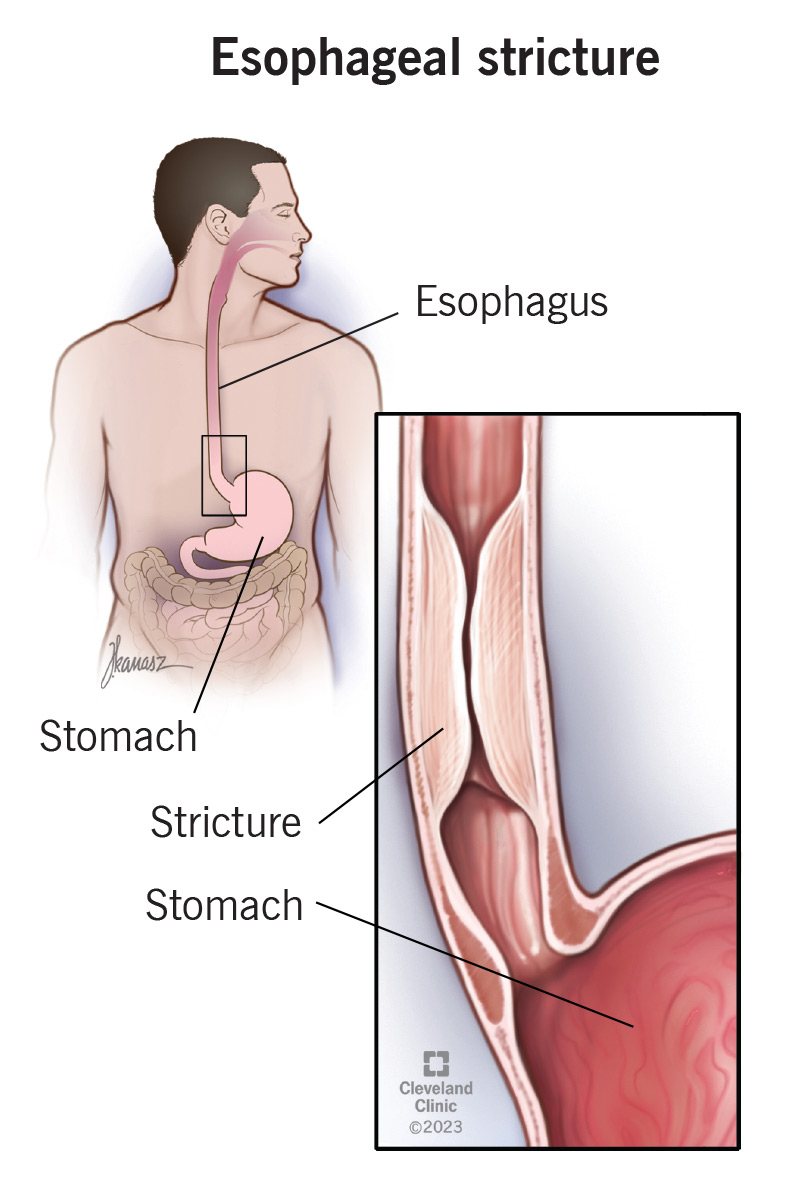
Esophageal stenosis, a condition characterized by the narrowing of the esophagus, presents a significant challenge to normal physiological functions, most notably swallowing. This stricture can impede the passage of food and liquids from the mouth to the stomach, leading to a cascade of symptoms and potential complications. Understanding the underlying causes, diagnostic approaches, and treatment strategies is crucial for managing this often-debilitating condition. The esophagus, a muscular tube extending from the pharynx to the stomach, relies on its flexibility and coordinated muscular contractions (peristalsis) to propel ingested materials. When stenosis occurs, this vital process is compromised, impacting an individual’s quality of life and nutritional status.
Causes of Esophageal Stenosis
The development of esophageal stenosis is rarely a spontaneous event. It is typically the consequence of damage to the esophageal lining, which then leads to scarring and subsequent narrowing. This damage can stem from a variety of insults, each with its own pathological pathway.
