The term “lap cholecystectomy” is a shorthand, commonly used in medical settings, for a laparoscopic cholecystectomy. This surgical procedure represents a significant advancement in the treatment of gallbladder disease, offering a less invasive and often quicker recovery compared to traditional open surgery. Understanding what a lap cholecystectomy entails requires delving into the anatomy of the gallbladder, the conditions it affects, and the specific techniques employed during the surgery.
The gallbladder, a small, pear-shaped organ nestled beneath the liver, plays a crucial role in digestion. Its primary function is to store and concentrate bile, a fluid produced by the liver that aids in the breakdown of fats in the small intestine. However, this vital organ can be prone to various ailments, the most common of which are gallstones.
Understanding Gallbladder Disease
Gallstones, concretions that form within the gallbladder, are a prevalent issue affecting millions worldwide. These stones can range in size from a grain of sand to a golf ball and are primarily composed of cholesterol, bile pigments, or a combination of both. While many individuals with gallstones remain asymptomatic, others can experience significant discomfort and complications.
The Formation and Impact of Gallstones
The precise mechanisms leading to gallstone formation are complex and not fully understood. However, several factors are known to increase risk, including obesity, rapid weight loss, high cholesterol diets, certain medical conditions like diabetes and liver disease, and genetic predispositions. When gallstones are present, they can obstruct the normal flow of bile.
Common Symptoms and Complications
The presence of gallstones can manifest in a variety of ways. Biliary colic, characterized by sudden, intense pain in the upper right abdomen, often radiating to the back or shoulder, is a hallmark symptom. This pain typically occurs after meals, particularly those high in fat, as the gallbladder attempts to contract and expel bile. Nausea, vomiting, and bloating can also accompany these episodes.
Beyond discomfort, gallstones can lead to more serious complications. Cholecystitis, or inflammation of the gallbladder, can occur when a stone persistently blocks the cystic duct. This condition often presents with fever, persistent severe pain, and tenderness in the upper abdomen. Other potential complications include:
- Choledocholithiasis: Gallstones migrating into the common bile duct, potentially obstructing bile flow from both the gallbladder and the liver. This can lead to jaundice (yellowing of the skin and eyes), dark urine, and pale stools.
- Pancreatitis: Inflammation of the pancreas, which can occur if gallstones block the duct that drains the pancreas into the small intestine. This is a serious condition requiring immediate medical attention.
- Cholangitis: An infection of the bile ducts, which can be life-threatening and requires aggressive treatment.
When these symptoms or complications arise, surgical intervention to remove the gallbladder often becomes necessary.
The Laparoscopic Cholecystectomy Procedure
Laparoscopic cholecystectomy, often referred to as a “lap chole,” is the gold standard for surgical gallbladder removal. This minimally invasive technique utilizes specialized instruments and a video camera to perform the surgery through small incisions.
Pre-Operative Preparations and Anesthesia
Before undergoing a lap cholecystectomy, patients will undergo a thorough medical evaluation. This typically includes a review of their medical history, a physical examination, and potentially blood tests and imaging studies such as an ultrasound to confirm the presence and location of gallstones. Patients will also receive pre-operative instructions regarding diet, medications, and when to stop eating and drinking before surgery.
The procedure is performed under general anesthesia, meaning the patient will be asleep and pain-free throughout the surgery. An anesthesiologist will administer and monitor the anesthesia, ensuring the patient’s safety and comfort.
