Pancreatic divisum is the most common congenital anomaly of the pancreas, meaning it is a condition present from birth due to a developmental issue in the embryonic stage. This anatomical variation arises from a failure of the dorsal and ventral pancreatic ducts to properly fuse during fetal development. While often asymptomatic, it can be associated with an increased risk of pancreatitis and other pancreatic disorders, making its understanding crucial for medical professionals and potentially impacting individuals diagnosed with it.
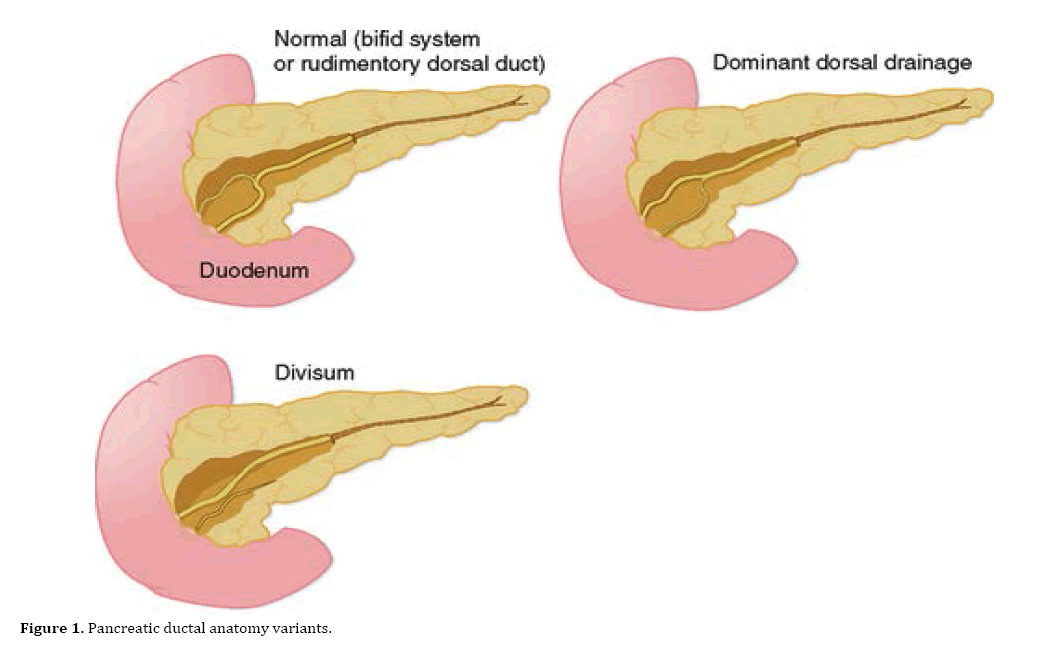
The pancreas is a vital organ located behind the stomach, responsible for producing digestive enzymes and hormones like insulin. Its dual embryonic origins, the ventral bud and the dorsal bud, contribute to the formation of its ductal system. Normally, these two buds fuse, and their respective ducts, the duct of Wirsung (ventral) and the duct of Santorini (dorsal), merge to form a single main pancreatic duct that empties into the duodenum. In pancreatic divisum, this fusion is incomplete.

Embryological Origins and Anatomical Variations
The development of the pancreas is a complex process that begins in the early weeks of gestation. Two distinct buds, the ventral and dorsal pancreatic anlagen, emerge from the primitive foregut. The ventral bud originates from the caudal part of the foregut, while the dorsal bud arises from the cranial part. These buds grow and differentiate, eventually forming the head, body, and tail of the pancreas.
The ductal system of the pancreas is intricately linked to these buds. The ventral bud typically forms the main pancreatic duct, known as the duct of Wirsung, which drains a portion of the head and the entire uncinated process. The dorsal bud forms the duct of Santorini, which drains the remaining parts of the head, body, and tail. A crucial event in normal pancreatic development is the fusion of these two ducts. The ventral duct usually joins the common bile duct and empties into the major duodenal papilla (ampulla of Vater). The dorsal duct then contributes to the duct of Wirsung, or it may persist as a separate duct that empties into the duodenum via the minor duodenal papilla.
