Understanding Trisomies and Their Genetic Basis
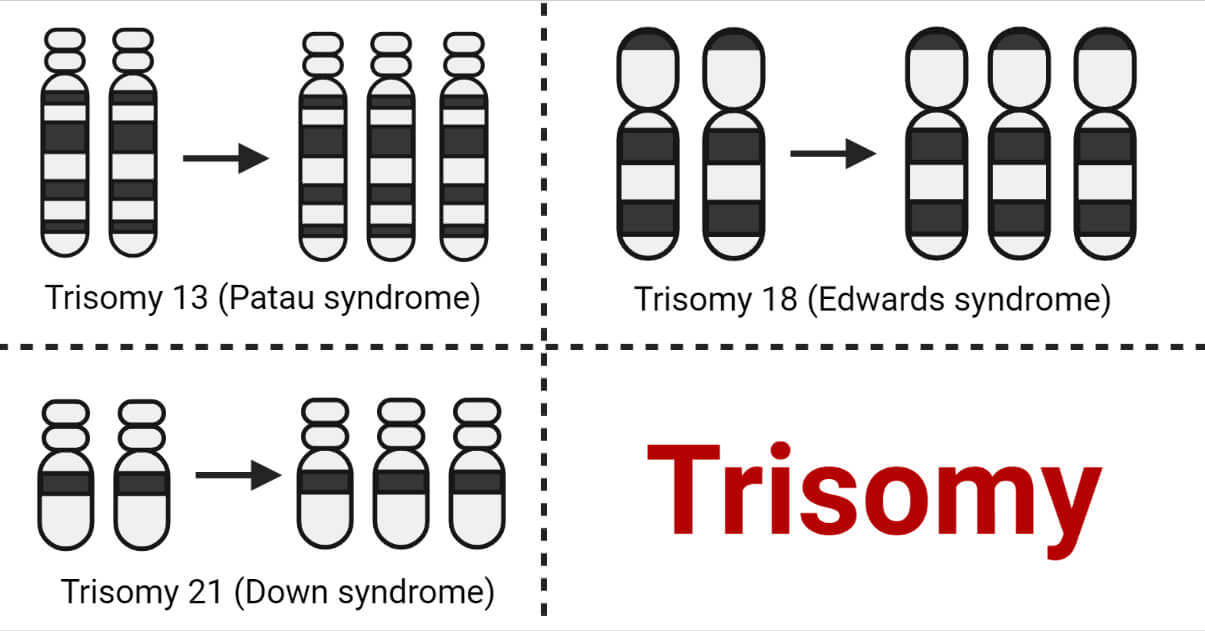
The human genome is a complex and intricate blueprint, meticulously organized into 23 pairs of chromosomes. These chromosomes carry our genetic information, dictating a vast array of traits and functions. While variations in this blueprint are common and often benign, certain chromosomal abnormalities can have profound implications for development and health. Among these, trisomies – a condition where an individual has three copies of a particular chromosome instead of the usual two – are particularly significant. This article will delve into three specific trisomies: Trisomy 21 (Down syndrome), Trisomy 18 (Edwards syndrome), and Trisomy 13 (Patau syndrome), exploring their genetic underpinnings and the developmental characteristics associated with each.
The Foundation of Heredity: Chromosomes and Genes
Before examining specific trisomies, it’s crucial to understand the fundamental role of chromosomes. Chromosomes are thread-like structures found within the nucleus of cells, composed of DNA tightly wound around proteins. Genes, segments of DNA, are the functional units that carry instructions for building and operating an organism. Humans typically possess 46 chromosomes, arranged in 23 homologous pairs. One set of 23 chromosomes is inherited from the mother, and the other set of 23 is inherited from the father. This organized structure ensures that each cell receives a complete and balanced set of genetic information.
The process of cell division, particularly meiosis, is responsible for producing gametes (sperm and egg cells) with half the number of chromosomes (23). Errors can occur during meiosis, leading to gametes with an abnormal number of chromosomes. When such a gamete fuses with a normal gamete during fertilization, the resulting zygote will have an extra chromosome, a condition known as aneuploidy. Trisomy is a specific type of aneuploidy where there is an extra copy of an entire chromosome.
Trisomy 21: The Most Common Autosomal Trisomy
Trisomy 21, commonly known as Down syndrome, is the most prevalent chromosomal disorder in humans, occurring in approximately 1 in every 700 to 1,000 live births. It is characterized by the presence of an extra copy of chromosome 21, meaning individuals with Down syndrome have three copies of this chromosome instead of the usual two.
Genetic Basis of Trisomy 21
The vast majority of Trisomy 21 cases (about 95%) arise from a meiotic error called nondisjunction. This occurs when homologous chromosomes fail to separate properly during the formation of egg or sperm cells. In the case of Trisomy 21, nondisjunction during meiosis I or meiosis II in either the mother or father leads to the formation of a gamete with two copies of chromosome 21. Upon fertilization with a normal gamete, the resulting embryo will have three copies of chromosome 21.
