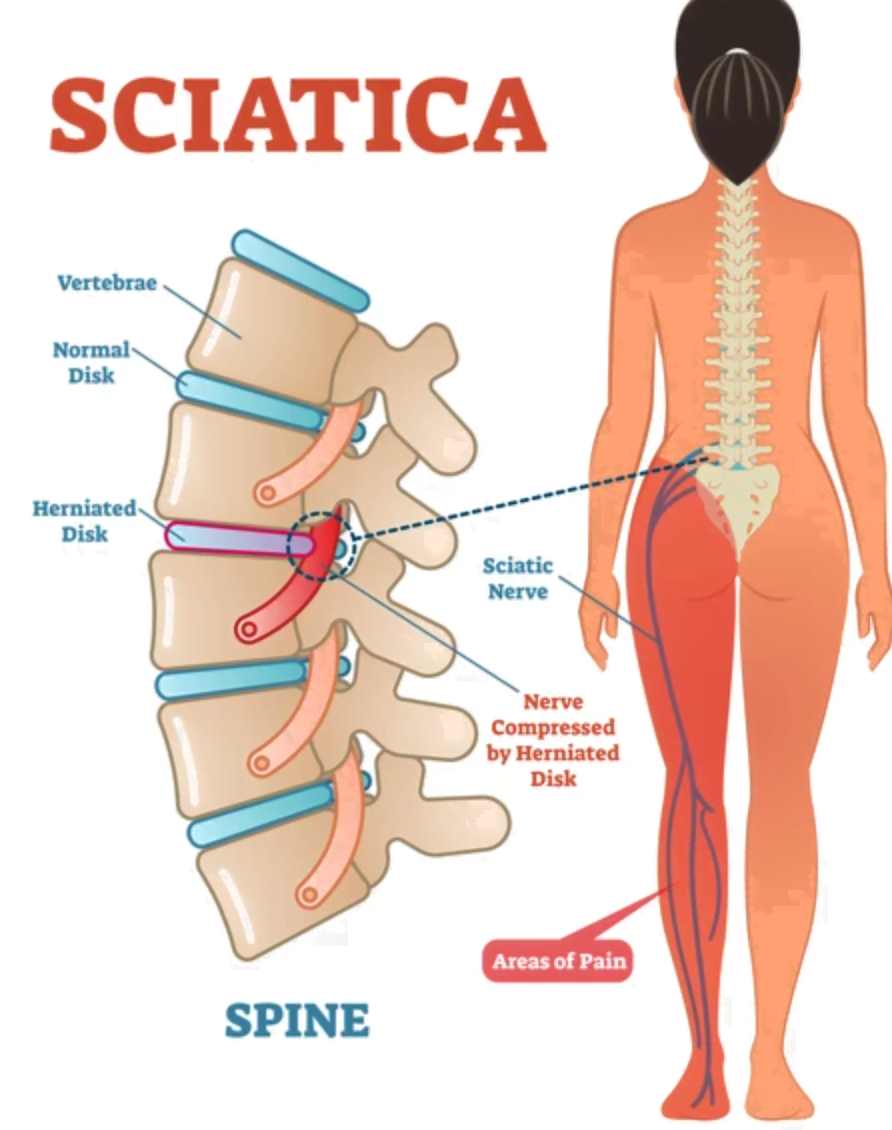
Sciatica, a term that evokes a visceral reaction of discomfort and pain, refers to a specific type of nerve irritation rather than a medical condition itself. It describes the pain that radiates along the path of the sciatic nerve, the longest and broadest nerve in the human body. This nerve originates in the lower back, passes through the buttocks, and then branches down each leg, extending all the way to the foot. When this nerve becomes compressed, inflamed, or irritated, it triggers a cascade of unpleasant sensations. Understanding the anatomy of the sciatic nerve, the common causes of its compression, and the diverse ways it can manifest is crucial for effective management and relief.
The Anatomy and Function of the Sciatic Nerve
The sciatic nerve is a marvel of biological engineering, serving as the primary conduit for signals between the brain and the muscles and skin of the legs and feet. Its intricate network of nerve fibers carries both motor commands and sensory information, enabling us to walk, run, feel the ground beneath our feet, and react to temperature and texture.
Origins and Pathways
The sciatic nerve is formed by a bundle of nerve roots emerging from the lumbar (lower back) and sacral (pelvic) regions of the spinal cord. Specifically, it’s comprised of contributions from the L4, L5, S1, S2, and S3 nerve roots. These roots converge to form two distinct trunks within the pelvis, which then merge to create the single, substantial sciatic nerve.
