Understanding the Anterior Cruciate Ligament and Its Injury
The anterior cruciate ligament (ACL) is a crucial component of the knee joint, playing a vital role in its stability and function. Situated within the knee, it runs diagonally across the tibia (shinbone) to the femur (thighbone). Its primary responsibility is to prevent the tibia from sliding too far forward relative to the femur, and to provide rotational stability to the knee. When this ligament is torn, it signifies a significant disruption to the knee’s biomechanics, often leading to a cascade of events that impact mobility, pain, and long-term joint health. Understanding the anatomy, mechanism of injury, and the subsequent physiological responses is key to comprehending the full impact of an ACL tear.
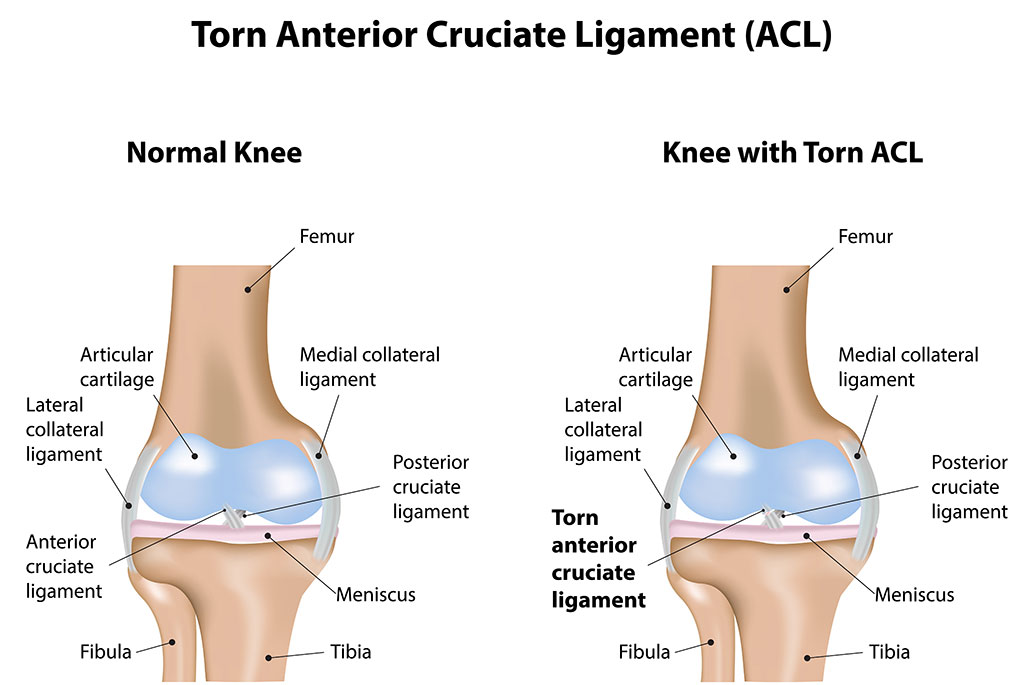
The knee joint itself is a complex interplay of bones, ligaments, tendons, and cartilage. The ACL, along with the posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL), forms the primary stabilizing structures of the knee. These ligaments act like strong, fibrous ropes, connecting bones to bones and restricting excessive movement. The ACL’s specific role in preventing anterior tibial translation is particularly important during activities that involve sudden changes in direction, jumping, and landing. Its elasticity and strength allow it to absorb significant forces, but these forces can also exceed its capacity, leading to a tear.
Tears can range in severity from a mild stretch (grade 1 sprain) to a complete rupture (grade 3 tear). In a complete tear, the ligament is severed into two pieces, rendering it incapable of fulfilling its stabilizing function. The immediate aftermath of such an injury is often characterized by a sudden, sharp pain, a popping sensation, and an inability to bear weight on the affected leg. Swelling typically develops rapidly due to bleeding within the joint, and the knee may feel unstable or “give way” with certain movements.
Mechanisms of ACL Injury
ACL tears are most commonly non-contact injuries, occurring during athletic activities that involve rapid deceleration, pivoting, or hyperextension of the knee. Sports such as soccer, basketball, football, skiing, and gymnastics are notorious for their high incidence of ACL injuries. The typical mechanism involves landing awkwardly from a jump with the foot planted, a sudden stop followed by a pivot, or a direct blow to the knee that forces it into an unnatural position.
-
Pivoting and Cutting: The most frequent cause of an ACL tear is a non-contact injury involving a rapid change in direction. When an athlete attempts to cut or pivot while their foot is planted, significant rotational forces are placed on the knee. If these forces exceed the ACL’s tensile strength, it can tear. This often happens when the knee is slightly bent and the foot is turned inward while the body continues to rotate.
-
Hyperextension: Another common mechanism is sudden hyperextension of the knee, where the knee is forced backward beyond its normal range of motion. This can occur during a fall or if an athlete lands heavily from a jump with their knee locked straight. The ACL can be stretched and torn under such extreme stress.
-
Landing from Jumps: Improper landing from jumps is a significant risk factor. Landing with the knee bent and the foot flat on the ground distributes forces more effectively. However, landing with the knee straight, or landing in a position where the knee collapses inward, can place excessive strain on the ACL.