Less commonly, a condition called mosaic Down syndrome can occur. In this scenario, nondisjunction happens after fertilization, during early embryonic development. This results in a mixture of cells in the body, some with the normal two copies of chromosome 21, and others with three copies. The severity of characteristics in mosaic Down syndrome can vary depending on the proportion of cells with the extra chromosome.
A very rare form, translocation Down syndrome, accounts for about 3-4% of cases. In this type, a portion of chromosome 21 becomes attached to another chromosome, typically chromosome 14. While the individual may have the usual 46 chromosomes, the extra genetic material from chromosome 21 leads to the features of Down syndrome. Translocation Down syndrome can sometimes be inherited from a parent who is a carrier of the balanced translocation.
Developmental Characteristics of Trisomy 21
The presence of an extra copy of chromosome 21 leads to a distinct set of physical and developmental characteristics. It’s important to emphasize that the expression and severity of these characteristics can vary significantly among individuals.
Common physical features often include:
- Facial features: Upward slanting eyes, a flattened facial profile, a small nose, and a protruding tongue.
- Body features: Short stature, a single deep crease across the palm of the hand (simian crease), a wider space between the first and second toes, and poor muscle tone (hypotonia) at birth.
Cognitive and developmental aspects are also significant:
- Intellectual disability: Individuals with Down syndrome typically have some degree of intellectual disability, ranging from mild to moderate.
- Developmental delays: Milestones such as sitting, crawling, and walking are often achieved later than in typically developing children.
- Speech and language development: Delays in speech and language are common.
- Social development: Despite developmental challenges, individuals with Down syndrome often exhibit strong social skills and a positive disposition.
Health considerations are also paramount:
- Congenital heart defects: These are common and can range in severity.
- Gastrointestinal issues: Problems such as blocked intestines or reflux can occur.
- Vision and hearing impairments: These are also frequently observed.
- Increased risk of certain infections and certain types of leukemia.
With appropriate medical care, early intervention services, and supportive environments, individuals with Down syndrome can lead fulfilling and meaningful lives, contributing to their communities in numerous ways.
Trisomy 18: Edwards Syndrome
Trisomy 18, also known as Edwards syndrome, is a more severe chromosomal disorder than Trisomy 21. It is characterized by the presence of an extra copy of chromosome 18. Trisomy 18 is significantly less common than Trisomy 21, occurring in about 1 in 5,000 live births. Unfortunately, it is also associated with a much higher rate of miscarriage and stillbirth, and infants born with this condition often have a significantly reduced life expectancy.
Genetic Basis of Trisomy 18
Similar to Trisomy 21, the overwhelming majority of Trisomy 18 cases (around 94%) are caused by nondisjunction during meiosis, resulting in a gamete with an extra copy of chromosome 18. This leads to a zygote with three copies of chromosome 18.
Mosaic Trisomy 18, where there is a mixture of cells with two and three copies of chromosome 18, accounts for about 5% of cases. The clinical presentation in mosaic Trisomy 18 can be variable but is generally less severe than in full Trisomy 18.
Translocation Trisomy 18, where a portion of chromosome 18 is attached to another chromosome, is the rarest form, accounting for less than 1% of cases.
Developmental Characteristics of Trisomy 18
The presence of an extra chromosome 18 leads to a wide range of serious developmental abnormalities affecting multiple organ systems.
Key physical characteristics often include:
- Growth retardation: Severe intrauterine growth restriction and low birth weight are common.
- Distinct facial features: A small head (microcephaly), a receding chin, a small mouth, and low-set ears are frequently observed.
- Hand and foot abnormalities: Clenched fists with overlapping fingers, particularly the second and fifth fingers over the third and fourth, and a prominent heel (rocker-bottom foot) are characteristic.
- Congenital heart defects: These are almost universally present and often complex, posing significant medical challenges.
- Gastrointestinal abnormalities: Such as an omphalocele (abdominal organs protruding outside the body) and intestinal malrotation.
- Central nervous system abnormalities: Including structural brain malformations.
- Genitourinary abnormalities: Such as kidney problems and undescended testes in males.
Cognitive and developmental outcomes are also severe:
- Profound intellectual disability: Infants with Trisomy 18 typically have severe intellectual disabilities and significant developmental delays.
- Failure to thrive: Many infants struggle with feeding and gaining weight.
- Neurological issues: Seizures are common.
Due to the severity and multiplicity of medical problems, the prognosis for infants with Trisomy 18 is often poor. While some individuals may survive into childhood, it is rare for them to live beyond their first year of life. Palliative care and focusing on comfort are often prioritized for affected infants and their families.
