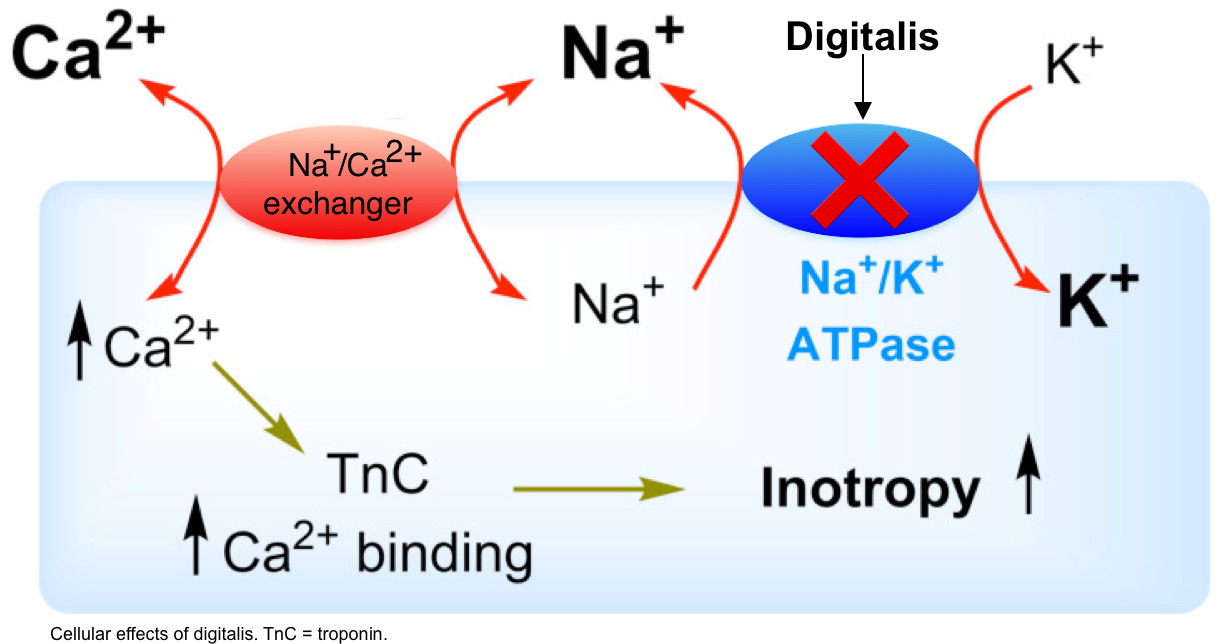
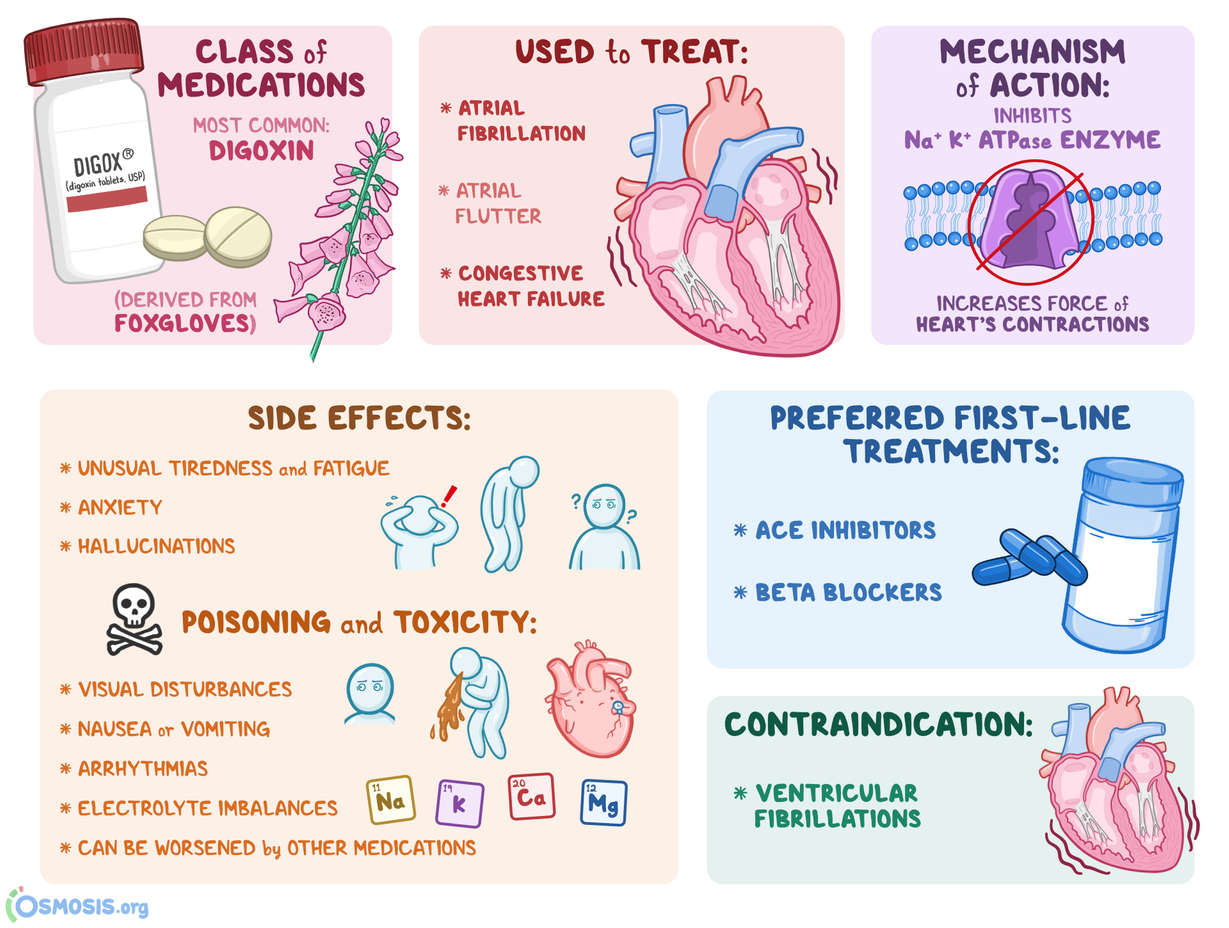
Digoxin, a cardiac glycoside derived from the Digitalis plant, has been a cornerstone in the management of certain cardiovascular conditions for decades. Its primary mechanism of action involves inhibiting the sodium-potassium ATPase pump (Na+/K+-ATPase) in myocardial cells. This inhibition leads to an increase in intracellular sodium, which in turn promotes calcium influx via the sodium-calcium exchanger, ultimately augmenting myocardial contractility. While effective in treating conditions such as heart failure and atrial fibrillation, digoxin’s therapeutic window is notoriously narrow, and its efficacy and safety are intimately linked to the patient’s electrolyte balance. Imbalances in certain electrolytes can significantly potentiate digoxin toxicity, making their careful monitoring and management paramount. Among the various electrolyte derangements, hypokalemia (low serum potassium) stands out as the most critical abnormality that digoxin can cause or, more accurately, exacerbate into a dangerous clinical scenario. Understanding this relationship is fundamental for healthcare professionals involved in prescribing and managing digoxin therapy.

The Critical Role of Potassium in Cardiac Function and Digoxin’s Mechanism
Potassium, a positively charged ion (cation), plays an indispensable role in maintaining the electrochemical gradient across cell membranes, particularly in excitable tissues like the heart and nerves. In cardiac cells, the resting membrane potential is largely determined by the outward movement of potassium ions through specific ion channels. This potential is crucial for the normal generation and propagation of electrical impulses that govern the heart’s rhythmic contractions.
The Na+/K+-ATPase pump, the primary target of digoxin, is responsible for actively transporting three sodium ions out of the cell for every two potassium ions it pumps into the cell, using adenosine triphosphate (ATP) as its energy source. This continuous action maintains a high extracellular potassium concentration and a low intracellular potassium concentration, essential for establishing and maintaining the negative resting membrane potential.
