Atrial fibrillation (AFib) is a common type of heart rhythm disorder characterized by a rapid and irregular heartbeat. This condition can lead to a variety of symptoms, including palpitations, shortness of breath, fatigue, and an increased risk of stroke. While medications are often the first line of treatment, they are not always effective or well-tolerated by all patients. For those who don’t find relief with drugs, or for whom medication is not suitable, a minimally invasive procedure called cardiac ablation offers a highly effective alternative. This article delves into the intricacies of AFib ablation, explaining what it is, how it works, and what patients can expect.

Understanding Atrial Fibrillation and its Underlying Causes
Before exploring ablation, it’s crucial to understand the electrical system of the heart. The heart’s rhythmic beating is controlled by electrical impulses generated by a specialized group of cells in the upper right chamber (atrium) called the sinoatrial (SA) node, the heart’s natural pacemaker. These impulses travel through the atria, causing them to contract and pump blood into the ventricles. A coordinated sequence of electrical events ensures efficient blood circulation throughout the body.
In AFib, the normal electrical signaling in the atria becomes chaotic. Instead of a single, organized impulse from the SA node, multiple rapid and irregular electrical signals erupt from various locations within the atria. These chaotic signals cause the atria to quiver or fibrillate rather than contract effectively. As a result, the ventricles receive these disorganized signals, leading to a rapid and irregular heartbeat.
The underlying causes of AFib are diverse and can include:
- Hypertension (High Blood Pressure): Chronic high blood pressure can strain the heart, leading to changes in the atria that predispose them to electrical abnormalities.
- Coronary Artery Disease: Narrowed or blocked coronary arteries can impair blood flow to the heart muscle, causing damage and increasing the risk of AFib.
- Heart Valve Disease: Malfunctioning heart valves can disrupt normal blood flow and put extra stress on the atria.
- Heart Failure: A weakened heart muscle may struggle to pump blood effectively, leading to enlargement of the atria and increased susceptibility to AFib.
- Thyroid Problems: An overactive thyroid gland (hyperthyroidism) can accelerate heart rate and trigger AFib.
- Obesity: Excess body weight can contribute to several risk factors for AFib, including sleep apnea, hypertension, and diabetes.
- Diabetes: High blood sugar levels can damage blood vessels and nerves, including those in the heart.
