The acronym PGT, in the context of genetic testing, stands for Preimplantation Genetic Testing. This advanced reproductive technology plays a crucial role in modern fertility treatments, offering prospective parents a deeper understanding of the genetic health of their embryos before implantation. PGT is not a single test but rather a suite of techniques designed to screen embryos for specific genetic abnormalities, thereby increasing the chances of a successful pregnancy and reducing the risk of certain inherited conditions.
The advent of PGT has revolutionized the field of assisted reproductive technology (ART), moving beyond simply achieving pregnancy to optimizing the genetic quality of the resulting pregnancy. It is typically performed in conjunction with in vitro fertilization (IVF), where eggs are fertilized by sperm in a laboratory setting. Following fertilization and initial embryonic development, a few cells are carefully biopsied from the developing embryo for genetic analysis. This information then guides the selection of the healthiest embryo for transfer into the uterus.
The decision to undergo PGT is a significant one, often involving careful consideration of ethical, medical, and personal factors. It is a process that requires comprehensive counseling and a thorough understanding of its benefits, limitations, and potential risks. This article aims to demystify PGT testing, exploring its various forms, the indications for its use, the process involved, and its impact on family planning and reproductive health.
Understanding the Different Types of PGT
PGT is a broad term encompassing several distinct testing methodologies, each tailored to address different genetic concerns. The choice of which PGT method to utilize depends entirely on the specific genetic risk factors present in a prospective parent or couple. Understanding these distinctions is paramount to appreciating the full scope of what PGT can achieve.
Preimplantation Genetic Diagnosis (PGD)
Historically, PGD was the term used for testing embryos for specific single-gene disorders or chromosomal translocations. While the terminology has evolved, the core purpose of PGD remains the same: to identify embryos that carry a particular genetic mutation or structural chromosomal abnormality that could lead to a specific inherited disease. This is particularly relevant for couples where one or both partners are known carriers of a recessive genetic disorder (like cystic fibrosis or sickle cell anemia) or have a balanced translocation (where chromosomal material has been rearranged but no genetic material has been lost or gained, which can lead to unbalanced chromosomes in offspring).
- Single-Gene Disorder Testing: This application of PGD is crucial for families with a known history of specific inherited diseases caused by mutations in a single gene. Before undergoing PGT, a genetic probe is developed specifically for the gene in question. This probe is used to test the embryo’s DNA for the presence or absence of the mutation. If an embryo is found to carry the mutation, it can be excluded from transfer, preventing the transmission of the disease to the child.
- Chromosomal Translocation Testing: For individuals with balanced chromosomal translocations, the risk of producing embryos with unbalanced chromosomal arrangements is significantly elevated. These unbalanced embryos can lead to miscarriage, infertility, or a child with a genetic syndrome. PGD can identify which embryos have the correct number and arrangement of chromosomes, avoiding the transfer of chromosomally unbalanced embryos.
Preimplantation Genetic Screening (PGS)
PGS, now more commonly referred to as Preimplantation Genetic Testing for Aneuploidy (PGT-A), is a broader form of genetic testing. Its primary focus is to screen embryos for aneuploidy, which is an abnormal number of chromosomes. Most human cells have 46 chromosomes arranged in 23 pairs. Aneuploidy occurs when an embryo has an extra chromosome (e.g., Down syndrome, where there are three copies of chromosome 21) or is missing a chromosome.
- Aneuploidy Screening: PGT-A is particularly beneficial for certain patient populations and has become a standard part of many IVF cycles. It can help identify embryos that are chromosomally normal, which can have several implications. For older women undergoing IVF, the rate of aneuploidy increases significantly with age, making PGT-A a valuable tool for selecting viable embryos. It can also be beneficial for individuals with recurrent implantation failure or recurrent pregnancy loss, as aneuploid embryos are a common cause of these issues. By transferring chromosomally normal embryos, the chances of implantation and a successful live birth can be improved, while the risk of miscarriage may also be reduced.
Preimplantation Genetic Testing for Monogenic/Single Gene Defects (PGT-M)
This category specifically addresses testing for inherited disorders caused by mutations in a single gene. As mentioned under PGD, PGT-M is designed to identify embryos that are free of a specific known genetic mutation within a family. The process is highly personalized, requiring the development of a specific probe for the gene of concern. This is distinct from PGT-A, which looks at the overall number of chromosomes rather than specific gene mutations. PGT-M is a powerful tool for families who wish to avoid passing on a particular genetic condition to their offspring, offering a proactive approach to reproductive planning.