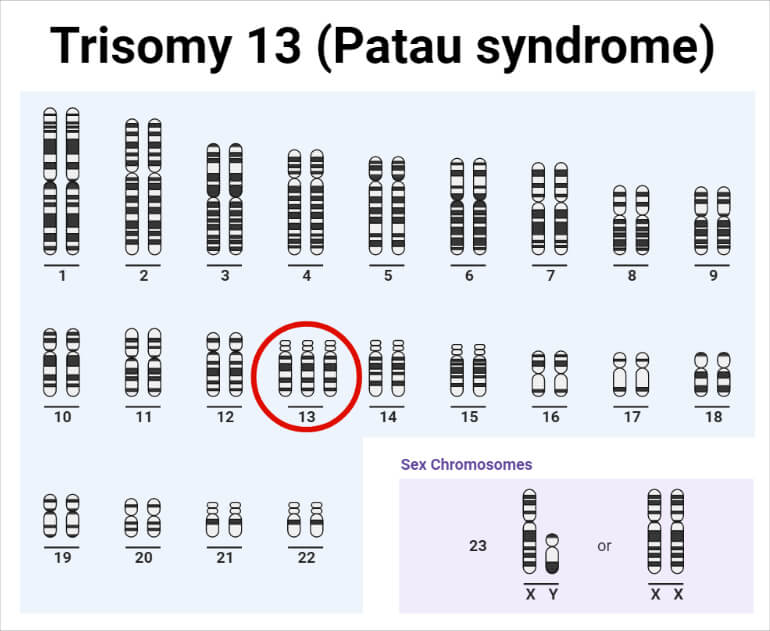
Trisomy 13: Patau Syndrome
Trisomy 13, known as Patau syndrome, is the least common and typically the most severe of these three autosomal trisomies. It is characterized by the presence of an extra copy of chromosome 13. Patau syndrome occurs in approximately 1 in 10,000 to 1 in 16,000 live births. Like Trisomy 18, it is associated with a high rate of miscarriage and stillbirth, and infants born with Patau syndrome have a very poor prognosis, with a high mortality rate in the first year of life.
Genetic Basis of Trisomy 13
The genetic basis for Trisomy 13 is predominantly nondisjunction during meiosis, leading to a gamete with an extra copy of chromosome 13. This results in a zygote with three copies of chromosome 13.
Mosaic Trisomy 13, where some cells have three copies of chromosome 13 and others have two, accounts for a small percentage of cases. The clinical features in mosaic cases can be less severe but still significant.
Translocation Trisomy 13 is also a rare cause, involving the attachment of a portion of chromosome 13 to another chromosome.
Developmental Characteristics of Trisomy 13
Patau syndrome is characterized by a wide array of severe physical and intellectual disabilities, often involving the brain, heart, kidneys, and limbs.
Prominent physical features typically include:
- Craniofacial abnormalities: The most striking features often involve the face, including severe midline defects. This can manifest as holoprosencephaly, a condition where the brain does not divide properly into two hemispheres. Other facial features may include a very small head (microcephaly), a sloping forehead, cleft lip and/or palate, and abnormal nose development.
- Eye abnormalities: Severe eye malformations are common, such as microphthalmia (abnormally small eyes) or cyclopia (a single eye).
- Polydactyly: The presence of extra fingers and toes is a frequent finding.
- Congenital heart defects: Significant heart abnormalities are present in most affected infants.
- Genitourinary defects: Kidney abnormalities are common.
- Umbilical or inguinal hernias.
Cognitive and developmental outcomes are extremely challenging:
- Severe intellectual disability: Infants with Trisomy 13 have profound intellectual disabilities.
- Developmental stagnation: Significant delays and lack of development are typical.
- Neurological dysfunction: Seizures and poor muscle tone are common.
Due to the severity of the medical issues, the majority of infants born with Trisomy 13 do not survive past the first few weeks or months of life. Survival beyond the first year is extremely rare. Medical management typically focuses on comfort care and supporting the family.
Diagnosis and Genetic Counseling
The diagnosis of Trisomy 21, 18, and 13 can be made during pregnancy through prenatal screening and diagnostic tests. Screening tests, such as nuchal translucency ultrasound and maternal serum screening, can assess the risk of these conditions. Diagnostic tests, like amniocentesis or chorionic villus sampling (CVS), can provide a definitive diagnosis by analyzing fetal chromosomes (karyotyping). These tests involve obtaining a sample of fetal cells to examine the number and structure of chromosomes.
Postnatally, a physical examination and genetic testing, such as karyotyping from a blood sample, can confirm the diagnosis of a trisomy.
Genetic counseling plays a vital role for families who receive a diagnosis of a trisomy. Genetic counselors can explain the condition, its inheritance patterns, the associated medical risks, and the available diagnostic and management options. They provide support and information to help families make informed decisions about prenatal testing, pregnancy management, and future reproductive planning.

Conclusion: Understanding Chromosomal Variations
Trisomy 21, 18, and 13 represent significant chromosomal abnormalities that arise from errors in cell division. While Trisomy 21 (Down syndrome) is associated with a range of characteristics and intellectual disability, individuals can lead fulfilling lives with appropriate support. Trisomy 18 (Edwards syndrome) and Trisomy 13 (Patau syndrome) are far more severe, often resulting in profound medical complications and significantly reduced life expectancy. Understanding the genetic basis and the diverse range of manifestations associated with these trisomies is crucial for medical professionals, families, and society to provide informed care, support, and compassion to affected individuals and their families. Advances in genetic technology continue to enhance our understanding of these complex conditions, paving the way for improved diagnostic capabilities and targeted support strategies.