Gamekeeper’s thumb, also known medically as skier’s thumb or ulnar collateral ligament (UCL) injury of the thumb, is a common condition affecting the ligament on the inside of the thumb. While its name might evoke images of rural pursuits, its prevalence in sports like skiing and, importantly for our discussion, in activities involving the precise and often forceful manipulation of specialized equipment, highlights its significance. Understanding this injury is crucial for anyone engaging in hobbies or professions that demand dexterity and a strong grip, particularly within the realm of advanced technology.
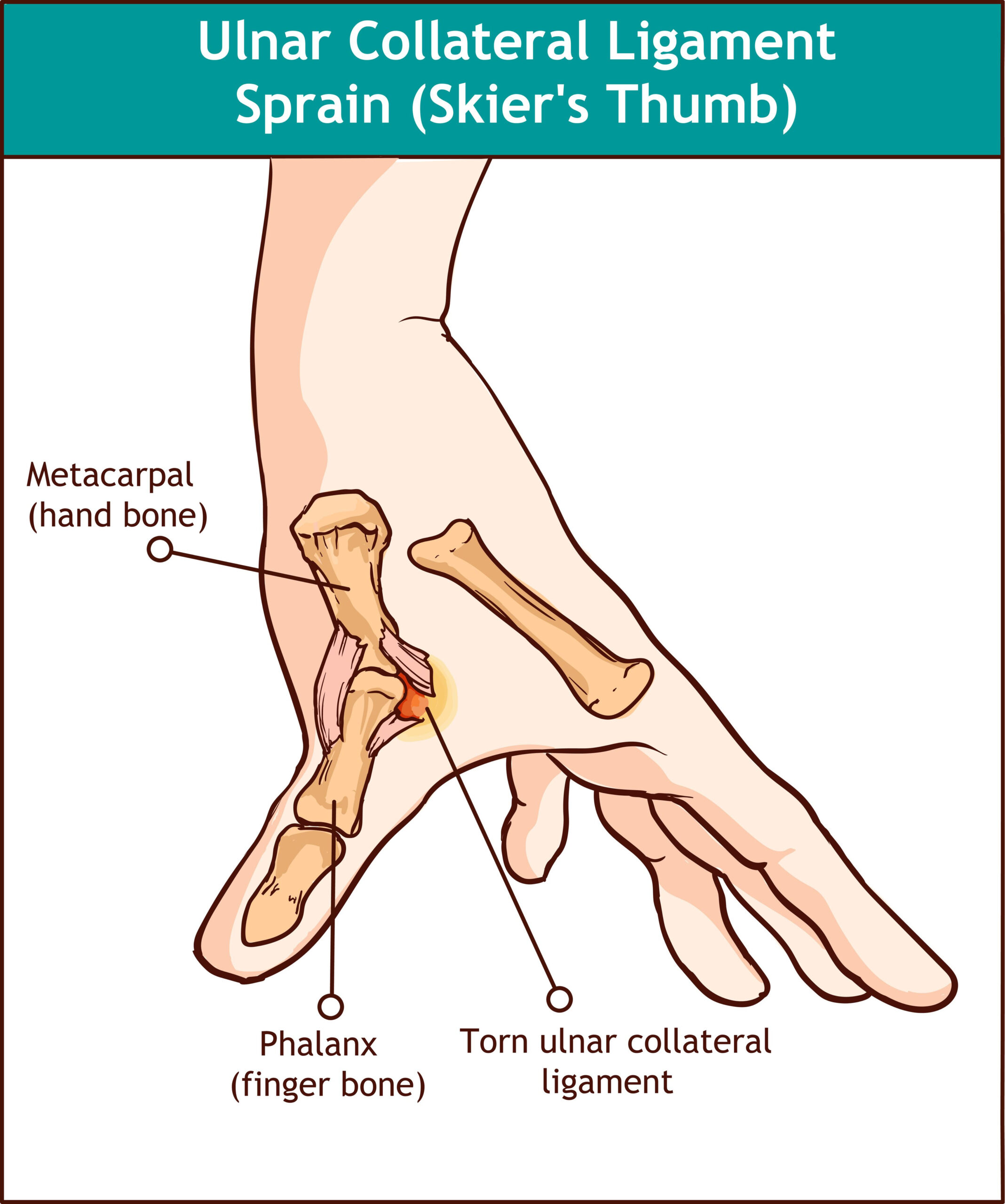
The thumb’s unique anatomy, with its broad range of motion and crucial role in grasping, makes it susceptible to injury. The ulnar collateral ligament (UCL) is the primary stabilizer of the metacarpophalangeal (MP) joint of the thumb. This joint, located at the base of the thumb where it meets the hand, is critical for pinch and grip strength. When this ligament is stretched or torn, it compromises the stability of the thumb, leading to pain, weakness, and a reduced ability to perform everyday tasks, let alone the intricate maneuvers required for operating sophisticated equipment.