In the case of pancreatic divisum, the fusion between the dorsal and ventral ducts fails. This failure results in the dorsal pancreas being drained primarily by the duct of Santorini, which typically empties into the minor duodenal papilla, and the ventral pancreas being drained by the duct of Wirsung, which empties into the major duodenal papilla. Consequently, the majority of pancreatic secretions from the dorsal bud must exit through the relatively smaller opening of the minor duodenal papilla.
There are three main types of pancreatic divisum described, based on the degree of ductal fusion and drainage:
Type 1: Complete Pancreatic Divisum
This is the most common and classic form, where there is a complete failure of fusion between the dorsal and ventral ducts. The dorsal pancreas is drained solely by the duct of Santorini, which empties into the minor papilla, while the ventral pancreas is drained by the duct of Wirsung, emptying into the major papilla. This leads to a significant drainage obstruction at the minor papilla.
Type 2: Partial Pancreatic Divisum
In this less common variant, there is a partial failure of fusion. Some communication may exist between the dorsal and ventral ducts, but the drainage pattern is still abnormal, often with a dominant role for the duct of Santorini.
Type 3: Incomplete Pancreatic Divisum
This is the rarest form, characterized by minimal or no fusion failure, but with some residual ductal anomalies.
The anatomical consequence of pancreatic divisum is that the bulk of pancreatic juice, rich in digestive enzymes, is forced to drain through the narrow minor duodenal papilla. This can lead to increased pressure within the duct of Santorini, potentially causing stasis of pancreatic secretions, obstruction, and ultimately, inflammation of the pancreas.
Clinical Manifestations and Associated Conditions
While pancreatic divisum is a congenital anomaly, it doesn’t always manifest with symptoms. Many individuals with this condition live their entire lives without any pancreatic issues. However, in a significant subset of patients, it can be a predisposing factor for several pancreatic disorders. The primary concern associated with pancreatic divisum is its link to recurrent acute pancreatitis.
Recurrent Acute Pancreatitis
This is the most frequently observed clinical manifestation in individuals with symptomatic pancreatic divisum. The theory is that the stenotic minor papilla acts as a bottleneck, impeding the free flow of pancreatic juice from the dorsal pancreas. This obstruction can lead to increased intraductal pressure, reflux of duodenal contents into the pancreatic ducts, and activation of digestive enzymes within the pancreas itself. This enzymatic autodigestion causes inflammation and damage, leading to acute pancreatitis. Symptoms of acute pancreatitis typically include severe upper abdominal pain that may radiate to the back, nausea, vomiting, fever, and abdominal tenderness. Episodes can range from mild to life-threatening.
Chronic Pancreatitis
In some individuals, recurrent episodes of acute pancreatitis can eventually lead to chronic pancreatitis. This is characterized by persistent inflammation, irreversible damage to pancreatic tissue, and impaired exocrine and endocrine function. Chronic pancreatitis can cause ongoing abdominal pain, malabsorption of nutrients (leading to steatorrhea and weight loss), and diabetes mellitus due to damage to insulin-producing cells.

Pancreatic Cancer
The relationship between pancreatic divisum and pancreatic cancer is a subject of ongoing research and debate. Some studies suggest a potentially higher risk of developing pancreatic ductal adenocarcinoma in individuals with pancreatic divisum, particularly those who also experience recurrent pancreatitis. The chronic inflammation and ductal stasis associated with pancreatic divisum might create a more favorable environment for neoplastic transformation. However, this association is not definitively established, and pancreatic divisum is not considered a direct precursor to cancer in the same way as certain genetic mutations.
Other Pancreatic Disorders
Less commonly, pancreatic divisum has been implicated in other pancreatic issues, such as pancreatic pseudocysts (fluid-filled sacs that can form in or around the pancreas), intraductal papillary mucinous neoplasms (IPMNs, a type of cystic tumor that can have malignant potential), and anomalous pancreaticobiliary union (APBU), where the pancreatic and common bile ducts join outside the duodenal wall.
It is important to note that the presence of pancreatic divisum alone does not guarantee the development of these conditions. Many factors, including genetic predisposition, lifestyle choices (such as alcohol consumption and diet), and environmental influences, play a role in the pathogenesis of pancreatic diseases.
Diagnosis and Management
Diagnosing pancreatic divisum and its associated complications requires a combination of imaging techniques and sometimes direct visualization. The management strategies are tailored to the individual’s symptoms and the underlying pancreatic issues.