- Sleep Apnea: This condition, characterized by pauses in breathing during sleep, is strongly linked to AFib.
- Alcohol Consumption: Excessive alcohol intake, particularly binge drinking, can acutely trigger AFib (“holiday heart syndrome”) and may contribute to chronic AFib over time.
- Genetics: In some individuals, there may be a genetic predisposition to developing AFib.
- Aging: The risk of AFib increases significantly with age, with a higher prevalence in older adults.
The irregular pumping of the atria in AFib means that blood can pool and stagnate, especially in the left atrial appendage, a small pouch within the left atrium. This pooling increases the likelihood of blood clot formation. If a clot breaks off, it can travel through the bloodstream and lodge in an artery supplying the brain, causing an ischemic stroke. This heightened risk of stroke is one of the most serious complications of AFib and a primary driver for its treatment.
The Principle of Cardiac Ablation for AFib
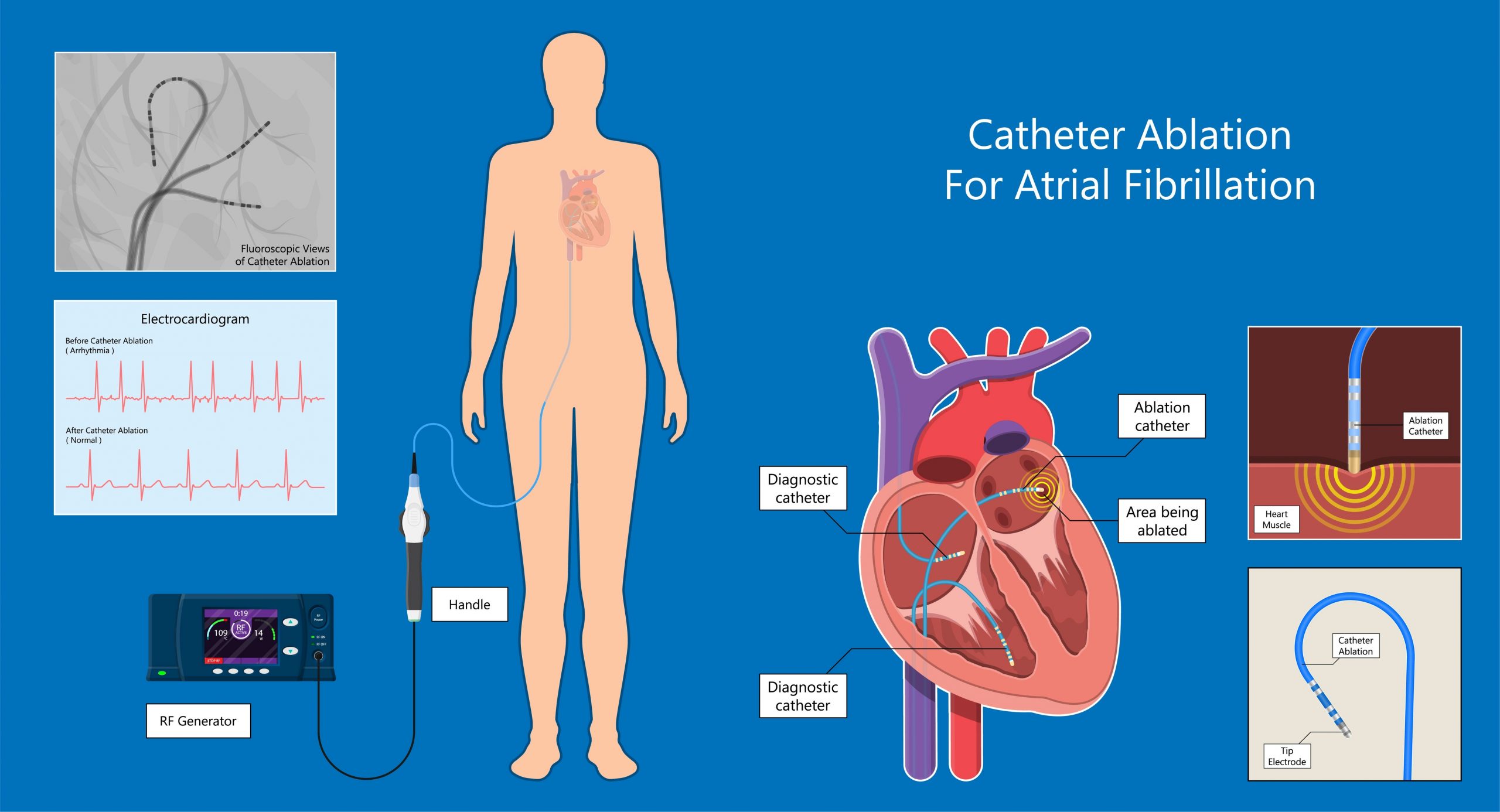
Cardiac ablation, specifically catheter ablation for AFib, is a procedure designed to eliminate the abnormal electrical pathways or sources that trigger and sustain the chaotic heart rhythms of AFib. The fundamental principle behind ablation is to intentionally create small scars in specific areas of the heart tissue. These scars are electrically inert, meaning they cannot conduct electrical impulses. By strategically placing these scars, the cardiologist can block the errant electrical signals that cause AFib, thereby restoring a normal heart rhythm.
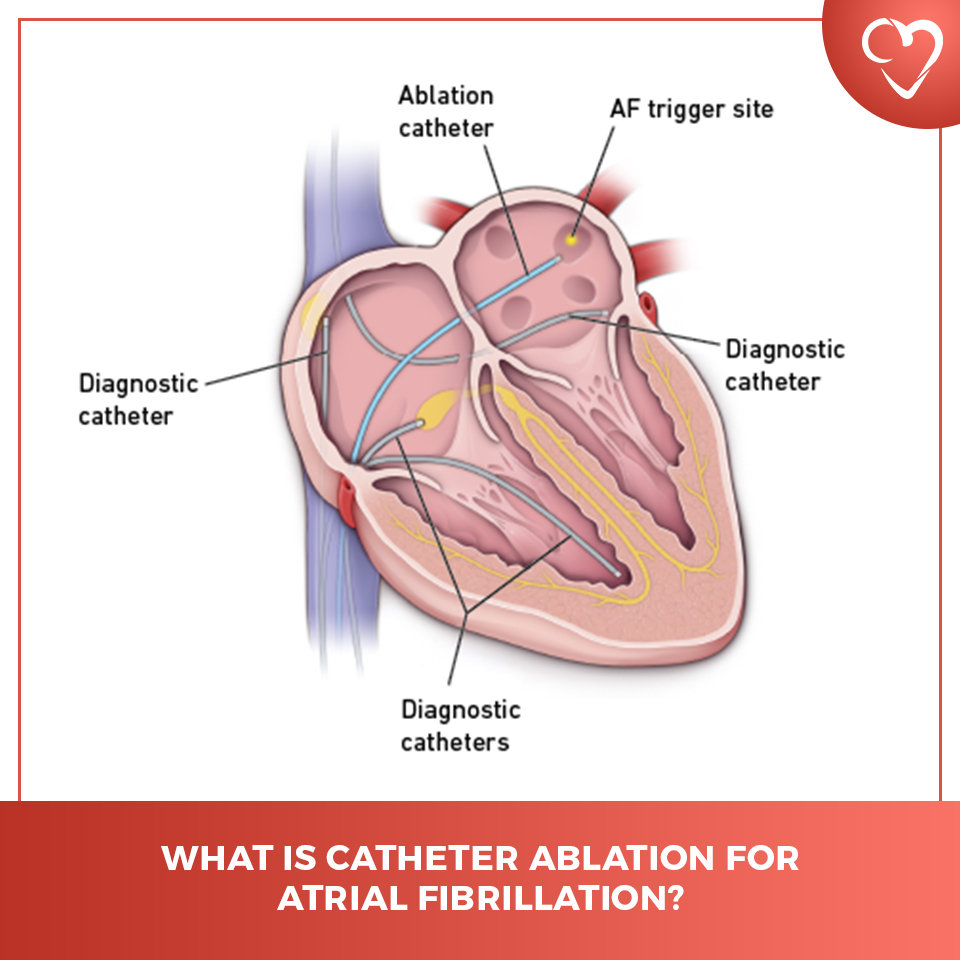
The most common culprits for AFib originate in the pulmonary veins, which are blood vessels that carry oxygenated blood from the lungs to the left atrium. In many individuals with AFib, the abnormal electrical impulses that initiate the arrhythmia arise from the muscle sleeves of the pulmonary veins where they connect to the left atrium. Therefore, a primary goal of AFib ablation is to isolate these pulmonary veins electrically from the rest of the atrium.
The procedure typically involves the use of radiofrequency energy or cryotherapy (extreme cold) delivered through a specialized catheter.
- Radiofrequency Ablation (RFA): This is the most common method. A catheter tipped with an electrode is guided through a vein (usually in the groin) to the heart. Once in position, the electrode at the tip of the catheter emits radiofrequency energy, which heats and destroys the targeted heart tissue, creating a small scar. This process is repeated at multiple points around the pulmonary veins to create a complete electrical block.