The Anatomy and Biomechanics of the Thumb’s UCL
The thumb’s remarkable dexterity is largely attributed to its unique skeletal structure and the complex interplay of muscles and ligaments. At the core of its stability lies the ulnar collateral ligament (UCL) complex, a robust band of fibrous tissue that runs along the ulnar side (the side closest to the little finger) of the metacarpophalangeal (MP) joint. This ligament is not a single entity but rather a complex comprising several distinct components, each contributing to the overall stability of the joint.
The Structure of the UCL Complex
The UCL complex is typically described as having two primary components:
- Proper UCL: This is the main ligamentous band that originates from the apex of the metacarpal head and inserts onto the base of the proximal phalanx. It is the most significant stabilizer against valgus (outward) stress at the MP joint.
- Accessory UCL: This is a broader, flatter band of tissue that lies volar (towards the palm) to the proper UCL. It reinforces the joint capsule and provides additional stability, particularly against rotational forces.
These components work in concert with the surrounding joint capsule, volar plate, and intrinsic hand muscles to maintain the structural integrity and functional mobility of the thumb. The MP joint itself is a condyloid joint, allowing for flexion, extension, abduction, adduction, and circumduction. However, its stability relies heavily on the integrity of the UCL, especially during activities that involve forceful grasping, pinching, or rapid changes in direction of movement.
Biomechanical Importance in Grip and Dexterity
The thumb’s ability to oppose the other fingers is fundamental to human dexterity and our capacity to interact with the world. The UCL plays a pivotal role in enabling this opposition by providing the necessary stability to withstand the forces generated during gripping. When we grasp an object, particularly one that requires a strong pinch or a forceful hold, significant stress is placed on the MP joint. The UCL acts as a crucial restraint, preventing excessive outward movement (valgus deviation) of the proximal phalanx relative to the metacarpal.
This inherent stability is vital for tasks requiring fine motor control and precise manipulation. Consider the act of holding and operating a camera gimbal, a drone controller, or even intricate FPV goggles. These activities demand not only the ability to execute subtle movements but also the strength to maintain a firm grip under varying conditions. The UCL’s role in providing this stable base of support for the thumb is paramount in such scenarios. Without its full function, the precision and strength required for these tasks would be significantly compromised, leading to fumbling, reduced control, and potential further injury.
Causes and Mechanisms of Gamekeeper’s Thumb
The injury, colloquially known as gamekeeper’s thumb, historically arose from the repetitive, forceful ulnar deviation of the thumb used by gamekeepers when preparing to wring the necks of birds. Today, however, the most common mechanism of injury is an acute, forceful abduction or hyperextension of the thumb, often encountered in sports. For individuals engaged in the operation of drones and related technologies, specific scenarios can mimic these high-risk movements.
Acute Traumatic Injury
The most frequent cause of gamekeeper’s thumb is a sudden, forceful trauma to the thumb. This typically occurs when the thumb is forcibly bent backward (hyperextended) or outward (abducted) away from the palm, beyond its normal range of motion. This can happen through:
- Falls: A common scenario is falling onto an outstretched hand, where the thumb bears the brunt of the impact or is twisted unnaturally.
- Sports Injuries: In sports, direct blows to the thumb or forceful twisting motions during play are often implicated. This is why it’s also frequently referred to as “skier’s thumb,” as a fall while skiing can easily lead to this type of injury if the hand is planted or twisted.
- Accidental Twisting: In everyday life, a forceful twist or pull on the thumb can also cause the UCL to tear.
Repetitive Stress and Microtrauma
While acute injuries are more commonly associated with a complete tear, repetitive stress and microtrauma can also contribute to UCL insufficiency over time. This type of injury might not present with a single, dramatic event but rather a gradual weakening and stretching of the ligament due to repeated minor strains. In the context of drone operation, this could manifest in scenarios involving prolonged, repetitive, and forceful thumb movements.
- Constant Gripping and Adjustments: Extended periods of gripping a drone controller, especially one that is heavy or has buttons requiring significant pressure, can lead to cumulative stress. Repeatedly making fine adjustments to camera angles or flight controls with excessive force can also strain the UCL.
- Awkward Postures: Operating drones in challenging environments might necessitate holding the controller in awkward positions for extended durations. This can alter the biomechanics of the thumb and increase the risk of repetitive strain on the UCL.
- High-Performance Flying: For pilots engaged in FPV (First Person View) racing or intricate aerial acrobatics, the demands on the thumbs are exceptionally high. The rapid, precise, and often forceful stick movements required can create a significant and sustained load on the UCL, potentially leading to chronic irritation and eventual injury.

