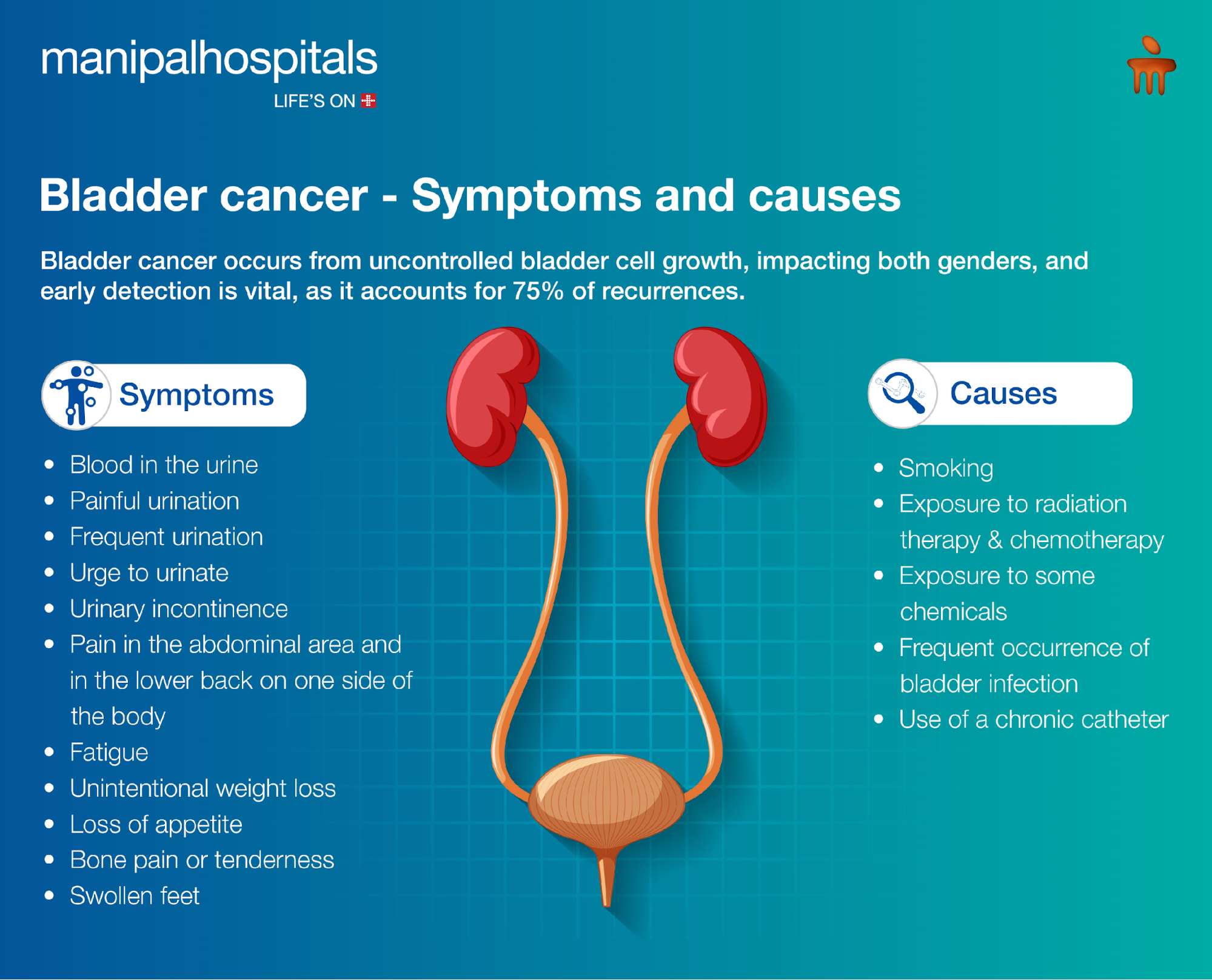
Bladder cancer is a disease that begins when cells in the bladder start to grow out of control. The bladder is a hollow, muscular organ that stores urine. Urine is produced by the kidneys and then travels down two tubes called ureters to the bladder. When the bladder is full, it signals to the brain that it’s time to urinate, and the urine exits the body through a tube called the urethra.
Most bladder cancers begin in the lining of the bladder, a layer of cells called the urothelium. This type of cancer is called urothelial carcinoma, and it’s the most common form of bladder cancer, accounting for about 90% of cases. If the cancer cells grow into deeper layers of the bladder wall, they can spread to other parts of the body.
Understanding the Different Types of Bladder Cancer
While urothelial carcinoma is the most prevalent, other less common types of bladder cancer exist, each with distinct characteristics and treatment approaches. Understanding these distinctions is crucial for accurate diagnosis and effective management.