Digoxin exerts its positive inotropic effect by inhibiting this pump. With reduced Na+/K+-ATPase activity, intracellular sodium concentration rises. This increased intracellular sodium creates a favorable gradient for the sodium-calcium exchanger to operate in reverse, pumping sodium out and calcium in. The elevated intracellular calcium then enhances the force of myocardial contraction.
Hypokalemia: The Gateway to Digoxin Toxicity
The danger of hypokalemia in the context of digoxin therapy arises from its direct impact on the Na+/K+-ATPase pump and the cardiac cell’s membrane potential.
Increased Affinity of Digoxin for its Target
When serum potassium levels are low, there is a relative excess of extracellular potassium compared to intracellular potassium. The Na+/K+-ATPase pump has binding sites for both sodium and potassium. In a state of hypokalemia, the reduced extracellular potassium concentration leads to fewer potassium ions available to bind to the pump’s extracellular binding sites. Consequently, digoxin, which also binds to a site on the extracellular portion of the Na+/K+-ATPase pump, can more readily and avidly bind to the pump. This increased affinity means that even at therapeutic digoxin concentrations, a greater proportion of the Na+/K+-ATPase pumps can be inhibited, leading to an exaggerated intracellular sodium and calcium accumulation, and thus, a heightened risk of digoxin toxicity.
Membrane Destabilization and Increased Excitability
Hypokalemia also profoundly affects the resting membrane potential of cardiac cells. As mentioned, potassium’s outward movement establishes this potential. With less potassium available in the extracellular space, the membrane potential becomes less negative (more depolarized). This altered resting membrane potential makes the cardiac cells more excitable and susceptible to abnormal electrical activity.
In a normokalemic state, digoxin’s mechanism of increasing intracellular calcium is generally well-tolerated. However, in the presence of hypokalemia, the combined effects of increased calcium influx (due to pump inhibition) and enhanced cellular excitability (due to membrane depolarization) can trigger serious cardiac arrhythmias. These arrhythmias can range from premature ventricular contractions (PVCs) and bradycardia to more life-threatening ventricular tachycardia and fibrillation.
Symptoms and Manifestations of Digoxin Toxicity Exacerbated by Hypokalemia
The clinical presentation of digoxin toxicity is diverse and can be challenging to diagnose, especially when superimposed on other medical conditions. However, hypokalemia often amplifies and accelerates the onset of these symptoms.
Gastrointestinal symptoms are frequently the earliest indicators and include nausea, vomiting, anorexia, and abdominal pain. These are thought to be related to direct irritation of the gastrointestinal tract and effects on the chemoreceptor trigger zone in the brainstem.
Neurological symptoms can also manifest and may include headache, dizziness, confusion, fatigue, and visual disturbances. The classic visual symptom is blurred or yellow-tinted vision (xanthopsia), although this is less common.
Cardiac manifestations are the most dangerous. In the setting of hypokalemia, the risk of arrhythmias significantly increases. These can include:
- Bradycardia: A slow heart rate, often disproportionate to the intended effect of digoxin.
- Heart Block: Impaired conduction of electrical impulses through the atrioventricular (AV) node, leading to a dissociation between atrial and ventricular contractions.
- Ventricular Ectopy: Premature beats originating from the ventricles, such as PVCs, which can occur singly or in salvos.
- Ventricular Tachycardia and Fibrillation: Life-threatening rapid heart rhythms that can lead to cardiac arrest.
The presence of hypokalemia not only increases the likelihood of these arrhythmias but can also make them more refractory to standard antiarrhythmic treatments.
Other Electrolyte Imbalances and Their Impact on Digoxin
While hypokalemia is the most significant electrolyte abnormality associated with digoxin, other imbalances can also influence its pharmacodynamics and increase the risk of toxicity.
Hypomagnesemia (Low Serum Magnesium)
Magnesium plays a crucial role in maintaining cellular membrane stability and also interacts with the Na+/K+-ATPase pump. Hypomagnesemia can, similar to hypokalemia, lead to increased digoxin binding to the Na+/K+-ATPase and predispose to arrhythmias. Magnesium is a natural calcium channel blocker and also helps to stabilize the myocardial cell membrane. When magnesium levels are low, these stabilizing effects are diminished, making the heart more susceptible to digoxin-induced electrical disturbances. Therefore, in patients on digoxin, especially those with conditions that predispose to hypomagnesemia (e.g., diuretic use, malabsorption), magnesium levels should also be monitored.