- Cryoablation: In this technique, the catheter tip is cooled to extremely low temperatures. This super-chilled tip freezes and destroys the abnormal heart tissue. Like RFA, multiple freeze-thaw cycles are performed to create scar tissue.
The choice between RFA and cryoablation often depends on the physician’s preference, the patient’s specific anatomy, and the characteristics of the AFib. Both methods have demonstrated high success rates in restoring normal sinus rhythm.
The Ablation Procedure: Step-by-Step
The AFib ablation procedure is performed in a cardiac catheterization laboratory (cath lab) by an electrophysiologist, a cardiologist who specializes in heart rhythm disorders. The process is generally as follows:
Pre-Procedure Preparation
Before the ablation, patients undergo a thorough evaluation, which may include:
- Medical History and Physical Examination: To assess overall health and identify any potential risks.
- Electrocardiogram (ECG/EKG): To record the heart’s electrical activity.
- Echocardiogram: An ultrasound of the heart to visualize its structure and function, including the size of the atria and the condition of the heart valves.
- Holter Monitor or Event Monitor: To capture heart rhythms over an extended period, helping to confirm the diagnosis and understand the pattern of AFib.
- Blood Tests: To check for anemia, thyroid function, and kidney function.
- Blood Thinners: Patients are typically advised to continue or adjust their anticoagulant medications as directed by their doctor, as this is crucial for preventing stroke during and after the procedure.
On the day of the procedure, patients are usually asked to fast for several hours beforehand. They will receive mild sedation to help them relax.
The Procedure Itself
- Access and Catheter Insertion: The procedure begins with numbing the skin at the insertion site, typically in the groin. A small puncture is made in a vein, and a thin, flexible tube called a sheath is inserted. Through this sheath, one or more specialized catheters are guided into the heart. These catheters are equipped with electrodes at their tips, which allow the electrophysiologist to map the heart’s electrical activity and deliver energy.
- Diagnostic Mapping: Before ablation, the electrophysiologist uses the catheters to create a detailed electrical map of the heart. This involves recording the electrical signals from different parts of the atria and pulmonary veins. This mapping helps identify the precise locations of the triggers for AFib and assesses the electrical conduction pathways. Sometimes, a medication is administered to try and provoke AFib if it’s not currently occurring, allowing for better mapping.