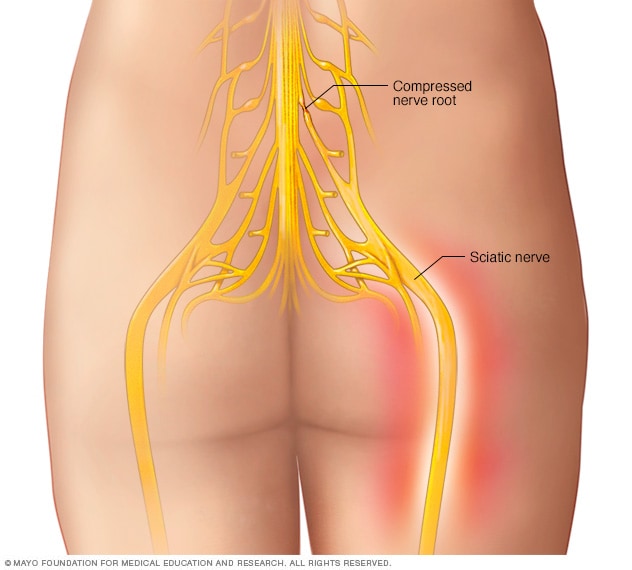
From its origin in the lower back, the nerve travels downwards through the buttock. It typically passes beneath or through the piriformis muscle, a small muscle located deep within the buttock. This anatomical relationship is significant, as the piriformis muscle can play a role in sciatica if it becomes tight or spasms. As the nerve continues its descent, it bifurcates (splits) in the popliteal fossa (the space behind the knee) into two main branches: the tibial nerve and the common fibular (peroneal) nerve. These branches further subdivide to innervate various muscles and sensory areas in the lower leg, ankle, and foot.
Motor and Sensory Functions
The sciatic nerve is responsible for a dual role:
- Motor Function: It controls the movement of numerous muscles in the posterior thigh, hamstring muscles (which help in bending the knee), and the muscles of the lower leg and foot. This allows for actions like extending the hip, flexing the knee, and pointing the toes downwards.
- Sensory Function: It transmits sensory information from the skin and deeper tissues of the posterior thigh, calf, ankle, and the sole of the foot back to the spinal cord and brain. This allows us to feel touch, pressure, temperature, and pain in these areas.
Any disruption to the integrity or function of this vital nerve can have profound consequences on mobility and sensation.
Common Causes of Sciatica
The “what is sciatica” question often leads to a deeper inquiry into its origins. Sciatica is a symptom, and its underlying cause is typically mechanical pressure or irritation on the sciatic nerve or its nerve roots. Identifying the root cause is paramount for effective treatment.
Lumbar Spine Issues
The most prevalent causes of sciatica stem from problems within the lumbar spine, where the nerve roots that form the sciatic nerve originate.
- Herniated or Bulging Disc: This is by far the most common culprit. The intervertebral discs, which act as cushions between the vertebrae, can degenerate over time or be injured. When the soft, gel-like center of a disc protrudes through its tougher outer layer (herniation) or bulges outwards, it can press directly onto an adjacent nerve root that contributes to the sciatic nerve. This compression leads to inflammation and pain radiating down the leg.
- Spinal Stenosis: This condition involves the narrowing of the spinal canal, the bony passage through which the spinal cord and nerve roots travel. This narrowing can be caused by age-related changes, such as bone spurs (osteophytes) or thickened ligaments. The reduced space can compress the nerve roots, mimicking the symptoms of sciatica.
- Spondylolisthesis: This occurs when one vertebra slips forward over the one below it. This slippage can put pressure on the exiting nerve roots, leading to sciatica.
- Degenerative Disc Disease: As discs age, they lose height and elasticity, becoming less effective at cushioning the vertebrae. This degeneration can lead to instability and sometimes nerve root compression.
Piriformis Syndrome
Beyond the spine, the piriformis muscle in the buttock can also be a source of sciatic pain.
- Piriformis Muscle Spasm or Tightness: The sciatic nerve typically passes close to or even through the piriformis muscle. If this muscle becomes inflamed, tight, or goes into spasm, it can compress the sciatic nerve, leading to pain that feels very similar to lumbar spine-related sciatica. This condition is known as piriformis syndrome. It can be aggravated by prolonged sitting, certain physical activities, or injuries.
Other Less Common Causes
While less frequent, other factors can contribute to sciatica.

- Tumors: In rare cases, tumors in the spine or pelvis can grow and press on the sciatic nerve or its roots.
- Trauma or Injury: Direct injury to the lower back, buttocks, or legs can damage the sciatic nerve or its surrounding structures, leading to pain.
- Infection: Though uncommon, infections in the spine or surrounding tissues can cause inflammation and nerve compression.
- Pregnancy: The weight of the growing uterus can put pressure on the sciatic nerve, and hormonal changes can lead to ligament laxity, contributing to nerve irritation.
Symptoms and Diagnosis of Sciatica
The experience of sciatica is often described as a distinct type of pain that sets it apart from general back discomfort. Its characteristic radiating pattern and accompanying sensory and motor disturbances are key diagnostic indicators.
The Nature of Sciatic Pain
The hallmark of sciatica is pain that originates in the lower back or buttock and travels down the back or side of the leg. The quality of the pain can vary widely among individuals.
- Radiating Pain: The pain typically follows the distribution of the sciatic nerve, though it might not always extend to the foot. It can be felt in the hip, thigh, calf, or foot.
