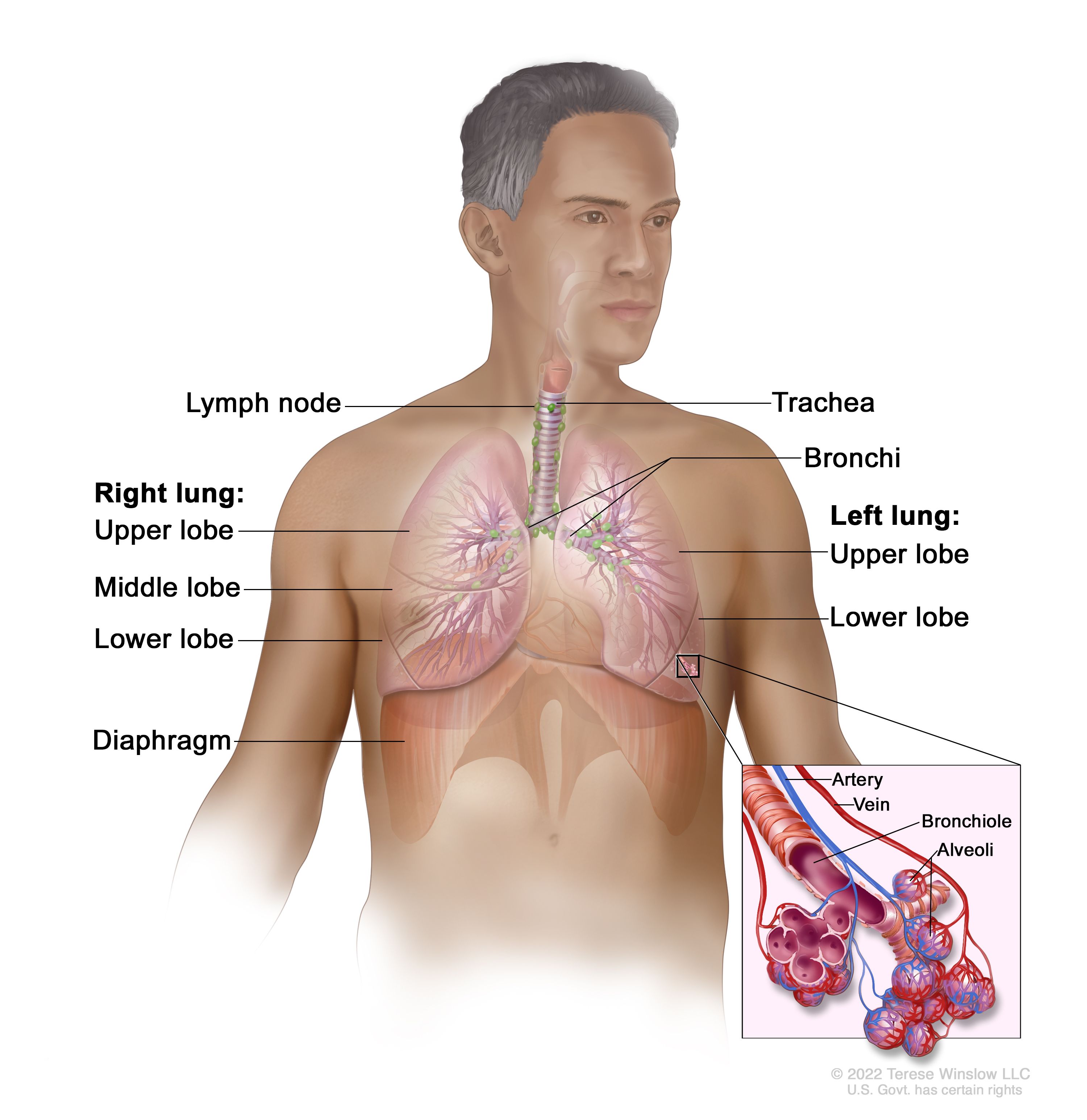
A windpipe, more accurately termed the trachea, is a vital component of the respiratory system in humans and many other animals. It serves as the primary conduit for air to travel from the larynx (voice box) to the lungs, playing a crucial role in breathing and vocalization. While seemingly a simple tube, the trachea is a marvel of biological engineering, designed for efficient airflow, protection from foreign particles, and structural integrity. Understanding its anatomy, function, and the challenges it faces provides valuable insight into the intricate workings of respiration and the broader field of biological engineering, which often inspires innovations in technology.
