The acronym “ACS” is a cornerstone of emergency medicine, representing a critical condition that demands immediate recognition and intervention. While seemingly straightforward, a thorough understanding of ACS encompasses a spectrum of conditions, their underlying pathophysiology, diagnostic approaches, and management strategies. This article aims to provide a professional, insightful, and engaging overview of ACS, delving into its various facets to equip healthcare providers with essential knowledge.
Understanding Acute Coronary Syndromes (ACS)
Acute Coronary Syndromes (ACS) are a group of clinical conditions characterized by a sudden, reduced blood flow to the heart muscle. This blockage or severe narrowing of the coronary arteries, which supply oxygenated blood to the myocardium, leads to myocardial ischemia (lack of oxygen) and, if prolonged or severe enough, myocardial infarction (heart muscle death). ACS is a broad term, encompassing several related but distinct entities, all stemming from atherosclerotic plaque rupture or erosion within the coronary arteries.
The Spectrum of ACS: From Unstable Angina to Myocardial Infarction
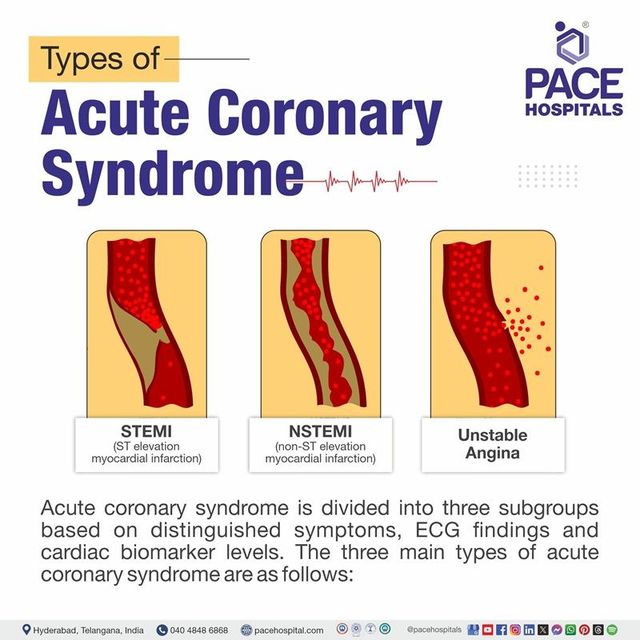
ACS is not a single diagnosis but rather a spectrum of conditions, differentiated by the degree of coronary artery blockage and the presence or absence of myocardial necrosis (heart muscle death). Understanding these distinctions is crucial for appropriate risk stratification and treatment selection.
Unstable Angina (UA)
Unstable angina represents the least severe end of the ACS spectrum. In UA, the coronary artery is significantly narrowed, but the blood flow is not completely occluded. Patients typically experience chest pain (angina) that is new in onset, occurs at rest, or is increasing in frequency, duration, or intensity. This signifies that the plaque within the artery has become unstable, leading to partial obstruction and intermittent ischemia. While there is no evidence of myocardial necrosis in UA, it is a critical warning sign of impending myocardial infarction and requires prompt evaluation and management to prevent further progression.
Non-ST-Segment Elevation Myocardial Infarction (NSTEMI)
NSTEMI is a more severe form of ACS where there is evidence of myocardial necrosis, but the electrocardiogram (ECG) does not show ST-segment elevation. This indicates a partial occlusion of a coronary artery. The damage to the heart muscle in NSTEMI can range from small to significant, depending on the duration and severity of the blood flow reduction. Biomarkers of myocardial injury, such as troponin, will be elevated in the blood, confirming the presence of heart muscle damage.
ST-Segment Elevation Myocardial Infarction (STEMI)
STEMI is the most severe and life-threatening form of ACS. It is characterized by a complete or near-complete occlusion of a coronary artery, leading to transmural (full-thickness) myocardial infarction. The ECG in STEMI classically shows ST-segment elevation in the leads corresponding to the affected area of the heart. This significant blockage results in substantial myocardial damage and loss of heart muscle function if not treated reperfusion (restoration of blood flow) rapidly. STEMI is a medical emergency that requires immediate reperfusion therapy, typically involving percutaneous coronary intervention (PCI) or fibrinolytic therapy.
