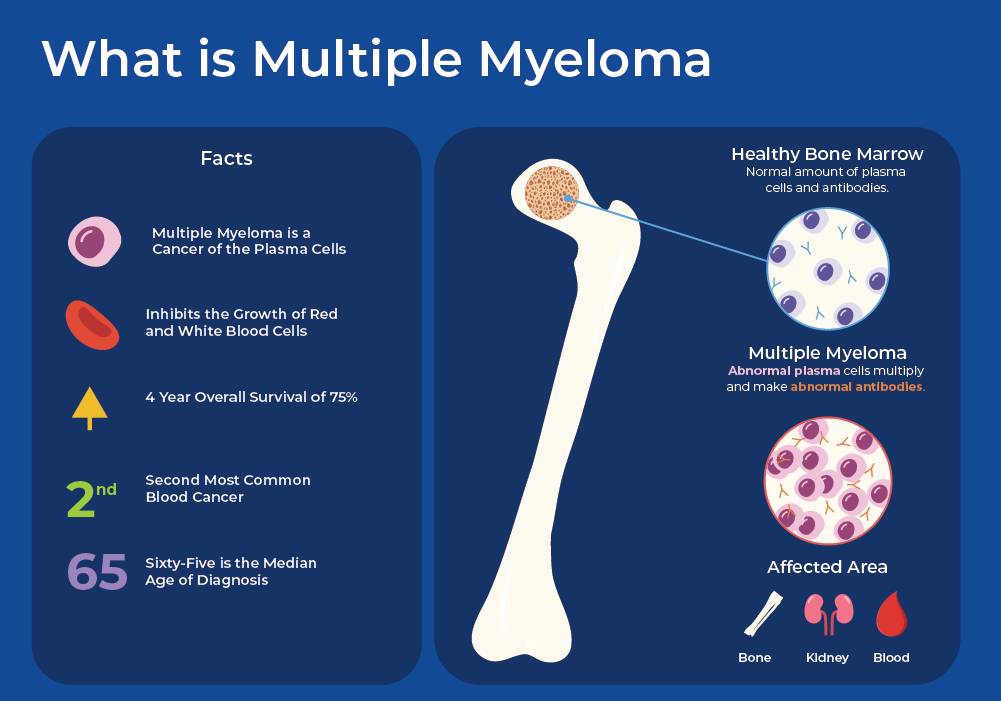
Myeloma, a term often encountered in discussions of blood cancers, refers to a specific type of malignancy that originates in the plasma cells. These plasma cells are a crucial component of the immune system, responsible for producing antibodies that help the body fight off infections. When these cells become cancerous, they proliferate uncontrollably, accumulating in the bone marrow and disrupting the production of normal blood cells. This disruption leads to a cascade of health issues that define the disease. Understanding myeloma requires delving into its cellular origins, its impact on the body, and the diagnostic and treatment approaches that have emerged.

The Cellular Roots of Myeloma
At its core, myeloma is a cancer of the plasma cells. To grasp the nature of this disease, it’s essential to first understand the normal function and lifecycle of these vital immune cells.
Plasma Cells: The Antibody Factories
Plasma cells, also known as plasma B cells or effector B cells, are differentiated B lymphocytes. B lymphocytes are a type of white blood cell that matures into plasma cells after encountering an antigen – a foreign substance that triggers an immune response. Upon activation, B cells undergo a remarkable transformation, developing into specialized plasma cells that are highly efficient antibody-producing factories. These antibodies, also called immunoglobulins, are Y-shaped proteins that bind to specific antigens, marking them for destruction by other immune cells or neutralizing them directly.
Normally, plasma cells reside primarily in the bone marrow, though small numbers can also be found in lymph nodes and the spleen. Their lifespan is relatively short, typically ranging from a few days to a few weeks, after which they undergo programmed cell death (apoptosis). This continuous turnover ensures that antibody production is dynamically regulated according to the body’s needs.