Diagnostic Modalities
Historically, endoscopic retrograde cholangiopancreatography (ERCP) was the gold standard for diagnosing pancreatic divisum. ERCP involves inserting an endoscope into the duodenum and cannulating the pancreatic duct to inject contrast dye, which is then visualized using X-rays. This allows for detailed mapping of the pancreatic ductal anatomy. However, ERCP is an invasive procedure with associated risks.
More recently, non-invasive imaging techniques have become increasingly important:
- Magnetic Resonance Cholangiopancreatography (MRCP): This MRI-based technique provides excellent visualization of the pancreatic and biliary ducts without the need for contrast injection or radiation. MRCP is highly effective in identifying ductal anomalies like pancreatic divisum and can also detect signs of inflammation or obstruction.
- Computed Tomography (CT) Scan: While less sensitive than MRCP for visualizing fine ductal details, CT scans can provide valuable information about the pancreas, including its size, texture, and the presence of any associated inflammatory changes or complications. Contrast-enhanced CT is particularly useful.
- Endoscopic Ultrasound (EUS): EUS combines endoscopy with ultrasound, offering high-resolution imaging of the pancreas and its ducts. It can detect subtle ductal abnormalities and is useful for assessing the extent of inflammation or for guiding biopsies.
- Intraductal Ultrasound (IDUS): This technique involves introducing a miniature ultrasound probe through an endoscope directly into the pancreatic duct. It provides the highest resolution imaging of the ductal wall and lumen and can be very helpful in assessing the degree of stenosis at the minor papilla.
In cases where non-invasive imaging is inconclusive or when further assessment of ductal pressure is needed, ERCP may still be considered. During ERCP, cannulation of the minor papilla can be attempted. If contrast injection fills the duct of Santorini but not the duct of Wirsung, or if there is significant resistance to flow, it supports the diagnosis of pancreatic divisum. Manometric studies can also be performed during ERCP to assess pressure gradients across the papilla.
Management Strategies
The management of pancreatic divisum depends on whether the individual is symptomatic or asymptomatic.
Asymptomatic Pancreatic Divisum
For individuals diagnosed with pancreatic divisum who have no symptoms and no history of pancreatitis, no specific treatment is usually required. Regular monitoring may be recommended, especially if there are other risk factors for pancreatic disease.
Symptomatic Pancreatic Divisum
For symptomatic individuals, particularly those with recurrent acute pancreatitis, the goals of management are to relieve ductal obstruction, reduce intraductal pressure, and prevent further episodes of inflammation. Treatment options include:
-
Endoscopic Therapy:
- Minor Papillary Sphincterotomy (MPS): This is the most common endoscopic treatment. It involves cutting a small portion of the sphincter muscle at the minor duodenal papilla using a specialized knife during ERCP. This widens the opening, facilitating better drainage of pancreatic juice and reducing pressure in the duct of Santorini. MPS is often effective in reducing the frequency and severity of pancreatitis episodes.
- Ductal Stenting: In some cases, a small plastic or self-expanding metal stent may be placed across the minor papilla to keep it open and further improve drainage.
-
Surgical Intervention:
- Puestow Procedure (Partenope procedure): This is a surgical drainage procedure where a portion of the pancreatic duct of Santorini is surgically connected to the jejunum (a part of the small intestine). This bypasses the stenotic minor papilla and allows for free drainage of pancreatic secretions. This procedure is typically reserved for patients who fail endoscopic therapy or have severe ductal changes.
- Ventral Pancreatic Resection (e.g., Whipple procedure): In rare cases, when the ventral pancreas is significantly involved or if other pathologies are present, a partial pancreatectomy might be considered, but this is a major surgery with significant implications.
-
Medical Management: Regardless of the intervention, supportive medical management is crucial during episodes of pancreatitis. This includes intravenous fluid resuscitation, pain control, nutritional support (often nasogastric or parenteral feeding), and management of any complications. Lifestyle modifications, such as avoiding alcohol and maintaining a healthy diet, are also important for overall pancreatic health.
The decision-making process for managing pancreatic divisum and its complications is multidisciplinary, often involving gastroenterologists, surgeons, and radiologists. Careful consideration of the individual’s clinical presentation, anatomical findings, and potential risks and benefits of each treatment modality is essential to achieve the best possible outcome. Understanding pancreatic divisum is key to accurate diagnosis and effective management of a spectrum of pancreatic disorders.