The Surgical Steps: A Minimally Invasive Approach
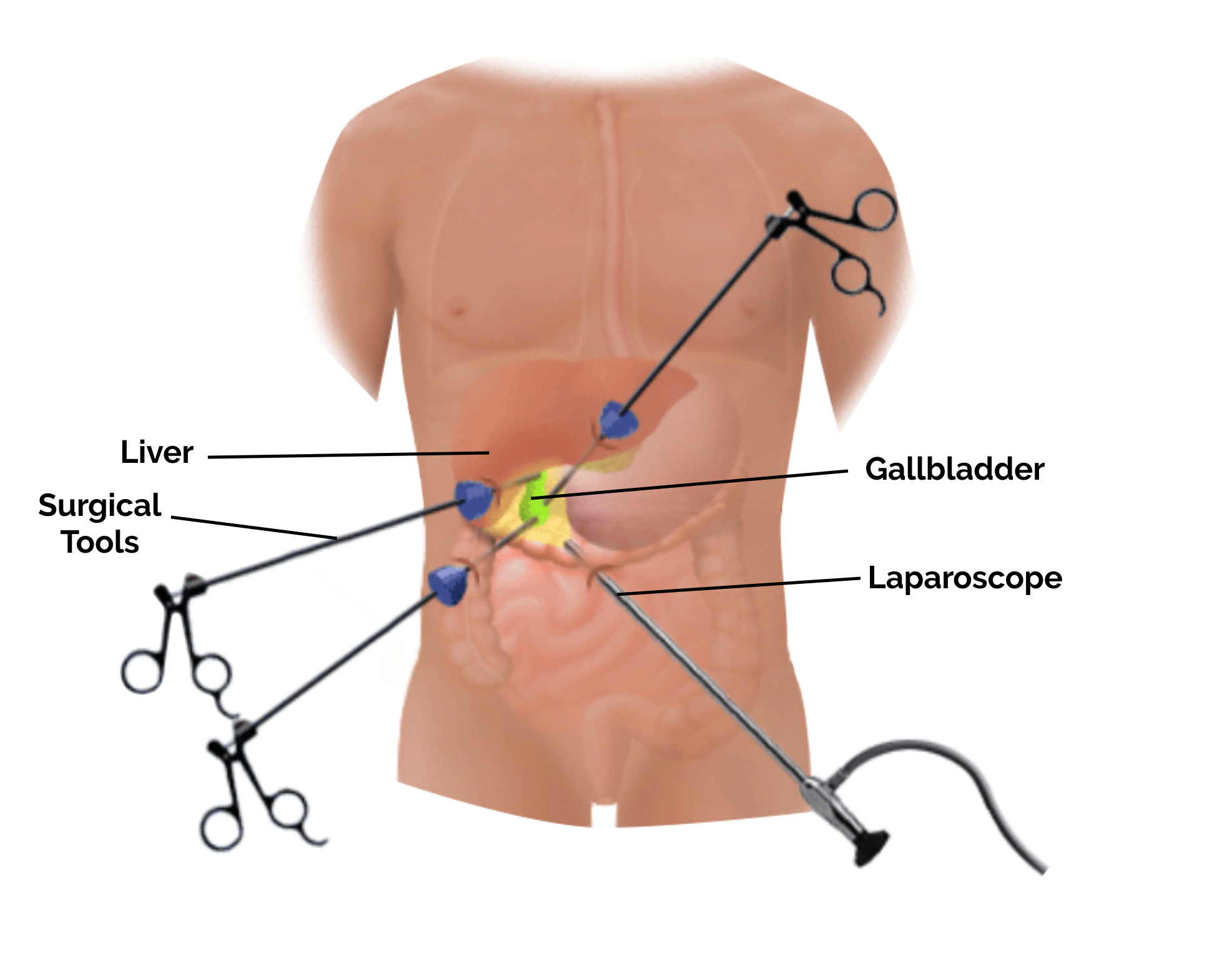
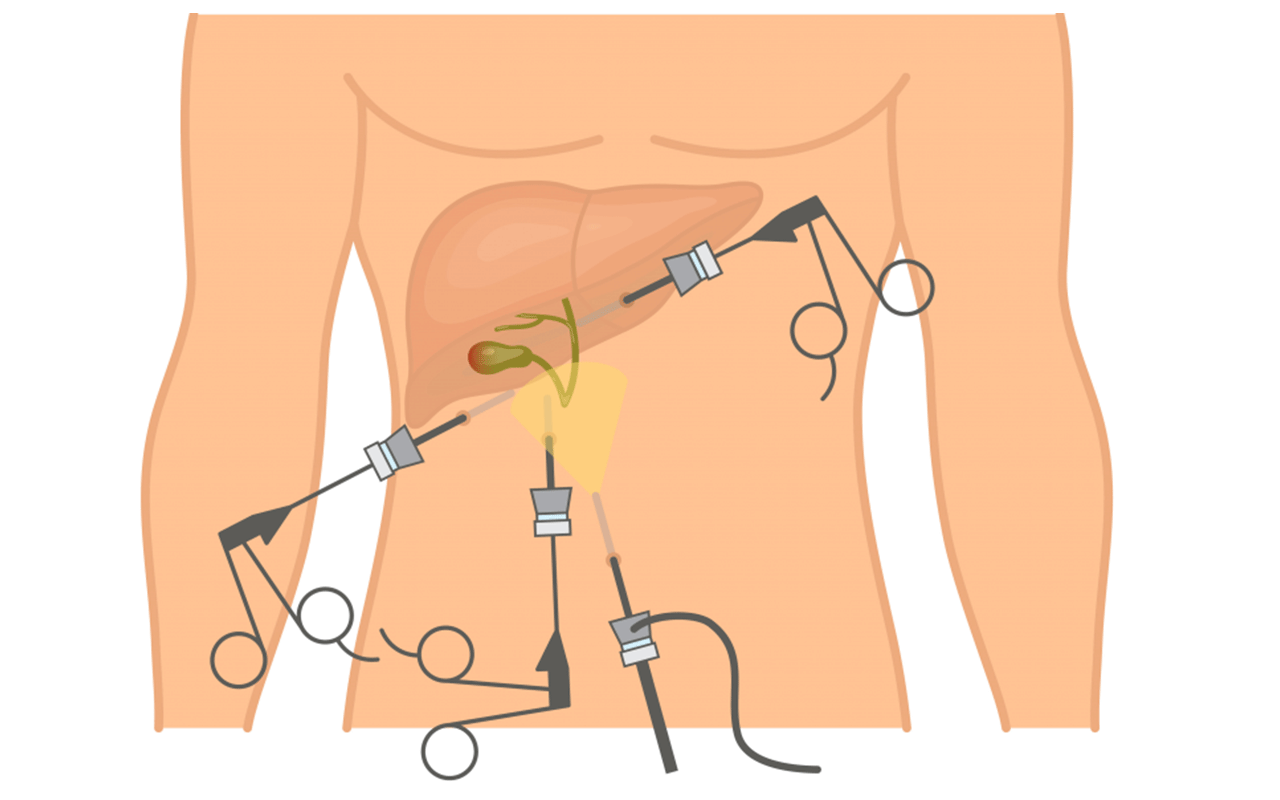
The core of the laparoscopic cholecystectomy lies in its minimal invasiveness. Instead of a large incision, the surgeon makes typically three to four small incisions, each about 0.5 to 1 centimeter in length, on the abdomen.
-
Establishing Pneumoperitoneum: The first step involves inflating the abdominal cavity with carbon dioxide gas. This creates space between the abdominal wall and the organs, providing the surgeon with a clear view and allowing for easier manipulation of instruments.
-
Inserting the Trocars: Through these small incisions, the surgeon inserts specialized surgical instruments called trocars. These are hollow tubes through which the laparoscopic instruments and the camera are passed.
-
Introducing the Laparoscope: One of the trocars is used to insert a laparoscope. This is a slender, lighted tube equipped with a high-definition camera. The camera transmits magnified images of the internal organs to a video monitor in the operating room, allowing the surgical team to visualize the gallbladder and surrounding structures in detail.

-
Instrument Manipulation: Through the other trocars, the surgeon inserts specialized laparoscopic instruments. These include graspers to hold tissues, scissors to cut, and dissectors to separate structures. The surgeon’s movements with these instruments are guided by the images on the monitor.
-
Dissecting the Gallbladder: The surgeon carefully identifies and dissects the cystic duct (the tube connecting the gallbladder to the common bile duct) and the cystic artery (the blood vessel supplying the gallbladder). These structures are then clipped or tied off to prevent bleeding and bile leakage.
-
Removing the Gallbladder: Once the gallbladder is fully detached, it is often placed into a small retrieval bag. This bag is then pulled out through one of the trocar incisions. In some cases, the gallbladder may be cut into smaller pieces before removal if it is too large to be extracted whole.
-
Closing the Incisions: After the gallbladder is removed and the surgical area is checked for any bleeding, the carbon dioxide gas is released from the abdomen. The small incisions are then closed with sutures, surgical tape, or sterile adhesive strips.
Advantages and Recovery
The laparoscopic approach to gallbladder removal offers numerous benefits over traditional open surgery, primarily centered on reduced invasiveness and a faster return to normal activities.