Hypercalcemia (High Serum Calcium)
Calcium influx is a critical step in digoxin’s mechanism of increasing myocardial contractility. Elevated serum calcium levels can potentiate the effects of digoxin. When intracellular calcium is already high due to hypercalcemia, the additional calcium influx promoted by digoxin can push the myocardial cells into a state of excessive contractility and electrical instability, increasing the risk of arrhythmias. While not directly caused by digoxin, hypercalcemia can synergize with digoxin to produce toxic effects.
Hypocalcemia (Low Serum Calcium)
The role of hypocalcemia in digoxin toxicity is more complex and less definitively established than hypokalemia or hypercalcemia. However, some evidence suggests that severe hypocalcemia may reduce the threshold for digoxin-induced arrhythmias. It’s important to note that the overall effect of calcium on digoxin toxicity is concentration-dependent and can be influenced by other coexisting electrolyte abnormalities.
Management and Prevention Strategies
Given the profound impact of electrolyte imbalances on digoxin’s safety profile, a proactive and vigilant approach to management is essential.
Careful Patient Selection and Dosing
- Renal Function: Digoxin is primarily eliminated by the kidneys. Patients with impaired renal function are at significantly higher risk of digoxin accumulation and toxicity. Dosing must be carefully adjusted based on estimated glomerular filtration rate (eGFR).
- Therapeutic Drug Monitoring: Regular monitoring of serum digoxin levels is crucial, especially in patients with unstable renal function, suspected toxicity, or when initiating therapy. The therapeutic range for digoxin is narrow, and levels above 2.0 ng/mL are generally considered toxic, though toxicity can occur at lower levels, particularly in the presence of electrolyte imbalances.
- Understanding Drug Interactions: Numerous medications can interact with digoxin, affecting its absorption, distribution, metabolism, and excretion, thereby increasing the risk of toxicity. Diuretics, amiodarone, verapamil, and certain antibiotics are common culprits.
Proactive Electrolyte Management
- Routine Monitoring: Patients receiving digoxin should have their serum electrolytes, particularly potassium, magnesium, and calcium, monitored regularly. The frequency of monitoring should be tailored to the individual patient’s risk factors, concurrent medications (especially diuretics), and clinical status.
- Correction of Imbalances: Any identified electrolyte abnormalities must be promptly and appropriately corrected.
- Hypokalemia: This is typically managed with oral or intravenous potassium supplementation. The goal is to maintain serum potassium within the normal physiological range (typically 3.5-5.0 mEq/L). Caution is advised with rapid intravenous potassium administration due to the risk of precipitating arrhythmias.
- Hypomagnesemia: Magnesium supplementation, often intravenously in acute settings, is used to correct low magnesium levels.
- Hypercalcemia and Hypocalcemia: These require specific management strategies depending on the severity and underlying cause.
Patient Education
Educating patients about the signs and symptoms of digoxin toxicity and the importance of adhering to medication regimens and attending regular medical appointments is vital. Patients should be advised to report any new symptoms, especially nausea, vomiting, visual changes, or palpitations, immediately to their healthcare provider.
Conclusion
The relationship between digoxin and electrolyte balance, particularly potassium, is one of the most critical considerations in its therapeutic use. Digoxin does not directly cause hypokalemia; rather, hypokalemia is an electrolyte abnormality that significantly potentiates digoxin’s toxic effects. By impairing the normal function of the Na+/K+-ATPase pump and destabilizing cardiac cell membranes, low serum potassium levels dramatically increase the risk of life-threatening cardiac arrhythmias in patients taking digoxin. A thorough understanding of this pharmacodynamic interaction, coupled with vigilant monitoring of both digoxin levels and key electrolytes, is paramount to ensuring the safe and effective use of this valuable cardiac medication. Healthcare providers must remain acutely aware that while digoxin offers substantial benefits for selected cardiac conditions, its narrow therapeutic index necessitates a comprehensive approach that prioritizes electrolyte homeostasis.