- Intensity and Quality: Sciatic pain can range from a dull, persistent ache to a sharp, burning sensation or even excruciating electric-shock-like pain.
- Aggravating Factors: The pain is often worsened by actions that increase pressure on the sciatic nerve or its roots. This includes sitting for extended periods, bending forward, lifting heavy objects, coughing, or sneezing.
- Numbness and Tingling: Along with pain, individuals may experience a loss of sensation (numbness) or a prickling, pins-and-needles feeling (tingling) in the affected leg or foot. This is a sign of nerve dysfunction.
- Weakness: In more severe cases, compression of the sciatic nerve can lead to muscle weakness in the leg or foot. This might manifest as difficulty lifting the foot (foot drop), making it hard to walk normally.
Diagnostic Process
Diagnosing sciatica involves a comprehensive evaluation by a healthcare professional to pinpoint the underlying cause.
- Medical History and Physical Examination: The doctor will begin by asking detailed questions about the onset, nature, location, and aggravating factors of the pain. A physical examination will involve assessing posture, range of motion, muscle strength, reflexes, and sensation in the legs. Specific tests, such as the straight leg raise test (Lasègue’s test), can help reproduce the sciatic pain and indicate nerve root irritation.
- Imaging Studies: If the initial assessment suggests a significant underlying issue, imaging tests may be ordered.
- X-rays: These can help identify bony abnormalities such as spinal stenosis or spondylolisthesis, but they do not show soft tissues like discs or nerves.
- MRI (Magnetic Resonance Imaging): This is the gold standard for visualizing soft tissues and is highly effective in detecting herniated discs, spinal stenosis, and other structural problems that might be compressing the sciatic nerve.
- CT Scan (Computed Tomography): While not as detailed as MRI for soft tissues, a CT scan can provide excellent detail of bony structures and may be used if MRI is contraindicated or inconclusive.
- Electromyography (EMG) and Nerve Conduction Studies (NCS): These tests can help assess the health of the nerves and muscles and can help differentiate between nerve root compression and other causes of leg pain. They measure the electrical activity in muscles and the speed at which nerves conduct signals.
Management and Treatment of Sciatica
Once the cause of sciatica is identified, a tailored treatment plan can be implemented to alleviate pain, restore function, and prevent recurrence. The approach is often multi-faceted, combining conservative measures with more targeted interventions when necessary.
Conservative Treatments
The majority of sciatica cases resolve with conservative management over weeks to months.
- Rest and Activity Modification: While complete bed rest is generally not recommended, short periods of rest may be helpful during acute pain flares. However, it is crucial to return to gentle activity as soon as possible. Avoiding activities that exacerbate the pain, such as heavy lifting or prolonged sitting, is important.
- Pain Management:
- Over-the-Counter (OTC) Pain Relievers: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen can help reduce inflammation and pain. Acetaminophen may also be used for pain relief.
- Prescription Medications: In cases of severe pain, doctors may prescribe stronger pain relievers, muscle relaxants, or anti-inflammatory medications.
- Physical Therapy: This is a cornerstone of sciatica treatment. A physical therapist can design an individualized exercise program focusing on:
- Stretching: Exercises to lengthen tight muscles, particularly the hamstrings and piriformis.
- Strengthening: Exercises to build core strength (abdominal and back muscles) to better support the spine.
- Posture Education: Guidance on proper posture and body mechanics to reduce strain on the back.
- Manual Therapy: Techniques such as massage and joint mobilization may be used to relieve muscle tension and improve spinal mobility.
- Heat and Cold Therapy: Applying heat packs or cold compresses to the affected area can help reduce inflammation and muscle spasms.
Interventional Treatments
If conservative treatments fail to provide adequate relief, or if there are signs of severe nerve compression, interventional procedures may be considered.
- Epidural Steroid Injections: Corticosteroids can be injected into the epidural space around the spinal cord and nerve roots. This powerful anti-inflammatory medication can significantly reduce swelling and pain by decreasing inflammation around the irritated nerve.
- Nerve Blocks: Local anesthetic injections can be used to block pain signals from specific nerves.
Surgical Interventions
Surgery is typically reserved for cases of sciatica that are severe, persistent, or caused by conditions that cannot be effectively managed by conservative means, such as significant disc herniations causing progressive weakness or cauda equina syndrome (a rare but serious condition affecting the nerves at the end of the spinal cord).
- Laminectomy/Discectomy: This procedure involves removing a portion of the lamina (a part of the vertebra) and/or the herniated disc material that is compressing the nerve root.
- Spinal Fusion: In cases of severe instability, such as with spondylolisthesis, spinal fusion may be performed to stabilize the vertebrae.
Living with sciatica can be challenging, but understanding its causes, symptoms, and the range of treatment options available empowers individuals to take an active role in their recovery and regain a pain-free life. Consulting with a healthcare professional for an accurate diagnosis and personalized treatment plan is always the essential first step.