Inflammatory and Infectious Causes
Chronic inflammation of the esophagus, known as esophagitis, is a leading contributor to stenosis. Several conditions can precipitate severe esophagitis:
Gastroesophageal Reflux Disease (GERD)
Long-standing and severe GERD is perhaps the most common culprit. Stomach acid that repeatedly flows back into the esophagus irritates and damages the delicate lining. Over time, this chronic inflammation can lead to the formation of scar tissue, which contracts and narrows the esophageal lumen. In severe cases, this can progress to a peptic stricture.
Eosinophilic Esophagitis (EoE)
This allergic inflammatory condition, often triggered by food allergens, causes a buildup of eosinophils (a type of white blood cell) in the esophageal wall. Chronic inflammation and subsequent fibrosis in EoE can also result in esophageal narrowing, particularly in the mid-to-distal esophagus.
Infections
Certain infections, though less common in developed countries, can cause esophageal inflammation and stenosis. Viral infections like herpes simplex virus (HSV) or cytomegalovirus (CMV) can lead to ulcerations that, upon healing, can form strictures. Fungal infections, such as Candida esophagitis, can also cause severe inflammation and, in immunocompromised individuals, potentially lead to scarring.
Mechanical and Traumatic Causes
Direct injury to the esophagus can also result in stenosis:
External Trauma
Penetrating injuries to the neck or chest that involve the esophagus can cause direct damage. While immediate surgical repair is often prioritized, the subsequent healing process can involve significant scarring and lumenal narrowing. Blunt trauma, though less likely to cause direct esophageal injury, can sometimes lead to contusion and subsequent stricture formation.
Ingestion of Caustic Substances
Accidental or intentional ingestion of corrosive materials, such as strong acids or alkalis, can cause severe chemical burns to the esophageal lining. These burns trigger an intense inflammatory response and significant tissue damage, leading to extensive scarring and potentially multiple, long esophageal strictures. The severity of the stenosis is directly proportional to the concentration and amount of the ingested substance.
Foreign Bodies
Prolonged impaction of a foreign body within the esophagus can lead to pressure necrosis and inflammation. If the foreign body remains lodged for an extended period, it can cause ulceration and eventual stricture formation at the site of impaction.
Iatrogenic Causes
Medical interventions themselves can inadvertently lead to esophageal damage:
Radiation Therapy
Radiation therapy to the chest or neck for cancers can damage the esophageal lining. The radiation causes inflammation and fibrosis, which can lead to a gradual narrowing of the esophagus, often developing months or years after treatment. The extent of the stenosis depends on the radiation dose and the area treated.
Endoscopic Procedures