Pathophysiology: The Underlying Cause of ACS
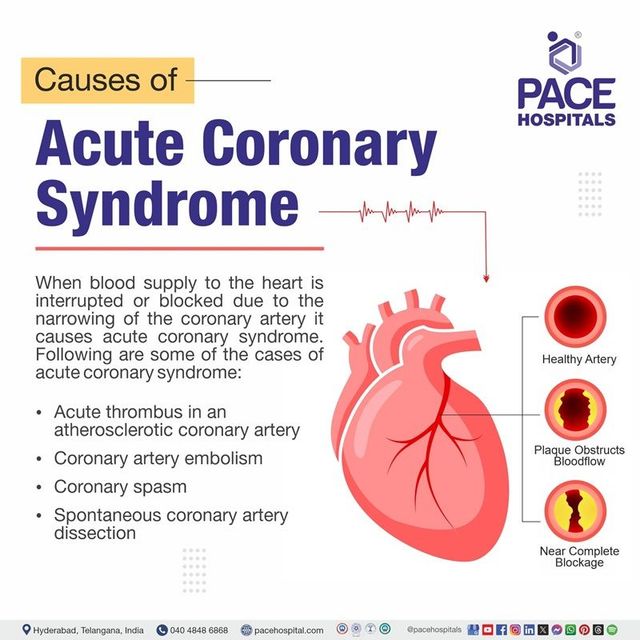
The genesis of ACS lies primarily in the process of atherosclerosis, a chronic inflammatory disease characterized by the buildup of fatty plaques within the inner lining of arteries.
Atherosclerotic Plaque Formation and Rupture
Atherosclerotic plaques begin as fatty streaks that progress to fibrous plaques containing cholesterol, inflammatory cells, and smooth muscle cells. These plaques can become unstable over time, developing a thin fibrous cap. The rupture or erosion of this cap exposes the thrombogenic core of the plaque to the bloodstream.
Thrombosis and Coronary Artery Occlusion
Upon exposure to the circulating blood, platelets adhere to the disrupted plaque, initiating the process of clot formation (thrombosis). This thrombus can partially or completely occlude the coronary artery, leading to reduced blood flow and myocardial ischemia. The severity of the occlusion dictates the clinical presentation and the extent of myocardial damage.
Myocardial Ischemia and Infarction
When blood flow to a portion of the myocardium is insufficient to meet its metabolic demands, ischemia occurs. If this ischemia is prolonged or severe enough, it leads to irreversible damage and death of heart muscle cells – myocardial infarction. The location and size of the infarct significantly impact the heart’s pumping function and can lead to various complications.
Diagnosis of ACS: A Multi-faceted Approach
Diagnosing ACS involves a systematic approach that combines patient history, physical examination, electrocardiography, and cardiac biomarker assessment. Early and accurate diagnosis is paramount for initiating appropriate treatment and improving patient outcomes.
History and Physical Examination: The First Clues
A detailed patient history is crucial, focusing on the characteristics of chest pain, including its onset, location, radiation, quality, duration, aggravating and relieving factors. Associated symptoms such as shortness of breath, nausea, vomiting, diaphoresis (sweating), and palpitations should also be elicited. The physical examination may reveal signs of impaired cardiac function, such as a gallop rhythm, murmurs, or evidence of pulmonary congestion.
Electrocardiography (ECG): A Vital Diagnostic Tool
The electrocardiogram is a cornerstone in the diagnosis of ACS. It provides a real-time electrical representation of the heart’s activity and can reveal characteristic changes indicative of ischemia or infarction.
ST-Segment Elevation and Depression
ST-segment elevation is a hallmark of STEMI and suggests acute transmural ischemia. ST-segment depression, on the other hand, can indicate subendocardial ischemia and is often seen in UA and NSTEMI. Changes in the T-waves, such as inversion or peaking, can also be indicative of ischemia.
Q Waves and Left Bundle Branch Block
The development of Q waves on the ECG typically signifies a completed myocardial infarction, indicating irreversible myocardial damage. A new left bundle branch block (LBBB) in the context of ischemic symptoms is also considered a STEMI equivalent by many guidelines, prompting emergent reperfusion strategies.
