Group B Streptococcus (GBS), often referred to as Group Strep B, is a common type of bacteria that can be found in the bodies of healthy adults, typically in the digestive or genitourinary tracts, without causing any illness. However, during pregnancy, GBS can pose a risk to both the mother and the newborn. Understanding GBS, its implications during pregnancy, and the preventative measures available is crucial for expectant parents and healthcare providers.
Understanding Group B Streptococcus (GBS)
Group B Streptococcus is a bacterium that naturally colonizes the lower gastrointestinal and genitourinary tracts of approximately 15-25% of healthy pregnant women. This colonization is usually asymptomatic, meaning the woman experiences no symptoms or discomfort. The presence of GBS in the pregnant individual is not considered an infection in the traditional sense, but rather a carrier state. The bacteria are typically harmless in this context.
What is GBS?
GBS is a Gram-positive, beta-hemolytic bacterium belonging to the Streptococcus genus. It is a common human commensal, meaning it lives on or in humans without typically causing harm. Its prevalence as a colonizer in the vaginal and rectal flora of women of childbearing age is well-established.
How is GBS Transmitted?
The transmission of GBS is generally not a concern for non-pregnant individuals. However, during labor and delivery, if a pregnant person is colonized with GBS, there is a risk that the bacteria can be transmitted to the baby as the infant passes through the birth canal. This intrapartum transmission is the primary pathway through which newborns can be exposed to GBS.
GBS Colonization vs. Infection
It is vital to distinguish between GBS colonization and GBS infection. Colonization refers to the presence of GBS bacteria without causing any symptoms or signs of illness. Infection occurs when the bacteria invade tissues and elicit an inflammatory response, leading to disease. While pregnant individuals are often colonized with GBS, this does not automatically mean they have a GBS infection. However, the colonization state creates the potential for transmission to the infant during birth.
Risks and Complications Associated with GBS in Pregnancy
While most GBS colonizations in pregnant women are benign, there are potential risks and complications, particularly for the newborn if GBS is transmitted during labor.
Risks to the Newborn
The most significant concern with GBS during pregnancy is the potential for early-onset GBS disease in newborns. This occurs when the baby acquires GBS from the mother during labor or delivery. Early-onset GBS disease typically manifests within the first 7 days of life and can lead to severe illness, including:
- Sepsis: A life-threatening bloodstream infection.
- Pneumonia: Infection of the lungs, causing breathing difficulties.
- Meningitis: Infection of the membranes surrounding the brain and spinal cord, which can lead to long-term neurological damage or death.
The severity of these conditions can be high, and prompt diagnosis and treatment are critical. While the overall risk of a baby developing early-onset GBS disease is relatively low, it is a significant concern for public health initiatives.
Risks to the Pregnant Person
While less common than neonatal GBS disease, GBS can also cause infections in the pregnant person. These can include:
- Urinary Tract Infections (UTIs): GBS is a known cause of UTIs in pregnant women.
- Chorioamnionitis: Infection of the amniotic fluid and membranes surrounding the fetus, which can lead to premature labor, fever, and complications for both mother and baby.
- Endometritis: Infection of the uterine lining after delivery.
- Bacteremia (sepsis): GBS can enter the bloodstream and cause a systemic infection in the mother.
These infections can pose serious health risks and require prompt medical attention.
Late-Onset GBS Disease
In addition to early-onset disease, newborns can also develop late-onset GBS disease, which typically occurs between 1 week and 3 months of age. This form is less commonly acquired during birth and may be due to other sources of exposure or reactivation of previously acquired bacteria. While less frequent than early-onset, late-onset GBS disease can still lead to serious complications.
Screening and Prevention Strategies
Given the potential risks, screening for GBS is a standard practice in prenatal care in many countries. The goal of screening is to identify pregnant individuals colonized with GBS so that preventative measures can be implemented during labor.
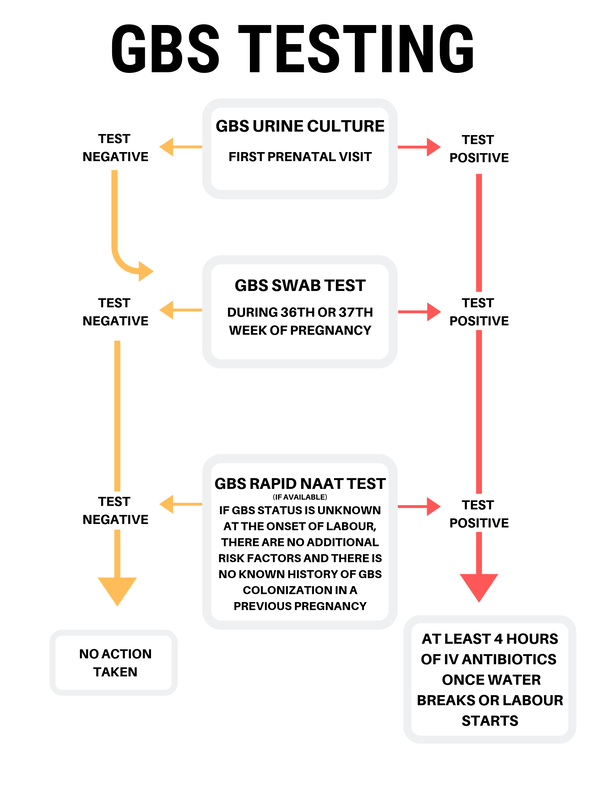
GBS Screening Process
GBS screening is typically performed between 35 and 37 weeks of gestation. The process involves a simple and painless swab of the lower vagina and rectum. The collected sample is then sent to a laboratory for testing to determine if GBS bacteria are present.