- Ablation Delivery: Once the target areas (often the ostia of the pulmonary veins) are identified, the ablation energy is delivered. For RFA, the catheter tip is positioned to deliver controlled heat. For cryoablation, the catheter tip is cooled. The electrophysiologist monitors the heart’s electrical response in real-time to ensure that the abnormal electrical signals are blocked. This process is repeated at multiple sites to create a complete circumferential line of block around the pulmonary veins. In some cases, ablation may also target other areas of the atria if they are contributing to the AFib.
- Testing and Confirmation: After the ablation is complete, the electrophysiologist will re-map the heart to confirm that the pulmonary veins are electrically isolated and that the abnormal signals have been eliminated. They will also try to induce AFib again to ensure the procedure was successful.
- Catheter Removal: Once the procedure is finished, the catheters are carefully removed, and the sheath is withdrawn. Pressure is applied to the puncture site to stop any bleeding, and a sterile dressing is applied.
Post-Procedure Recovery
After the ablation, patients are typically monitored in a recovery area for several hours. They are usually able to resume normal activities within a day or two, although strenuous exercise may be restricted for a week or two. Mild soreness at the insertion site is common. Patients will likely remain on blood thinners for a period after the procedure, as it takes time for the ablated tissue to heal and for the risk of clot formation to decrease. Follow-up appointments with the electrophysiologist are essential to monitor the heart rhythm and assess the long-term success of the ablation.
Benefits, Risks, and Success Rates of AFib Ablation
Cardiac ablation has emerged as a highly effective treatment for AFib, offering significant benefits for many patients.
Benefits of Ablation
- Restoration of Normal Heart Rhythm: The primary goal and benefit of ablation is to restore and maintain a normal sinus rhythm, which can alleviate symptoms and improve quality of life.
- Reduced Symptoms: Patients often experience a significant reduction or complete elimination of AFib symptoms such as palpitations, fatigue, shortness of breath, and dizziness.
- Reduced Stroke Risk: By eliminating AFib, the risk of stroke associated with the condition is substantially decreased. In many cases, patients who were previously on long-term anticoagulation may be able to discontinue or reduce their blood-thinning medication after a successful ablation, although this decision is always made on an individual basis and with careful consideration of residual risk factors.
- Improved Quality of Life: With fewer symptoms and a reduced risk of serious complications, patients often report a marked improvement in their overall well-being and ability to engage in daily activities.
- Alternative to Long-Term Medication: For patients who experience side effects from antiarrhythmic drugs or for whom medications are ineffective, ablation offers a durable alternative.
Risks Associated with Ablation
While cardiac ablation is considered a safe procedure, like any invasive intervention, it carries some risks. These are generally low, and the electrophysiologist will discuss them in detail with the patient. Potential risks include:
- Bleeding or Bruising: At the catheter insertion site.
- Infection: At the insertion site or within the heart.
- Blood Clots: Formation of clots in the legs (deep vein thrombosis) or lungs (pulmonary embolism).
- Cardiac Tamponade: A rare but serious complication where fluid accumulates around the heart, impairing its ability to pump.
- Damage to the Esophagus: The esophagus runs very close to the back of the left atrium, and in rare cases, heat from the ablation can cause injury.
- Pulmonary Vein Stenosis: Narrowing of the pulmonary veins, which can occur over time, though it is uncommon.
- Phrenic Nerve Injury: The phrenic nerve, which controls the diaphragm, runs near the pulmonary veins. Injury can lead to temporary or permanent diaphragm weakness.
- Stroke or Transient Ischemic Attack (TIA): Although ablation aims to reduce stroke risk, there is a small risk of stroke during or shortly after the procedure.
- Heart Block: Damage to the heart’s natural electrical system, requiring a pacemaker.
- Recurrence of AFib: Despite successful ablation, AFib can sometimes return, especially over time.
Success Rates
The success rates for AFib ablation vary depending on several factors, including the type of AFib (paroxysmal, persistent, or long-standing persistent), the patient’s overall health, the experience of the electrophysiologist and the center, and the specific ablation technique used.
For paroxysmal AFib (AFib that comes and goes), a single ablation procedure can be successful in restoring normal sinus rhythm in 70-80% of patients. For persistent AFib (AFib that is continuous), success rates may be slightly lower, and repeat procedures might be necessary. It’s important to understand that “success” is often defined as being free from AFib symptoms and documented AFib episodes on long-term monitoring. Even if AFib recurs, it may be less frequent or less severe than before the ablation, and symptoms may still be significantly improved.
Ablation is a powerful tool in the management of AFib, offering a pathway to symptom relief and a reduced risk of stroke for many individuals struggling with this common heart rhythm disorder. The decision to pursue ablation should be made in consultation with a qualified electrophysiologist, who can assess individual circumstances and guide patients toward the most appropriate treatment plan.