Anatomy of the Trachea: A Resilient Structure for Airflow
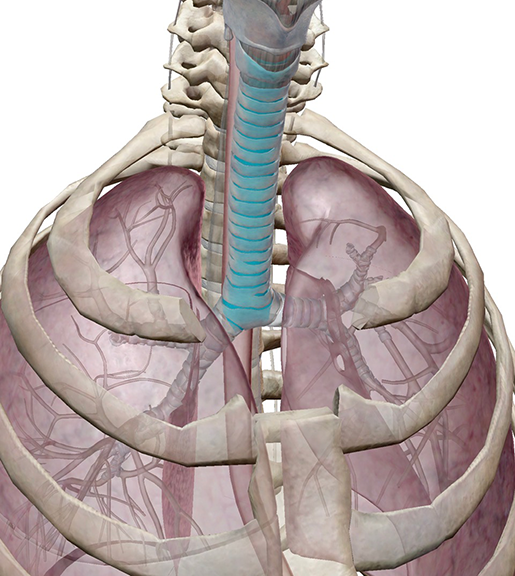
The trachea is a cartilaginous tube, typically measuring about 10-12 centimeters in length and 2-2.5 centimeters in diameter in adults. Its unique structure is essential for its demanding role in respiration.
Cartilaginous Rings: Providing Structural Support
The most distinctive feature of the trachea is its series of C-shaped rings of hyaline cartilage. There are typically 16 to 20 such rings, stacked one above the other. These cartilaginous rings are not complete circles; rather, they are open at the posterior (back) side. This C-shape is critical for the trachea’s function. The rigid cartilage provides continuous support, preventing the airway from collapsing, especially during inhalation when negative pressure is created within the thoracic cavity. Without this constant support, the trachea would likely collapse, impeding airflow and making breathing impossible. The open posterior portion of the C-ring is bridged by a band of smooth muscle called the trachealis muscle, and connective tissue. This arrangement allows for some degree of flexibility and slight changes in diameter.
Smooth Muscle and Connective Tissue: Dynamic Control and Flexibility
The trachealis muscle plays a significant role in regulating the diameter of the trachea. While its primary function isn’t to actively dilate or constrict the airway for breathing control (that role belongs more to the bronchioles), it can contract, subtly narrowing the tracheal lumen. This contraction is often triggered by irritants or during forceful expulsion of air, such as during coughing. The connective tissue surrounding the cartilaginous rings and connecting them to adjacent structures provides further flexibility and resilience. This allows the trachea to move and adjust as the neck extends and flexes, and also accommodates the slight expansion of the esophagus, which lies directly behind the trachea.
Mucous Membrane and Cilia: The Defense Mechanism
Lining the inner surface of the trachea is a specialized mucous membrane, also known as the respiratory epithelium. This membrane is pseudostratified columnar epithelium and is characterized by two key elements: goblet cells and ciliated cells.
Goblet Cells: Producing Mucus for Trapping
Goblet cells are specialized epithelial cells that secrete mucus. This mucus forms a sticky layer that covers the inner surface of the trachea. Its primary function is to trap inhaled particles such as dust, pollen, bacteria, viruses, and other debris. This trapping mechanism is a crucial first line of defense against respiratory infections and irritants. The sticky nature of the mucus effectively immobilizes these foreign substances, preventing them from reaching the delicate tissues of the lungs.
Ciliated Cells: The Escalator System
Interspersed among the goblet cells are ciliated cells, which possess thousands of tiny, hair-like projections called cilia on their apical surface. These cilia beat in a coordinated, wave-like motion, propelling the mucus and any trapped debris upward towards the pharynx. This continuous upward movement is often referred to as the mucociliary escalator. Once the mucus reaches the pharynx, it is either swallowed unconsciously or expectorated through coughing. This efficient cleaning mechanism is vital for maintaining a clear and healthy airway.
Functions of the Trachea: The Airway to Life
The trachea’s primary role is to facilitate the passage of air, but it also contributes to other essential respiratory functions.