Benefits of Minimally Invasive Surgery
The advantages of a lap cholecystectomy are significant and contribute to a better patient experience:
- Reduced Pain: With smaller incisions and less trauma to the abdominal tissues, patients generally experience significantly less post-operative pain compared to open surgery.
- Shorter Hospital Stay: The majority of patients undergoing a lap cholecystectomy are able to go home the same day or the following day. Open surgery typically requires a longer hospital stay.
- Faster Recovery and Return to Activity: The less invasive nature of the procedure allows for a quicker recovery. Most individuals can resume light activities within a few days and return to their normal routines, including work and exercise, within one to two weeks.
- Minimal Scarring: The small incisions result in less noticeable scarring, which is often a cosmetic advantage for patients.
- Lower Risk of Infection: Smaller incisions generally carry a lower risk of surgical site infections.
- Reduced Risk of Hernia Formation: Compared to larger incisions, the smaller incisions in laparoscopic surgery are associated with a lower incidence of incisional hernias.
Post-Operative Care and Expectations
Following a lap cholecystectomy, patients will be monitored in a recovery area as they awaken from anesthesia. They will be given pain medication to manage any discomfort. It is common to feel some soreness around the incision sites and potentially some shoulder pain, which is typically referred pain from the carbon dioxide gas used during surgery.
Dietary recommendations post-surgery are usually gradual. Initially, patients may be advised to stick to a clear liquid diet and then progress to a bland diet. Many individuals can resume a normal diet within a few weeks, though some may find they need to adjust their intake of fatty foods.
While the gallbladder is removed, the body can adapt without it. Bile will flow directly from the liver into the small intestine, and most individuals do not experience long-term digestive issues. Some may experience temporary changes in bowel habits, such as looser stools, which often resolve over time.
When is Lap Cholecystectomy Recommended?
Laparoscopic cholecystectomy is the preferred surgical method for a wide range of gallbladder conditions, particularly those involving symptomatic gallstones.
Indications for Gallbladder Removal
The decision to recommend a lap cholecystectomy is typically based on the presence of symptomatic gallstones or other gallbladder abnormalities that pose a risk to health. Common indications include:
- Symptomatic Cholelithiasis (Gallstones): This is the most frequent reason for gallbladder removal. If gallstones are causing recurrent pain (biliary colic), the patient is likely to benefit from surgery.
- Acute Cholecystitis: Inflammation of the gallbladder, often caused by a gallstone obstructing the cystic duct.
- Gallstone Pancreatitis: When gallstones are the cause of pancreatic inflammation.
- Choledocholithiasis: Presence of gallstones in the common bile duct.
- Biliary Dyskinesia: A motility disorder of the gallbladder where it does not empty properly, causing pain despite the absence of stones.
- Gallbladder Polyps: Certain types of gallbladder polyps, especially if they are large or growing, may warrant removal due to the risk of malignancy.
- Acalculous Cholecystitis: Inflammation of the gallbladder without the presence of gallstones, which can occur in critically ill patients.
Contraindications and Alternative Approaches
While lap cholecystectomy is widely applicable, there are certain situations where it may not be the safest or most appropriate option. Relative contraindications can include:
- Severe Inflammation or Infection: In cases of extremely severe inflammation or infection of the gallbladder, an open approach might be chosen to provide better access and control.
- Advanced Liver Disease: Patients with severe cirrhosis or portal hypertension may have an increased risk of bleeding during laparoscopic surgery.
- Previous Abdominal Surgeries: Extensive adhesions from prior surgeries could make laparoscopic dissection challenging.
- Uncorrected Bleeding Disorders: Conditions that impair blood clotting can increase surgical risks.
- Inability to Tolerate General Anesthesia: If a patient cannot safely undergo general anesthesia, alternative options may be explored.
In instances where laparoscopic surgery is deemed too risky or not feasible, an open cholecystectomy would be performed. This involves a larger incision in the upper abdomen, providing the surgeon with direct visual and tactile access to the gallbladder. In rare cases, a procedure may begin laparoscopically and need to be converted to an open surgery if unforeseen complications arise.
In conclusion, the lap cholecystectomy represents a remarkable stride in surgical medicine, transforming the treatment of gallbladder disease from a major undertaking to a generally well-tolerated procedure with rapid recovery. Its widespread adoption is a testament to its efficacy and the significant improvement it offers in patient outcomes and quality of life.