The Aberrant Transformation: From Healthy Cell to Cancerous Clone
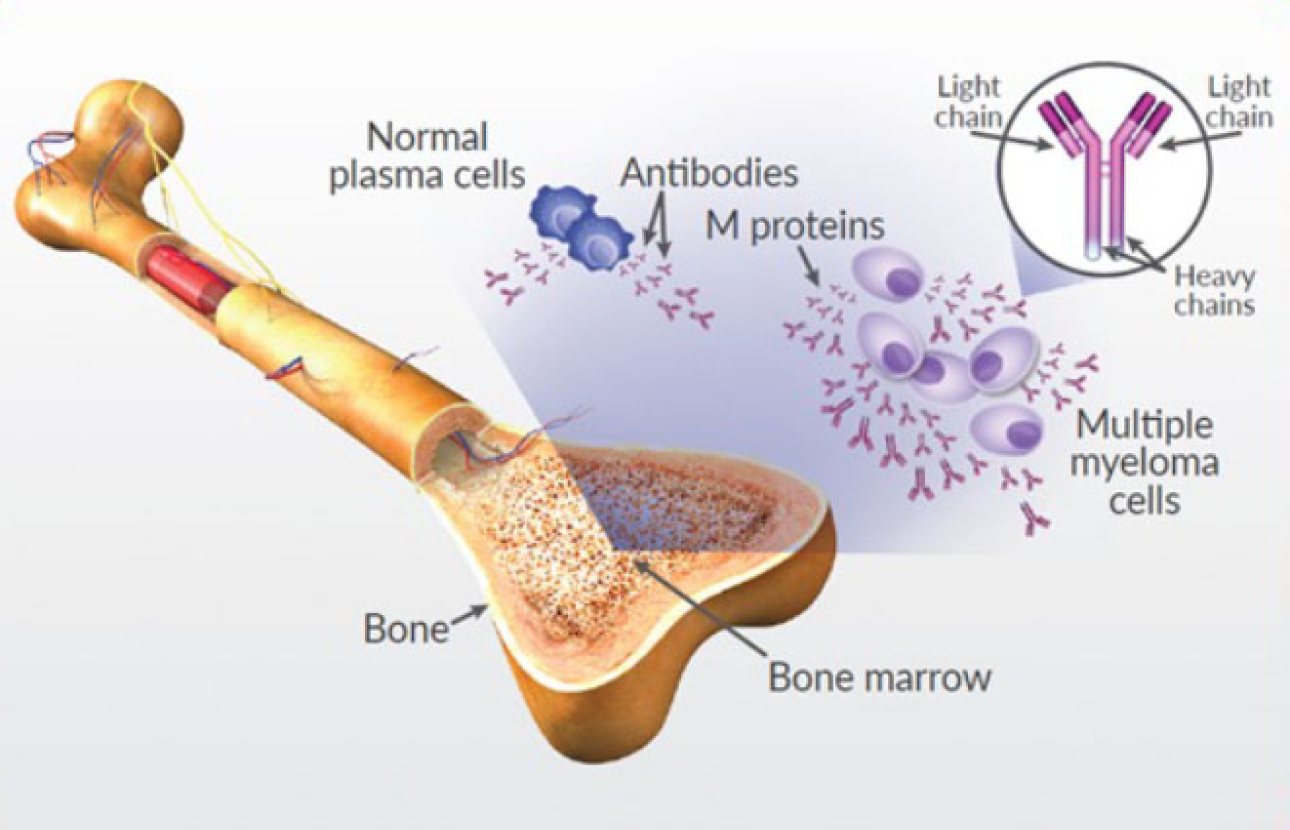
In myeloma, a single plasma cell undergoes genetic mutations, leading to its transformation into a cancerous cell. This mutated cell then begins to divide and multiply uncontrollably, forming a clone of abnormal plasma cells. Unlike their healthy counterparts, these myeloma cells are often immortal, continuing to proliferate indefinitely. Furthermore, they lose their ability to produce functional antibodies. Instead, many myeloma cells produce a specific type of abnormal antibody called a monoclonal immunoglobulin or M-protein. This M-protein is often detected in blood and urine tests and serves as a key diagnostic marker for myeloma.
The accumulation of these cancerous plasma cells in the bone marrow is the hallmark of the disease. This crowding out of normal hematopoietic stem cells disrupts the production of other essential blood components, including red blood cells, white blood cells (other than lymphocytes), and platelets. This can lead to a variety of symptoms and complications associated with myeloma.
The Impact of Myeloma on the Body
The uncontrolled proliferation of myeloma cells and their disruption of normal bone marrow function have widespread effects on various organ systems. The symptoms experienced by individuals with myeloma are directly related to these consequences.
Bone Marrow Dysfunction and Its Consequences
As myeloma cells infiltrate and proliferate within the bone marrow, they displace the healthy cells responsible for producing red blood cells, white blood cells, and platelets.
- Anemia: The reduced production of red blood cells leads to anemia, characterized by a deficiency in oxygen-carrying capacity. Symptoms of anemia include fatigue, weakness, shortness of breath, and paleness.
- Immunodeficiency: The impaired production of healthy white blood cells can weaken the immune system, making individuals with myeloma more susceptible to infections. These infections can be recurrent and severe, posing a significant threat.
- Thrombocytopenia: A low platelet count, known as thrombocytopenia, can lead to an increased risk of bleeding and bruising.
Bone Lesions and Skeletal Complications
One of the most characteristic and debilitating features of myeloma is its impact on the bones. The accumulating myeloma cells in the bone marrow can directly affect bone metabolism.