While diagnostic and therapeutic endoscopy is generally safe, repeated or aggressive procedures, such as dilations for benign strictures or endoscopic mucosal resection (EMR) for early cancers, can sometimes cause further injury or scarring, potentially exacerbating existing stenosis or creating new ones. Post-operative strictures following esophageal surgery are also a concern.
Malignant Causes
Cancer originating in the esophagus or adjacent structures can cause obstruction and symptoms mimicking benign stenosis:
Esophageal Cancer
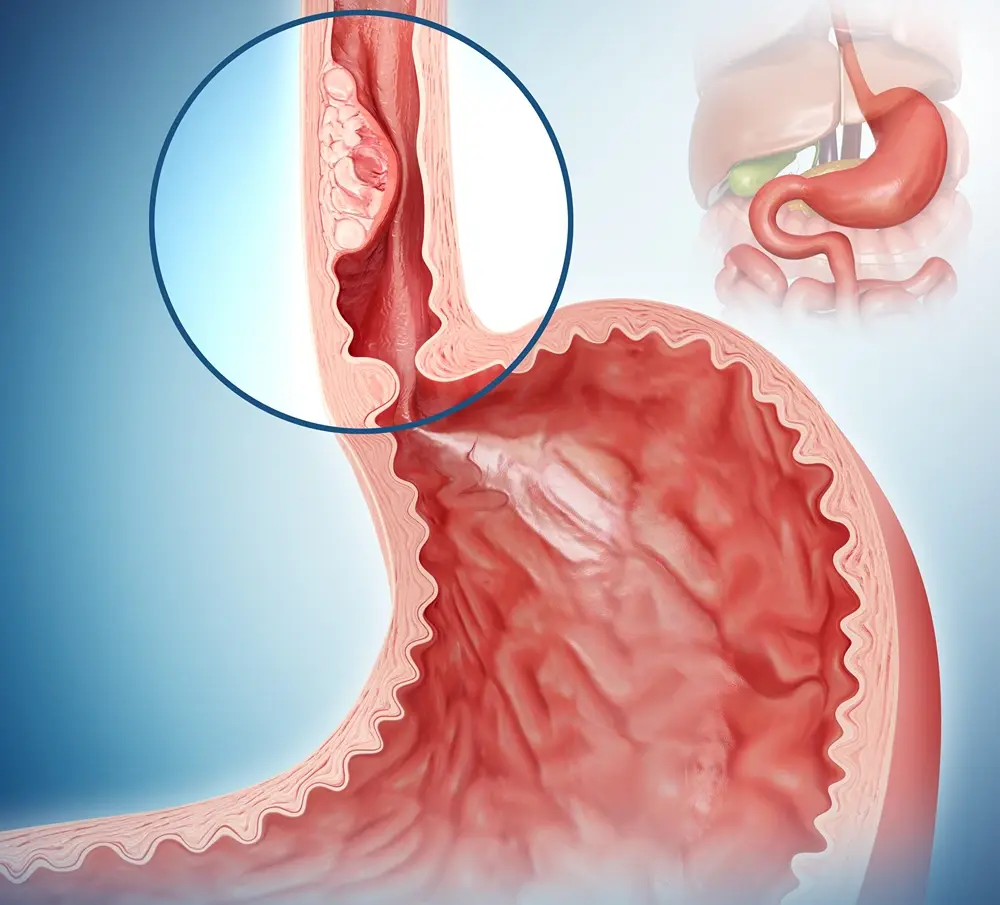
Tumors arising from the esophageal lining itself (e.g., squamous cell carcinoma, adenocarcinoma) can grow and obstruct the lumen. While malignant strictures are often irregular and associated with other cancer symptoms like weight loss and bleeding, they can present initially with dysphagia, making differentiation from benign causes critical.
Extrinsic Compression
Cancers of the lung, thyroid, or mediastinum can compress the esophagus externally, leading to narrowing and dysphagia.
Symptoms of Esophageal Stenosis
The hallmark symptom of esophageal stenosis is dysphagia, the difficulty or inability to swallow. The presentation and severity of dysphagia can vary widely depending on the degree and location of the narrowing.
Early Symptoms
In the initial stages of stenosis, individuals may experience:
Sensation of Food Sticking
A common complaint is the feeling of food getting “stuck” in the chest after swallowing, particularly with solid foods. This sensation can be intermittent and may improve with drinking water.
Odynophagia (Painful Swallowing)
In cases of active inflammation or ulceration associated with the stenosis, swallowing can become painful. This is more common in conditions like severe esophagitis or active chemical burns.
Advanced Symptoms
As the stenosis progresses, symptoms become more pronounced and debilitating:
Progressive Dysphagia
The difficulty in swallowing worsens over time, and it may start to affect softer foods and eventually liquids. Individuals may unconsciously alter their diet to softer, easier-to-swallow foods, leading to nutritional deficits.
Regurgitation and Vomiting
If food cannot pass through the narrowed segment, it can be regurgitated back into the mouth, often undigested. In severe cases, this can lead to vomiting, especially after attempting to eat.
Weight Loss and Malnutrition
The inability to consume adequate calories and nutrients due to dysphagia can lead to significant unintended weight loss and malnutrition. This can have profound effects on overall health and well-being.
Chest Pain
While not always present, some individuals experience chest pain, which can be associated with the passage of food or as a result of esophageal spasms.
Aspiration
In severe cases, when food or liquids cannot pass the obstruction, they can be aspirated into the airways, leading to coughing, choking, and an increased risk of pneumonia.
Diagnosis of Esophageal Stenosis
Diagnosing esophageal stenosis involves a combination of patient history, physical examination, and diagnostic imaging and endoscopic procedures. The goal is to identify the presence of a stricture, determine its cause, and assess its severity.