Cardiac Biomarkers: Confirming Myocardial Injury
Cardiac biomarkers are blood tests that measure the presence of specific proteins released into the bloodstream when heart muscle cells are damaged. Elevated levels of these biomarkers confirm myocardial necrosis and are essential for differentiating between unstable angina and myocardial infarction.
Troponin: The Gold Standard
Cardiac troponin, particularly troponin I and troponin T, are the most sensitive and specific biomarkers for myocardial injury. They are released into the circulation within hours of myocardial damage and remain elevated for several days. Serial measurements of troponin are crucial for detecting incremental rises, which are indicative of acute myocardial infarction.
Creatine Kinase-Myocardial Band (CK-MB)
While less sensitive and specific than troponin, CK-MB was historically used as a cardiac biomarker. It is an enzyme released from damaged heart muscle cells. Its levels typically rise a few hours after an infarction and return to normal within a couple of days.
Management of ACS: A Time-Sensitive Intervention
The management of ACS is a time-sensitive endeavor aimed at restoring blood flow to the myocardium, relieving symptoms, preventing further myocardial damage, and reducing the risk of future cardiovascular events. Treatment strategies are tailored to the specific type of ACS, with STEMI requiring immediate reperfusion therapy.
Initial Stabilization and Medical Management
Regardless of the specific ACS subtype, initial management often involves a combination of medications to reduce myocardial oxygen demand, prevent further clot formation, and alleviate pain.
Antiplatelet Agents
Dual antiplatelet therapy (DAPT), typically involving aspirin and a P2Y12 inhibitor (e.g., clopidogrel, ticagrelor, or prasugrel), is a cornerstone of ACS management. These medications prevent platelets from aggregating and forming blood clots.
Anticoagulants
Anticoagulants, such as heparin or low-molecular-weight heparin, are administered to prevent the propagation of existing thrombi and the formation of new clots.
Beta-Blockers and Nitrates
Beta-blockers help reduce myocardial oxygen demand by decreasing heart rate and contractility. Nitrates, such as nitroglycerin, are potent vasodilators that can relieve chest pain by improving blood flow to the heart muscle.
Statins
High-intensity statin therapy is initiated early in the management of ACS to stabilize atherosclerotic plaques and reduce the risk of future cardiovascular events.
Reperfusion Therapy for STEMI: A Life-Saving Intervention
For STEMI, rapid restoration of blood flow to the occluded coronary artery is critical to minimize myocardial damage.
Percutaneous Coronary Intervention (PCI)
Primary PCI, also known as angioplasty with stenting, is the preferred reperfusion strategy for STEMI when it can be performed promptly by an experienced team. This procedure involves inserting a catheter into the blocked artery, inflating a balloon to open it, and typically placing a stent to keep it open.
Fibrinolytic Therapy
Fibrinolytic therapy, or “clot-busting” drugs, can be used if PCI is not readily available. These medications dissolve the thrombus that is blocking the coronary artery. However, fibrinolysis carries a higher risk of bleeding complications compared to PCI.
Risk Stratification and Long-Term Management
Following initial treatment, patients with ACS undergo risk stratification to assess their likelihood of experiencing future cardiovascular events. This informs long-term management strategies aimed at secondary prevention.
Risk Assessment Tools
Tools such as the TIMI score or GRACE score are used to estimate short-term and long-term mortality risk in ACS patients.
Lifestyle Modifications and Secondary Prevention
Long-term management emphasizes aggressive risk factor modification, including smoking cessation, a heart-healthy diet, regular exercise, weight management, and optimal medical therapy to control blood pressure, cholesterol, and diabetes. Cardiac rehabilitation plays a vital role in helping patients recover and adopt a healthier lifestyle.
In conclusion, Acute Coronary Syndrome is a complex and dynamic medical condition requiring a comprehensive understanding of its pathophysiology, diagnostic nuances, and multifaceted management strategies. By mastering the intricacies of ACS, healthcare professionals can significantly improve patient outcomes and contribute to the prevention of cardiovascular disease.