- Osteolytic Lesions: Myeloma cells stimulate osteoclasts, cells that break down bone tissue, while simultaneously suppressing osteoblasts, cells that build bone. This imbalance leads to the formation of lytic lesions, which are areas of bone destruction. These lesions are often described as “punched-out” areas on X-rays and are most commonly found in the spine, skull, pelvis, and ribs.
- Bone Pain: The destruction of bone tissue can cause significant pain, often described as a deep, aching sensation. This pain can be constant or intermittent and may worsen with movement.
- Fractures: Weakened bones are prone to fractures, even from minor trauma. Pathological fractures, occurring without significant injury, are a common complication of myeloma.
- Hypercalcemia: The breakdown of bone releases calcium into the bloodstream, leading to hypercalcemia, or elevated calcium levels. Symptoms of hypercalcemia can include nausea, vomiting, constipation, confusion, and kidney problems.
Kidney Dysfunction
The kidneys are particularly vulnerable to the effects of myeloma.
- Light Chain Deposition Disease: The abnormal M-proteins produced by myeloma cells can be filtered by the kidneys. In some cases, these proteins, particularly the smaller light chains, can accumulate in the kidney tubules, causing damage and impairing kidney function. This condition is known as light chain deposition disease.
- Amyloidosis: In certain types of myeloma, the M-protein can misfold and aggregate into amyloid fibrils, which can deposit in various organs, including the kidneys, heart, and nerves. This can lead to organ damage and dysfunction.
- Dehydration and Hypercalcemia: The aforementioned hypercalcemia can also contribute to kidney damage by affecting fluid balance and the ability of the kidneys to concentrate urine.
Diagnosis and Treatment of Myeloma
Diagnosing myeloma involves a comprehensive approach that utilizes a variety of tests to confirm the presence of cancerous plasma cells and assess the extent of the disease. Treatment strategies are tailored to the individual patient, considering factors such as the stage of the disease, the patient’s overall health, and the presence of specific genetic abnormalities.
Diagnostic Pathways
The diagnostic process for myeloma typically involves a combination of blood tests, urine tests, bone marrow biopsy, and imaging studies.
- Blood Tests:
- Complete Blood Count (CBC): Evaluates the levels of red blood cells, white blood cells, and platelets, which can reveal anemia, immunodeficiency, or low platelet counts.
- Serum Protein Electrophoresis (SPEP) and Immunofixation Electrophoresis (SIFE): These tests detect and quantify M-proteins in the blood.
- Serum Free Light Chain Assay: Measures the levels of kappa and lambda free light chains, which can also indicate myeloma.
- Kidney Function Tests: Assess the health of the kidneys.
- Calcium Levels: Measures blood calcium to detect hypercalcemia.
- Urine Tests:
- 24-Hour Urine Collection: Used for urine protein electrophoresis and immunofixation to detect Bence Jones proteins (monoclonal free light chains) in the urine.
- Bone Marrow Biopsy and Aspiration: A small sample of bone marrow is extracted, usually from the hip bone. This allows pathologists to examine the number and morphology of plasma cells and identify any genetic abnormalities within the cells.
- Imaging Studies:
- X-rays: Used to detect lytic bone lesions.
- CT Scans (Computed Tomography): Provide more detailed images of bone lesions and can help assess the extent of bone involvement.
- MRI Scans (Magnetic Resonance Imaging): Offer excellent visualization of bone marrow and soft tissues, useful for identifying lesions that may not be visible on X-rays.
- PET Scans (Positron Emission Tomography): Can help detect active areas of myeloma throughout the body.
Therapeutic Strategies
Treatment for myeloma has evolved significantly, offering various options to manage the disease and improve patient outcomes. The goal of treatment is to control the growth of myeloma cells, alleviate symptoms, and prevent complications.
- Chemotherapy: The use of drugs to kill cancer cells. Different types of chemotherapy agents are used, often in combination.
- Targeted Therapy: Medications that specifically target certain molecules or pathways involved in the growth of myeloma cells. Examples include proteasome inhibitors and immunomodulatory drugs.
- Immunotherapy: Therapies that harness the patient’s own immune system to fight cancer. This can include monoclonal antibodies that target myeloma cells.
- Stem Cell Transplantation:
- Autologous Stem Cell Transplantation (ASCT): The patient’s own stem cells are collected, treated to remove myeloma cells, and then infused back into the patient after high-dose chemotherapy.
- Allogeneic Stem Cell Transplantation: Stem cells from a donor are used. This is less common for myeloma but can be an option in certain cases.
- Supportive Care: Management of symptoms and complications, such as pain management, treatment of anemia and infections, and management of bone health.
The management of myeloma is often a multidisciplinary effort involving oncologists, hematologists, radiologists, and other specialists to provide comprehensive care for patients. Ongoing research continues to explore novel treatment strategies and improve our understanding of this complex blood cancer.