-
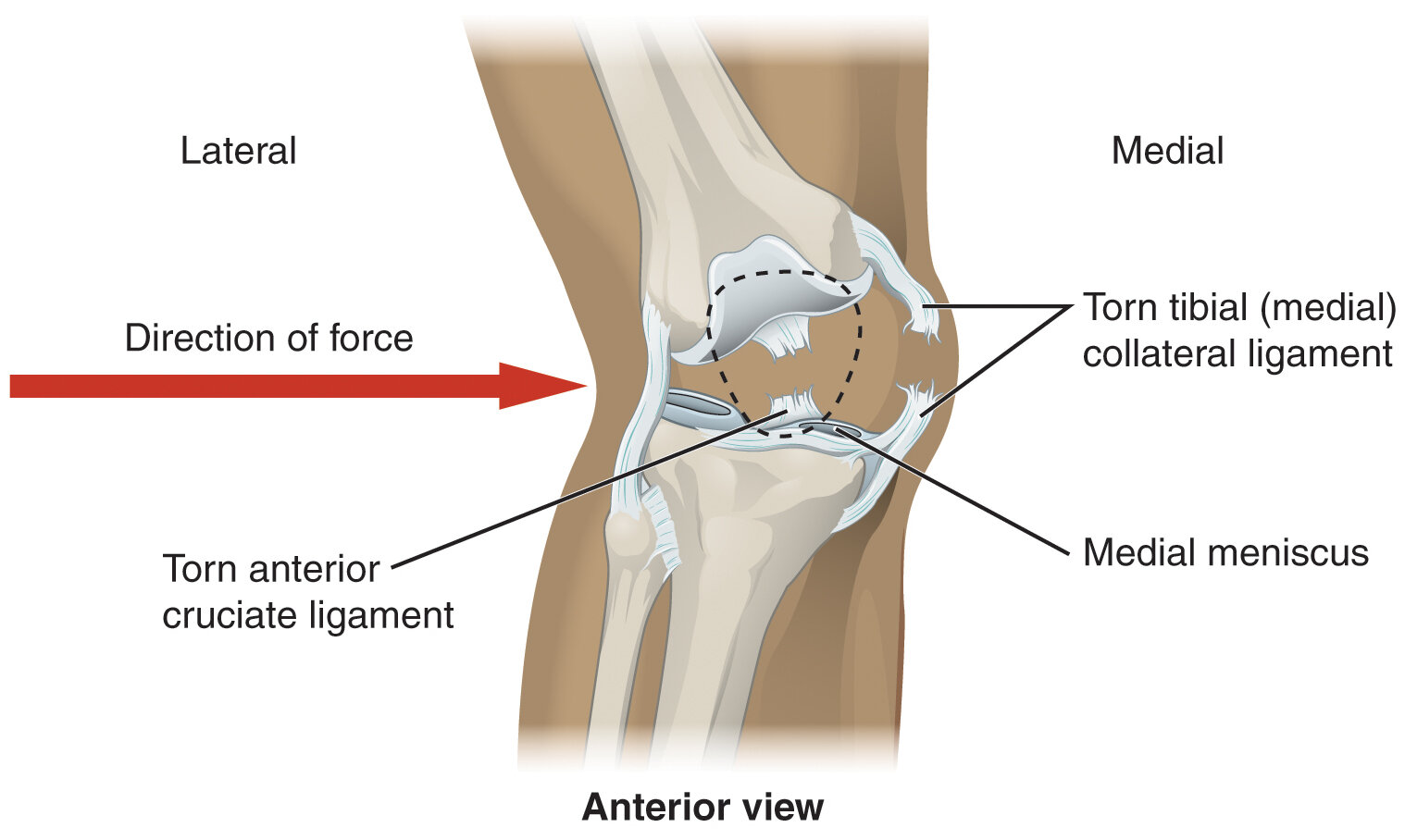
Direct Blows: While less common than non-contact injuries, a direct blow to the knee, particularly to the outside of the joint (valgus force), can also cause an ACL tear. This type of injury is often associated with damage to other structures as well, such as the MCL.
The forces involved in these mechanisms are substantial, and the susceptibility of the ACL can be influenced by factors such as muscle strength imbalances, fatigue, fatigue, and biomechanical deficiencies. Female athletes, for instance, have a higher incidence of ACL tears compared to males, which is thought to be due to differences in anatomy, neuromuscular control, and hormonal factors.
Immediate Consequences and Diagnosis
The immediate aftermath of an ACL tear is a traumatic event for the knee. The sudden disruption of the ligament’s integrity leads to an inflammatory response, characterized by pain, swelling, and a feeling of instability. The “pop” that many individuals report is believed to be the sound of the ligament tearing. Following the initial injury, the knee becomes painful and swollen, and weight-bearing often becomes difficult or impossible. The feeling of the knee “giving way” is a hallmark symptom, indicating the loss of crucial stability.