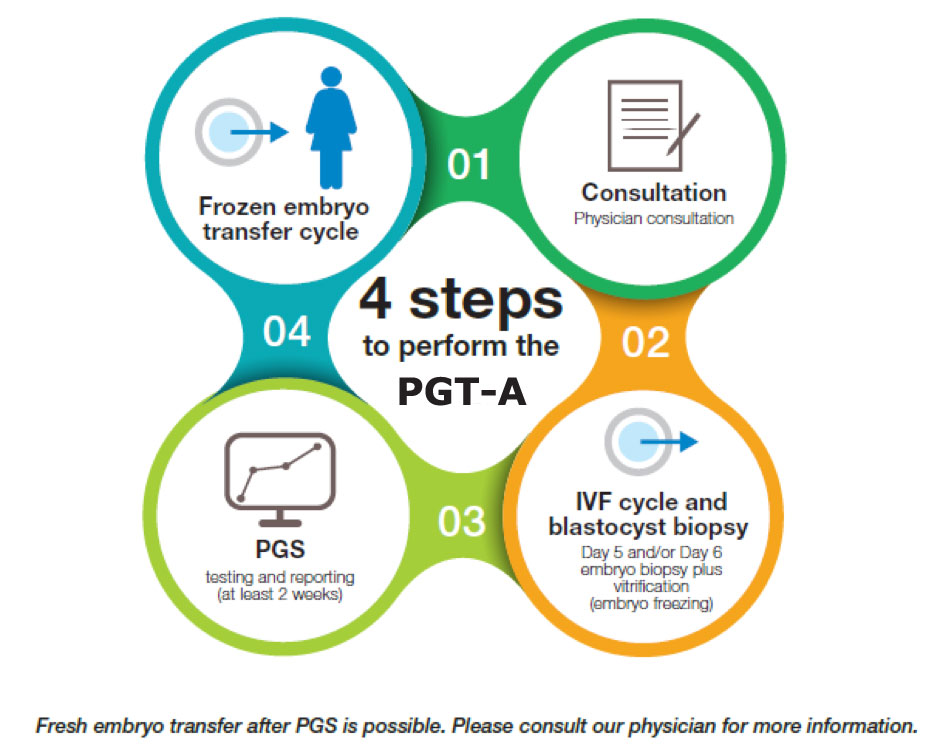
The PGT Process: From IVF to Embryo Selection
Undergoing PGT involves a series of interconnected steps, meticulously managed by a multidisciplinary team of fertility specialists, geneticists, and embryologists. The entire process is integrated within a standard IVF cycle, with the genetic testing being an additional layer of analysis performed on the developing embryos.
The IVF Cycle and Embryo Biopsy
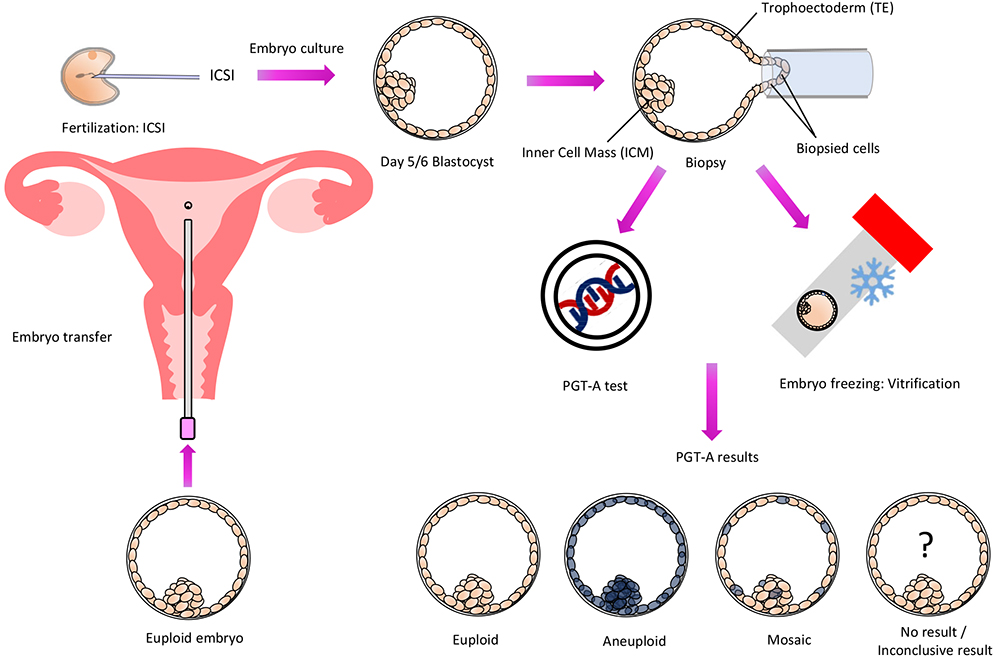
The journey begins with a standard IVF cycle. This involves ovarian stimulation to produce multiple eggs, egg retrieval, fertilization of the eggs with sperm in the laboratory, and the subsequent development of embryos. Once the embryos reach a specific developmental stage, typically the blastocyst stage (around day 5 or 6 after fertilization), a crucial step known as embryo biopsy is performed.