Symptoms and Diagnosis of a UCL Injury
The signs and symptoms of gamekeeper’s thumb can vary depending on the severity of the ligamentous tear. From a mild sprain to a complete rupture, the presentation will differ, necessitating a thorough diagnostic approach.
Clinical Manifestations of an Injured UCL
When the UCL is injured, several key symptoms emerge, indicating compromised thumb stability and function. These include:
- Pain: This is typically the most prominent symptom. Pain is usually localized to the ulnar side of the MP joint of the thumb. It can range from a dull ache with mild injuries to sharp, intense pain with more severe tears, especially when attempting to grasp or pinch. The pain may worsen with movement or pressure on the joint.
- Tenderness: The area over the UCL will be exquisitely tender to the touch. Palpating the ligament during a physical examination will elicit significant discomfort.
- Swelling: Inflammation around the MP joint is common, leading to visible swelling. This swelling can contribute to stiffness and discomfort.
- Bruising: In cases of significant trauma, bruising may be present around the injured area.
- Weakness: A hallmark symptom is a noticeable weakness in the thumb’s grip and pinch strength. The ability to firmly grasp objects, particularly those requiring a two-fingered pinch, is significantly impaired.
- Instability: The most concerning symptom of a significant UCL tear is a feeling of instability in the thumb. The thumb may feel “loose” or like it might “give out” when attempting to exert force. This is a direct consequence of the compromised ligamentous support.
- Limited Range of Motion: Pain and swelling can restrict the thumb’s normal range of motion, making it difficult to fully flex, extend, or abduct the digit.
Diagnostic Procedures and Imaging
Diagnosing gamekeeper’s thumb involves a combination of a thorough medical history, a detailed physical examination, and, in some cases, imaging studies to confirm the extent of the injury.
- Medical History: The physician will inquire about the mechanism of injury, including how and when the injury occurred, the type of activity being performed at the time, and the onset and nature of the symptoms. This is crucial for understanding the forces that may have been applied to the thumb.
- Physical Examination: The physical examination is paramount. The physician will:
- Palpate: Gently press on the UCL to identify the precise location of tenderness.
- Assess Range of Motion: Evaluate active and passive range of motion of the thumb, noting any limitations or pain.
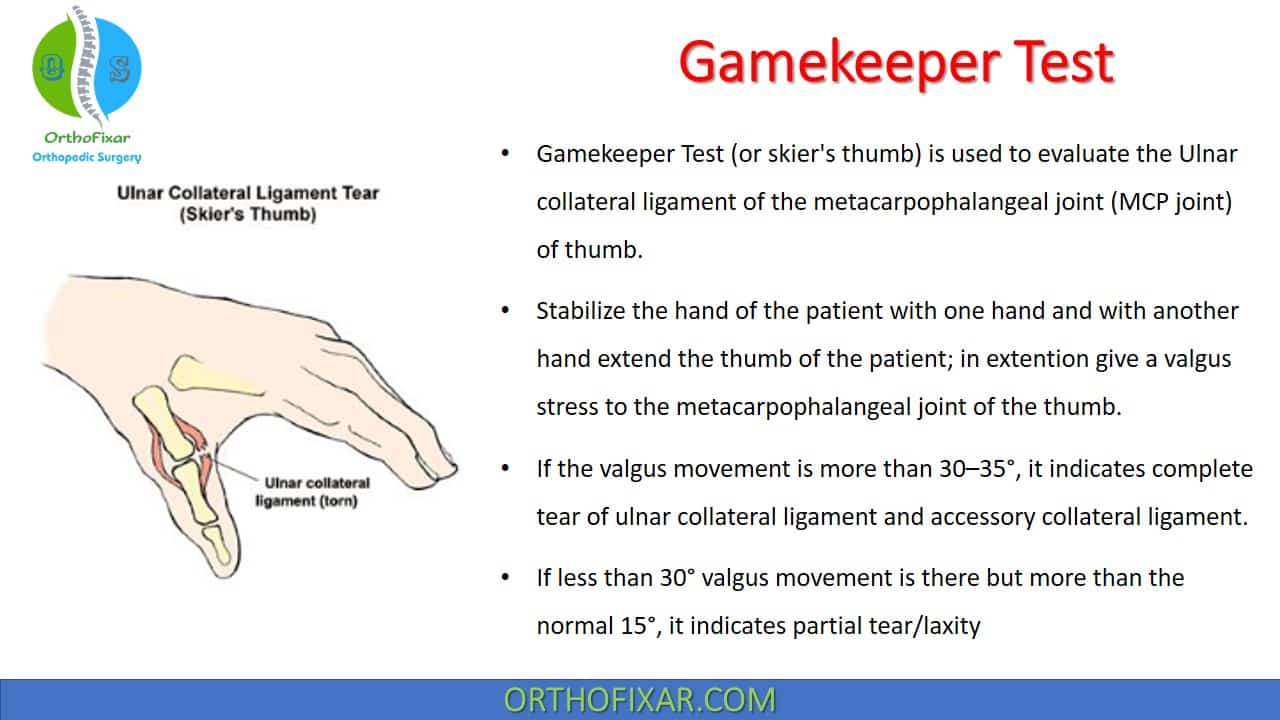
- Stress Testing: The most critical part of the physical exam is the valgus stress test. The examiner stabilizes the metacarpal bone and gently applies an outward force to the proximal phalanx. In a healthy thumb, there is very little “give.” However, in an injured UCL, the joint will open up excessively, indicating ligamentous laxity. The degree of opening (measured in degrees) helps classify the severity of the tear.