Urothelial Carcinoma (Transitional Cell Carcinoma)
As mentioned, this is by far the most common type of bladder cancer. It originates in the urothelium, the inner lining of the bladder. Urothelial carcinoma can be further categorized into two main types based on how deeply the cancer cells have invaded the bladder wall:
Non-Muscle Invasive Bladder Cancer (NMIBC)
In this form, the cancer cells are confined to the innermost lining of the bladder (the urothelium) or have grown into the superficial layer beneath it (the lamina propria). NMIBC generally has a good prognosis, especially if detected and treated early. However, it has a higher risk of recurrence, meaning it can come back even after treatment. Regular follow-up is therefore essential.
Muscle-Invasive Bladder Cancer (MIBC)
This type of bladder cancer has grown through the inner lining and into the muscle layer of the bladder wall. MIBC is more aggressive and has a higher risk of spreading to other organs. Treatment for MIBC is more complex and often involves surgery, chemotherapy, and sometimes radiation therapy.
Squamous Cell Carcinoma
This type of bladder cancer arises from squamous cells, which are flat cells that can develop in the bladder lining, often in response to chronic irritation or infection. Squamous cell carcinoma is less common than urothelial carcinoma and is often associated with a history of bladder stones, urinary tract infections, or schistosomiasis (a parasitic infection common in some parts of the world). It can be more aggressive than urothelial carcinoma.
Adenocarcinoma
Adenocarcinoma develops from glandular cells in the bladder. These are the cells that normally produce mucus. This type of bladder cancer is rare, accounting for less than 2% of all cases. It can be more difficult to treat than urothelial carcinoma and may require more aggressive therapy.
Small Cell Carcinoma
This is a very rare and aggressive type of bladder cancer that begins in neuroendocrine cells within the bladder lining. Small cell carcinoma is often associated with smoking and can spread quickly to other parts of the body. It is typically treated with chemotherapy and sometimes radiation.
Other Rare Types
Very rarely, other types of cancer can occur in the bladder, including sarcomas (cancers that arise from connective tissues like muscle or blood vessels) and lymphomas (cancers of the lymphatic system). These are exceptionally uncommon and have their own specific diagnostic and treatment pathways.
Recognizing the Symptoms of Bladder Cancer
Early detection of bladder cancer significantly improves treatment outcomes. While some symptoms can be indicative of less serious conditions, persistent or recurring signs warrant prompt medical attention. It’s important to be aware of the potential warning signs and to consult a healthcare professional if you experience any concerning changes.
Blood in the Urine (Hematuria)
This is the most common and often the first noticeable symptom of bladder cancer. Hematuria can manifest in two ways:
Visible Blood (Gross Hematuria)
The urine may appear pink, red, or even brownish due to the presence of blood. This can occur suddenly and may or may not be accompanied by pain. Even a small amount of blood can cause the urine to change color.
Microscopic Blood (Microscopic Hematuria)
In this case, blood is not visible to the naked eye but can be detected during a routine urine test (urinalysis). While microscopic hematuria can be caused by various factors, it is still considered a significant finding that requires further investigation, especially in individuals with risk factors for bladder cancer.
Changes in Urinary Habits
Beyond the presence of blood, alterations in how and when you urinate can also be indicative of bladder cancer. These changes may include:
Frequent Urination
Feeling the need to urinate more often than usual, even when the bladder is not full, can be a symptom.
Urgent Need to Urinate
Experiencing a sudden, strong urge to urinate that is difficult to control.
Pain or Burning Sensation During Urination (Dysuria)
This symptom, while common in urinary tract infections, can also be associated with bladder cancer, particularly if it’s persistent or accompanied by other symptoms.
Difficulty Urinating or Weak Urine Stream
In some cases, a tumor can obstruct the flow of urine, leading to difficulty initiating urination or a weakened stream.
Other Potential Symptoms
While less common or more general, these symptoms can sometimes be associated with bladder cancer, especially in later stages or in conjunction with other signs:
Persistent Lower Back Pain or Pelvic Pain
If bladder cancer has spread to nearby lymph nodes or other organs, it can cause pain in the lower back or pelvic region.
Unexplained Fatigue or Weakness
As with many cancers, unexplained and persistent fatigue can be a sign of the disease.
Loss of Appetite and Unexplained Weight Loss
These are general symptoms that can accompany many serious illnesses, including advanced bladder cancer.
Factors That Increase the Risk of Developing Bladder Cancer
While anyone can develop bladder cancer, certain factors significantly increase an individual’s risk. Understanding these risk factors can empower individuals to make informed lifestyle choices and to be more vigilant about their health.