- Blastocyst Biopsy: At the blastocyst stage, the embryo has differentiated into two main cell types: the inner cell mass, which will develop into the fetus, and the trophectoderm, which will form the placenta. For PGT, a few cells are carefully removed from the trophectoderm. This is a highly skilled procedure performed by experienced embryologists under a microscope. The biopsy is designed to be minimally invasive, removing cells that are destined to become placental tissue, thereby minimizing any potential harm to the developing fetus. The biopsied cells are then sent to a specialized genetic laboratory for analysis.
Genetic Analysis and Reporting
The laboratory analysis of the biopsied cells is a complex process that varies depending on the type of PGT being performed. Advanced molecular techniques are employed to extract and analyze the DNA from the sampled cells.
- PGT-A Analysis: For PGT-A, techniques like Next-Generation Sequencing (NGS) or Chromosomal Microarray Analysis (CMA) are commonly used. These methods can detect aneuploidy across all 23 pairs of chromosomes. NGS, in particular, provides a high-resolution analysis of the DNA, allowing for the detection of even subtle chromosomal abnormalities.
- PGT-M and PGD Analysis: For PGT-M and PGD, specific DNA probes are used to target the gene or chromosomal region of concern. The analysis confirms whether the embryo carries the specific mutation or translocation that the couple wishes to avoid.
- Reporting and Interpretation: Once the genetic analysis is complete, a detailed report is generated. This report will indicate whether each biopsied embryo is euploid (chromosomally normal), aneuploid, or carries the specific genetic defect being screened for. Fertility specialists and genetic counselors then review these results with the prospective parents, explaining the findings in detail and discussing the implications for embryo selection.
Embryo Selection and Transfer
Based on the PGT results and other clinical factors, the couple and their medical team will decide which embryos are suitable for transfer. The goal is to select the genetically healthiest embryo(s) to maximize the chances of a successful pregnancy and minimize the risk of genetic complications.
- Informed Decision-Making: The interpretation of PGT results is crucial for informed decision-making. A genetically normal embryo, according to the PGT testing, is considered to have a higher probability of implantation and successful development. Conversely, embryos identified with significant aneuploidy or specific genetic disorders are typically not recommended for transfer.
- Single Embryo Transfer (SET): In many cases, PGT, particularly PGT-A, supports the practice of Single Embryo Transfer (SET). By identifying a chromosomally normal embryo, the likelihood of a successful pregnancy with just one embryo is increased, thereby reducing the risks associated with multiple pregnancies (e.g., premature birth, low birth weight, preeclampsia).
Who Can Benefit from PGT?
The decision to pursue PGT is a deeply personal one, and it is not a routine recommendation for all individuals undergoing IVF. However, there are specific circumstances and patient profiles where PGT can offer significant advantages and peace of mind.
Indications for PGT
Several factors can lead a couple or individual to consider PGT as part of their fertility treatment journey. These indications are generally categorized based on the genetic risks or reproductive challenges faced.
- Advanced Maternal Age: As women age, the incidence of aneuploidy in their eggs and consequently in their embryos increases significantly. For women over the age of 35, PGT-A can help identify chromosomally normal embryos, potentially improving IVF success rates and reducing the risk of miscarriages associated with aneuploidy.