Diagnostic Tools and Procedures
Barium Esophagography (Barium Swallow)
This is often the initial diagnostic imaging study. The patient swallows a contrast agent (barium sulfate), which coats the lining of the esophagus. X-rays are then taken to visualize the passage of barium. A narrowed segment, irregular contours, or pooling of barium can indicate a stricture. This study can provide information about the length, location, and severity of the stenosis.
Esophagoscopy (Esophageal Endoscopy)
This is a crucial diagnostic and often therapeutic procedure. A flexible, lighted tube with a camera (endoscope) is inserted through the mouth and down into the esophagus. This allows for direct visualization of the esophageal lining, enabling the identification of inflammation, ulcers, tumors, or scar tissue. Biopsies can be taken during endoscopy to determine the cause of the inflammation or to rule out malignancy.
Esophageal Manometry
While not directly diagnosing stenosis, manometry can assess the muscular function of the esophagus and identify any associated motility disorders that might contribute to dysphagia.
pH Monitoring
For suspected GERD-related strictures, ambulatory 24-hour esophageal pH monitoring can help quantify the amount of acid reflux.
Computed Tomography (CT) Scan or Magnetic Resonance Imaging (MRI)
These imaging modalities are particularly useful for evaluating extrinsic compression of the esophagus by tumors or enlarged lymph nodes, and for assessing the extent of esophageal wall thickening in cases of malignancy or severe inflammation.
Management and Treatment of Esophageal Stenosis
The treatment of esophageal stenosis aims to alleviate dysphagia, improve nutritional status, and address the underlying cause. The approach is tailored to the individual patient based on the etiology, severity, and location of the stricture.
Endoscopic Interventions
Esophageal Dilation
This is the cornerstone of treatment for most benign esophageal strictures. Using a variety of dilators (e.g., Savary-Gillard dilators, balloon dilators), the narrowed segment of the esophagus is stretched open. This procedure is typically performed under sedation and may need to be repeated at intervals to maintain the lumen size. For complex or tight strictures, endoscopic ultrasound-guided balloon dilation may be employed.
Bougienage
Similar to dilation, bougienage involves passing progressively larger graduated tubes (bougies) through the narrowed area.
Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD)
In select cases of early esophageal cancer or high-grade dysplasia that can cause stricturing, these endoscopic techniques can be used to remove the abnormal tissue.
Stent Placement
For patients who are poor surgical candidates or when dilation is not sufficiently effective, esophageal stents (self-expanding metal stents or biodegradable stents) can be placed endoscopically to mechanically hold the esophagus open. These can provide significant relief but carry risks of complications such as stent migration, perforation, or tumor ingrowth.
Surgical Interventions
Surgery is generally reserved for cases where endoscopic treatment is unsuccessful, for very long or complex strictures, or when malignancy is suspected or confirmed.
Esophageal Strictureplasty
This surgical procedure involves incising the stenotic segment longitudinally and then closing it transversely to widen the lumen.
Esophagectomy
In cases of advanced esophageal cancer causing severe stenosis, or for very extensive benign strictures, a portion or all of the esophagus may need to be removed (esophagectomy) and reconstructed, often using a segment of the stomach or colon.
Medical Management
Proton Pump Inhibitors (PPIs)
For strictures related to GERD or eosinophilic esophagitis, long-term treatment with PPIs is essential to reduce acid exposure and inflammation, which can help prevent further scarring and may even promote some healing.
Immunosuppressive Therapy
In cases of eosinophilic esophagitis, dietary modifications and sometimes topical or systemic corticosteroids are used to control the inflammation.
Nutritional Support
For patients experiencing significant weight loss and malnutrition, nutritional support is vital. This may involve dietary modifications, oral nutritional supplements, or in severe cases, nasogastric tube feeding or percutaneous endoscopic gastrostomy (PEG) tube placement.

Lifestyle and Dietary Modifications
For strictures related to GERD, patients are advised to avoid trigger foods, eat smaller meals, avoid lying down after eating, and elevate the head of their bed. A soft diet may be recommended to ease the passage of food.
In conclusion, esophageal stenosis is a multifaceted condition with diverse etiologies. Effective management hinges on accurate diagnosis and a personalized treatment plan that may involve a combination of endoscopic, surgical, and medical interventions. Addressing the underlying cause, alongside symptomatic relief, is paramount to restoring the patient’s ability to swallow and improving their quality of life.