Smoking
This is by far the most significant risk factor for bladder cancer, accounting for approximately 50% of all cases. Chemicals in tobacco smoke are absorbed into the bloodstream and filtered by the kidneys, where they can damage the cells lining the urinary tract, including the bladder. The risk is dose-dependent, meaning the more a person smokes and the longer they smoke, the higher their risk.
Age
The risk of bladder cancer increases with age. The majority of cases are diagnosed in individuals over the age of 60.
Sex
Men are diagnosed with bladder cancer more often than women. This may be due to a combination of factors, including higher rates of smoking in men historically and potential hormonal influences.
Exposure to Certain Chemicals
Occupational exposure to certain chemicals, particularly dyes and rubber manufacturing industries, has been linked to an increased risk of bladder cancer. These chemicals, such as aromatic amines, can be carcinogenic.
Race and Ethnicity
While bladder cancer can occur in people of all racial and ethnic backgrounds, Caucasians are diagnosed with bladder cancer more frequently than African Americans and Hispanic Americans.
Certain Medical Conditions and Treatments
- Chronic Bladder Infections and Irritation: Long-term, recurrent bladder infections, bladder stones, or other conditions that cause chronic inflammation of the bladder lining can increase the risk of squamous cell carcinoma.
- Radiation Therapy to the Pelvic Area: Individuals who have undergone radiation therapy to the pelvic region for other cancers (e.g., prostate, cervical, or uterine cancer) have an increased risk of developing bladder cancer later in life.
- Certain Cancer Drugs: Some chemotherapy drugs, particularly cyclophosphamide, have been associated with an increased risk of bladder cancer.
Family History of Bladder Cancer
Having a first-degree relative (parent, sibling, or child) with bladder cancer can slightly increase an individual’s risk.
Certain Birth Defects of the Bladder
Rarely, certain congenital abnormalities of the bladder can be associated with an increased risk of cancer.
Diagnosis and Treatment of Bladder Cancer
If bladder cancer is suspected based on symptoms or risk factors, a healthcare provider will recommend a series of diagnostic tests to confirm the diagnosis and determine the extent of the cancer. Once diagnosed, a range of treatment options are available, tailored to the type, stage, and individual patient’s health.
Diagnostic Procedures
- Urinalysis and Urine Cytology: These tests examine urine for the presence of blood, abnormal cells, and other indicators of bladder cancer.
- Cystoscopy: This is a procedure where a thin, flexible tube with a camera (cystoscope) is inserted into the bladder through the urethra to visualize the bladder lining directly. Biopsies can be taken during cystoscopy if suspicious areas are found.
- Imaging Tests: CT scans, MRI scans, and ultrasounds can help determine the size and location of the tumor and whether it has spread to other parts of the body.
- Biopsy: A tissue sample taken from the bladder lining or from suspicious areas is examined under a microscope by a pathologist to confirm the presence and type of cancer.
Treatment Options
The treatment approach for bladder cancer is highly individualized and depends on several factors, including the stage and grade of the cancer, the patient’s overall health, and their preferences. Common treatment modalities include:
- Surgery:
- Transurethral Resection of Bladder Tumor (TURBT): For non-muscle-invasive bladder cancer, this procedure involves removing the tumor through the urethra using a special instrument.
- Radical Cystectomy: For muscle-invasive bladder cancer, this surgery involves removing the entire bladder, and sometimes nearby lymph nodes and organs (prostate and seminal vesicles in men, uterus, ovaries, and part of the vagina in women). Urinary diversion (creating a new way for urine to exit the body) is necessary after a cystectomy.
- Intravesical Therapy: This involves introducing medication directly into the bladder through a catheter.
- Bacillus Calmette-Guérin (BCG) Therapy: A weakened form of a tuberculosis vaccine that stimulates the immune system to attack cancer cells. Commonly used for non-muscle-invasive bladder cancer.
- Chemotherapy: Chemotherapy drugs can be instilled into the bladder to kill cancer cells.
- Chemotherapy: Systemic chemotherapy (given intravenously) is used to treat bladder cancer that has spread or is considered aggressive. It can be given before surgery to shrink tumors or after surgery to kill any remaining cancer cells.
- Radiation Therapy: High-energy rays are used to kill cancer cells. It is often used in combination with chemotherapy for muscle-invasive bladder cancer or for patients who are not candidates for surgery.
- Immunotherapy: Newer treatments that harness the body’s own immune system to fight cancer are also being developed and used.
Regular follow-up care, including cystoscopies, is crucial after treatment to monitor for recurrence.