- Recurrent Pregnancy Loss: For individuals or couples who have experienced multiple failed IVF cycles or recurrent miscarriages, PGT can help identify aneuploid embryos as a potential cause. By transferring chromosomally normal embryos, the chances of a successful pregnancy may be improved.
- Known Genetic Carrier Status: If one or both partners are known carriers of a specific single-gene disorder (e.g., cystic fibrosis, Huntington’s disease, beta-thalassemia) or a balanced chromosomal translocation, PGT-M or PGD is highly recommended. This allows them to avoid passing on the specific genetic condition to their child.
- Previous Child with a Chromosomal or Genetic Abnormality: If a couple has previously had a child diagnosed with a chromosomal abnormality or a specific genetic disorder, PGT can be used to screen future embryos to prevent the recurrence of that condition.
- Severe Male Factor Infertility: While not as strongly indicated as other factors, some studies suggest that PGT-A might offer marginal benefits in cases of severe male factor infertility, where the quality and chromosomal integrity of sperm might be compromised.
Counseling and Ethical Considerations
The decision to undergo PGT is not solely a medical one; it also involves significant ethical and psychosocial considerations. Comprehensive genetic counseling is an integral part of the PGT process.
- Genetic Counseling: Genetic counselors play a vital role in educating prospective parents about the intricacies of PGT, including the types of tests available, their limitations, and the potential implications of the results. They discuss the risks and benefits, address any concerns, and help individuals make informed decisions aligned with their values and family planning goals.
- Ethical Debates: PGT has sparked ongoing ethical debates regarding its use, particularly concerning the potential for embryo selection based on non-medical traits (though current clinical practice strictly focuses on medical indications). Discussions around the definition of “genetic health,” the status of embryos, and the potential for a “slippery slope” are ongoing within the scientific and ethical communities. It is crucial for patients to understand that PGT is a medical tool to prevent disease and improve reproductive outcomes, not for selecting for desired non-medical traits.
The Impact and Future of PGT
Preimplantation Genetic Testing has significantly advanced the capabilities of assisted reproductive technologies, offering hope and greater control to individuals and couples navigating complex reproductive journeys. Its impact extends beyond simply achieving pregnancy, influencing the health and well-being of future generations.
Enhancing Reproductive Outcomes
The primary benefit of PGT lies in its ability to enhance reproductive outcomes for specific patient populations. By identifying and selecting genetically healthy embryos, PGT aims to:
- Increase Live Birth Rates: For women with advanced maternal age or those experiencing recurrent implantation failure, PGT-A can lead to higher implantation and live birth rates by ensuring that only chromosomally normal embryos are transferred.
- Reduce Miscarriage Rates: Aneuploidy is a leading cause of early miscarriage. By screening for and avoiding the transfer of aneuploid embryos, PGT can help reduce the incidence of pregnancy loss.
- Prevent the Transmission of Genetic Diseases: PGT-M and PGD are invaluable for couples at risk of passing on specific inherited disorders. They provide a way to ensure that their children are born free from these debilitating conditions.

Technological Advancements and Future Directions
The field of PGT is continuously evolving, driven by rapid advancements in genetic technologies and a deeper understanding of embryonic development.
- Improved Biopsy Techniques: Research is ongoing to develop even less invasive biopsy methods, potentially including non-invasive prenatal testing (NIPT) principles applied to embryos, although this is still largely in the research phase.
- Enhanced Diagnostic Accuracy: Next-Generation Sequencing (NGS) continues to be refined, offering greater accuracy and resolution in detecting chromosomal abnormalities. New analytical techniques are also being developed to interpret complex genetic data more effectively.
- Broader Genetic Screening: While current PGT focuses on specific single-gene disorders or aneuploidy, future developments might explore screening for a wider range of genetic predispositions or polygenic risk factors, though this is a complex area with significant ethical considerations.
- AI and Machine Learning: Artificial intelligence is beginning to be explored for its potential to analyze embryo images and genetic data, potentially assisting in predicting embryo viability and improving the efficiency of PGT analysis.
In conclusion, Preimplantation Genetic Testing represents a remarkable intersection of genetics, embryology, and reproductive medicine. It empowers individuals and couples with valuable information, allowing for more informed decisions and offering a pathway to a healthier genetic future. As technology continues to advance, PGT will undoubtedly play an even more significant role in optimizing reproductive health and providing peace of mind for families around the world.