Importance of Universal Screening
In the United States, the Centers for Disease Control and Prevention (CDC) recommends universal GBS screening for all pregnant individuals between 35 and 37 weeks of gestation, regardless of whether they have any symptoms. This approach aims to identify all carriers and implement appropriate preventative measures.
Intrapartum Antibiotic Prophylaxis (IAP)
The primary method for preventing early-onset GBS disease in newborns is Intrapartum Antibiotic Prophylaxis (IAP). If a pregnant person is found to be GBS positive during screening, they will be offered intravenous (IV) antibiotics during labor. The antibiotics are typically administered once labor begins and continue periodically until delivery. The goal of IAP is to reduce the number of GBS bacteria in the birth canal, thereby minimizing the risk of transmission to the baby.
Criteria for IAP
IAP is recommended for pregnant individuals who meet certain criteria, including:
- Positive GBS screening culture: If a pregnant person’s screening culture result is positive for GBS.
- Unknown GBS status at labor: If GBS status is unknown at the onset of labor, IAP is recommended if any of the following risk factors are present:
- Preterm labor (before 37 weeks gestation).
- Rupture of membranes for 18 hours or longer.
- Intrapartum fever (temperature of 100.4°F or 38°C or higher).
- GBS bacteriuria: Presence of GBS in the urine during pregnancy, even if the vaginal/rectal culture is negative, as this indicates a higher bacterial load.
- Previous infant with GBS disease: If a previous child had GBS disease, the mother is considered high risk.
Types of Antibiotics Used
The most commonly used antibiotics for IAP are penicillin and ampicillin, as GBS is generally susceptible to these medications. For individuals with a penicillin allergy, alternative antibiotics such as clindamycin or vancomycin may be used, depending on the severity of the allergy and local resistance patterns.
Limitations of IAP
While IAP is highly effective in preventing early-onset GBS disease, it is not foolproof. Several factors can influence its effectiveness:
- Timing of antibiotics: Antibiotics need to be administered sufficiently before delivery to be effective. If labor is very rapid, the baby may be born before the antibiotics have had adequate time to work.
- Penicillin allergies: Some individuals have severe penicillin allergies, requiring alternative antibiotics that may be less effective or associated with higher resistance rates.
- GBS colonization changes: A pregnant person may become colonized with GBS between the time of screening and labor, or their bacterial load may fluctuate.
- Emergence of resistant strains: While rare, strains of GBS can develop resistance to antibiotics over time.
Alternative Prevention Strategies and Research
Ongoing research explores alternative and complementary strategies to further reduce the risk of GBS transmission and disease. These include:
- Vaccines: Development of a GBS vaccine is a significant area of research. A vaccine could potentially protect both pregnant individuals and their newborns by stimulating the production of protective antibodies before exposure.
- Non-antibiotic interventions: Research into non-antibiotic preventative measures is also underway, though these are generally not yet standard practice.
Managing GBS in Pregnancy: A Collaborative Approach
Effective management of GBS during pregnancy requires a collaborative approach involving healthcare providers and expectant parents. Open communication and adherence to recommended guidelines are paramount.
Communication with Healthcare Providers
It is essential for pregnant individuals to discuss GBS with their healthcare providers. Understanding the screening process, the rationale behind it, and the implications of a positive or unknown GBS status empowers patients to make informed decisions.
What to Expect During Labor
If you are identified as GBS positive or your status is unknown at the onset of labor, your healthcare team will discuss the plan for intrapartum antibiotic prophylaxis. Be sure to inform the labor and delivery staff about your GBS status and any allergies you may have.
Postpartum Care
While the primary focus is on preventing GBS transmission during birth, awareness of GBS in the postpartum period is also important. If a newborn develops symptoms suggestive of GBS infection, prompt medical evaluation and treatment are crucial. For the mother, any signs of infection, such as fever, abdominal pain, or unusual discharge, should be reported to a healthcare provider immediately.
Support and Resources
Navigating pregnancy and potential health concerns can be overwhelming. Various resources are available to provide support and information:
- Healthcare Providers: Your obstetrician, midwife, or pediatrician are your primary sources of information and care.
- Public Health Organizations: Organizations like the CDC and national health services provide comprehensive guidelines and patient information.
- Patient Advocacy Groups: Support groups and online communities can offer shared experiences and emotional support.
By understanding Group B Streptococcus, its potential impacts, and the established prevention strategies, expectant families can work closely with their healthcare providers to ensure the healthiest possible outcome for themselves and their newborns.