- Assess Grip and Pinch Strength: Compare the strength of the injured thumb to the uninjured thumb.
- Imaging Studies:
- X-rays: X-rays are routinely performed to rule out associated fractures of the metacarpal or phalanges. They can also sometimes reveal evidence of chronic injury or displacement of the ligament’s attachment if a bone fragment is pulled away (avulsion fracture).
- Ultrasound: Ultrasound can be a valuable tool for visualizing the UCL and assessing for tears, particularly partial tears and thickening of the ligament. It allows for dynamic assessment of the ligament during stress testing.
- MRI (Magnetic Resonance Imaging): MRI is the most sensitive imaging modality for evaluating soft tissue injuries, including complete UCL tears, partial tears, and associated injuries to other structures around the thumb. It provides detailed cross-sectional images of the ligament and surrounding tissues, helping to precisely define the extent of the damage.
Treatment and Rehabilitation for Gamekeeper’s Thumb
The treatment approach for gamekeeper’s thumb is tailored to the severity of the injury, ranging from conservative management for mild sprains to surgical intervention for complete tears or unstable injuries. The ultimate goal of treatment is to restore the thumb’s stability, strength, and full range of motion, enabling a return to all desired activities, including the precise demands of operating advanced technological equipment.
Conservative Management
For milder injuries, such as Grade I (sprain) and some Grade II (partial tear) injuries, conservative treatment is often effective. This approach focuses on RICE principles and gradual rehabilitation:
- Rest: Avoiding activities that aggravate the pain and stress the thumb is crucial. This may mean temporarily ceasing drone operation or modifying how it is performed.
- Ice: Applying ice packs to the affected area for 15-20 minutes several times a day helps reduce swelling and pain.
- Compression: A compression bandage can provide support and help manage swelling.
- Elevation: Keeping the hand elevated above the heart level further aids in reducing swelling.
- Immobilization: A splint or brace, often a thumb spica cast or custom-molded splint, is typically used to immobilize the thumb and allow the ligament to begin healing. This immobilization period can range from a few weeks to several months, depending on the severity.
- Pain Management: Over-the-counter pain relievers like ibuprofen or naproxen can help manage pain and inflammation. Prescription pain medication may be used for more severe pain.
Surgical Intervention
Complete tears of the UCL (Grade III injuries) or injuries where the ligament has pulled away from the bone (avulsion fractures) often require surgical repair. Surgical intervention is also considered if conservative management fails to provide adequate stability or if there is significant joint instability. The primary goals of surgery are to:
- Repair the Torn Ligament: The surgeon will reattach the torn ligament to its original insertion point on the bone, often using sutures, anchors, or small screws.
- Reconstruct the Ligament: In cases of chronic injury or significant stretching, the surgeon may need to reconstruct the ligament using a tendon graft taken from another part of the body.
The surgical procedure is typically followed by a period of immobilization, similar to conservative management, to allow the repaired ligament to heal properly.
Rehabilitation and Return to Activity
Regardless of the treatment method, a comprehensive rehabilitation program is essential for a successful recovery. This program is designed to gradually restore:
- Range of Motion: Gentle exercises are initiated to regain the full flexibility of the thumb and MP joint.
- Strength: As pain and swelling subside, strengthening exercises are introduced to rebuild the muscles that support the thumb and hand. This is particularly important for restoring grip and pinch strength.
- Dexterity and Fine Motor Skills: Exercises that mimic the precise movements required for everyday tasks and specialized hobbies are incorporated. For drone pilots, this might involve practicing simulated flight control movements or handling small objects with precision.
- Proprioception and Stability: Exercises to improve the sense of joint position and enhance the dynamic stability of the thumb are crucial for preventing re-injury.
The timeline for returning to specific activities, such as operating drones, will depend on the individual’s healing progress, the severity of the injury, and the demands of the activity. A phased return to activity, starting with lighter tasks and gradually increasing intensity and duration, is usually recommended. Close communication with a physical therapist or hand specialist is vital throughout the rehabilitation process to ensure a safe and effective return to optimal function.