Air Conduction: The Main Highway for Breath

The most fundamental function of the trachea is to serve as a conduit for air. It connects the larynx, where air enters the respiratory tract from the upper airway, to the bronchi, which then branch into the lungs. During inhalation, air is drawn from the atmosphere, through the nasal cavity or mouth, past the pharynx and larynx, and then down the trachea. During exhalation, the process is reversed, with air moving from the lungs, up the bronchi, through the trachea, and out of the body. The trachea’s wide, unobstructed lumen ensures that a sufficient volume of air can be exchanged with each breath, supporting the metabolic needs of the body. The cartilaginous rings are essential here, preventing any collapse that would hinder this vital airflow.
Protection from Inhaled Foreign Matter: The First Line of Defense
As discussed earlier, the mucous membrane and the mucociliary escalator are the trachea’s primary defense mechanisms against inhaled foreign matter. The sticky mucus traps particles, and the beating cilia move them upwards to be cleared. This protective function is critical in preventing infections and irritation of the lower respiratory tract. The cough reflex, often initiated by irritation within the trachea, is another protective mechanism that forcibly expels irritants and excess mucus.
Facilitating Coughing and Clearing the Airways: A Powerful Expulsion Mechanism
The trachea plays a crucial role in the powerful reflex of coughing. When the lining of the trachea is irritated, nerve signals are sent to the brain, triggering a deep inhalation, followed by a forceful closure of the glottis (the opening between the vocal cords). The muscles of the chest and abdomen then contract, building up pressure within the lungs. Finally, the glottis is suddenly opened, and the air is expelled rapidly, creating the characteristic sound of a cough. This forceful expulsion can clear mucus, foreign objects, or other irritants from the trachea and upper airways, thereby protecting the lungs. The flexibility of the trachealis muscle and the surrounding tissues allows for the significant changes in pressure and volume required for an effective cough.
Clinical Significance of the Trachea: When the Airway is Compromised
Disruptions to the normal structure or function of the trachea can have serious consequences for respiration. Various conditions can affect this vital airway.
Tracheal Obstruction: Threats to Airflow
Obstruction of the trachea is a medical emergency, as it can rapidly lead to suffocation. Obstructions can be caused by a variety of factors:
- Foreign Body Aspiration: This is particularly common in children, who may inhale small objects like toys, food particles, or coins. In adults, foreign bodies can be inhaled during eating or drinking, especially in individuals with impaired swallowing reflexes.
- Tumors: Both benign and malignant tumors can grow within the trachea, narrowing the airway.
- Inflammation and Swelling: Conditions like severe infections (e.g., epiglottitis, although it primarily affects the epiglottis, can lead to secondary tracheal inflammation) or allergic reactions can cause swelling of the tracheal lining, restricting airflow.
- Trauma: Blunt force trauma to the neck can damage the trachea, leading to bleeding, swelling, or even rupture. Penetrating injuries are also a significant risk.
- Stenosis: This refers to the narrowing of the trachea, which can occur after prolonged intubation (mechanical ventilation), radiation therapy, or as a result of chronic inflammatory conditions.
Tracheostomy and Intubation: Medical Interventions for Airway Management
When the natural airway is compromised, medical professionals may need to intervene to ensure adequate airflow.
Tracheostomy: Creating a Direct Airway
A tracheostomy is a surgical procedure that creates an opening in the anterior aspect of the neck and into the trachea, through which a breathing tube (tracheostomy tube) is inserted. This procedure bypasses the upper airway, providing a direct path for air to enter the lungs. Tracheostomies are performed for a variety of reasons, including:
- Long-term mechanical ventilation: When a patient requires prolonged support from a ventilator.
- Airway obstruction above the trachea: When the larynx or pharynx is blocked by a tumor, swelling, or trauma.
- Management of excessive secretions: For individuals who have difficulty clearing secretions from their airways.
- Facilitating weaning from mechanical ventilation.
Endotracheal Intubation: Temporary Airway Management
Endotracheal intubation involves inserting a tube through the mouth or nose, down the pharynx and larynx, and into the trachea. This is a temporary measure, typically used in emergency situations or for surgical procedures where the patient requires airway management and mechanical ventilation. While effective for short-term use, prolonged intubation can lead to tracheal damage, including stenosis, due to pressure from the tube and cuff.
The trachea is a testament to the elegance of biological design, a flexible yet resilient tube that safeguards our very breath. Its intricate structure, from the supportive cartilaginous rings to the self-cleaning mucociliary escalator, works tirelessly to ensure the unimpeded flow of life-giving air. Understanding this crucial airway highlights the fundamental importance of respiratory health and underscores the incredible adaptability of biological systems.