Recognizing the Symptoms
A clear understanding of the symptoms can aid in prompt diagnosis and treatment. While symptoms can vary slightly from person to person, several key indicators are commonly reported:
- A Loud Pop: Many individuals hear or feel a distinct “pop” at the time of injury. This is often the first indication that something significant has occurred.
- Severe Pain: Immediately following the tear, intense pain is usually experienced. This pain can subside somewhat as the initial shock wears off, but it remains a significant factor.
- Swelling: Within a few hours of the injury, the knee typically begins to swell. This swelling is due to bleeding from the torn ligament into the joint capsule.
- Loss of Range of Motion: The pain and swelling can restrict the ability to fully bend or straighten the knee.
- Instability and “Giving Way”: A persistent feeling of looseness or instability in the knee is common. The knee may feel like it will buckle or give out during weight-bearing or pivoting activities.
- Tenderness: The area around the knee joint may be tender to the touch, particularly along the joint line.
Diagnostic Process
Diagnosing an ACL tear involves a combination of a thorough medical history, a physical examination, and imaging studies. A healthcare professional will gather information about the mechanism of injury, the patient’s symptoms, and their activity levels.
- Physical Examination: The physician will perform several tests to assess the integrity of the ACL and other knee structures. These may include the Lachman test, anterior drawer test, and pivot shift test. These tests evaluate the degree of anterior tibial translation and rotational stability.
- Imaging Studies: While physical examination can strongly suggest an ACL tear, imaging is crucial for confirmation and to assess the extent of the damage, as well as any associated injuries.
- X-rays: X-rays are typically the first imaging modality used. They are effective at identifying bone fractures but do not visualize soft tissues like ligaments directly. However, they can help rule out bone injuries that might mimic ACL tear symptoms.
- MRI (Magnetic Resonance Imaging): An MRI is the gold standard for diagnosing ACL tears and other soft tissue injuries of the knee. It provides detailed images of the ligaments, cartilage, menisci, and other soft tissues, allowing for a precise assessment of the tear and any accompanying damage.
Associated Injuries
It’s important to note that ACL tears rarely occur in isolation. The forces that cause an ACL tear can also damage other structures within the knee. Common associated injuries include:
- Meniscal Tears: The menisci are C-shaped pieces of cartilage that act as shock absorbers between the femur and tibia. Tears to the medial or lateral meniscus are frequently seen with ACL injuries.
- Cartilage Damage: The articular cartilage that covers the ends of the bones can also be damaged, leading to a higher risk of osteoarthritis in the long term.
- Other Ligament Injuries: Tears to the MCL or LCL can occur in conjunction with an ACL tear, particularly in cases of direct trauma.
The Long-Term Implications and Treatment Pathways
A torn ACL significantly alters the biomechanics of the knee, leading to a range of long-term implications if not adequately addressed. The loss of anterior stability can result in chronic pain, recurrent episodes of the knee “giving way,” and further damage to other intra-articular structures. The management of an ACL tear typically involves a decision-making process that considers the individual’s age, activity level, the severity of the tear, and the presence of associated injuries.
Non-Surgical Management
For individuals who are less active, older, or who have sustained only a partial tear with minimal instability, non-surgical management may be an option. This approach focuses on rehabilitation and pain management.
- Rehabilitation Program: A comprehensive physical therapy program is essential. It aims to:
- Reduce pain and swelling.
- Restore full range of motion.
- Strengthen the muscles surrounding the knee, particularly the quadriceps and hamstrings, to compensate for the loss of ACL stability.
- Improve balance and proprioception (the body’s sense of its position in space).
- Gradually return to functional activities.
- Bracing: In some cases, a functional knee brace may be recommended to provide external support and stability during certain activities.
While non-surgical management can be successful for some, it is often associated with a higher risk of long-term instability and degenerative changes in the knee joint, especially for individuals who wish to return to high-impact sports.
Surgical Reconstruction
For athletes, active individuals, or those experiencing significant instability, surgical reconstruction of the ACL is often recommended. This procedure involves replacing the torn ligament with a graft.
- Graft Options: The graft material is typically harvested from the patient’s own body (autograft) or, less commonly, from a donor (allograft). Common autograft sources include:
- Patellar Tendon Graft: A portion of the patellar tendon, along with a small piece of bone from the kneecap and tibia, is used. This is a very strong and reliable graft.
- Hamstring Tendon Graft: Tendons from the hamstrings on the inner side of the thigh are harvested. This is another widely used and effective option.
- Quadriceps Tendon Graft: A portion of the quadriceps tendon above the kneecap can also be used.
- Surgical Procedure: Arthroscopic surgery is typically performed, meaning small incisions are made, and a camera (arthroscope) is used to visualize the inside of the knee. The surgeon drills tunnels in the tibia and femur, through which the graft is passed and secured.
- Post-Operative Rehabilitation: Surgery is only the first step. A rigorous and lengthy rehabilitation program is absolutely critical for a successful outcome. This program is phased and progresses from regaining range of motion and reducing swelling, to strengthening, proprioception training, and eventually, sport-specific drills. Full return to sport typically takes 9-12 months, and sometimes longer.

Long-Term Outlook and Prevention
The long-term outlook for individuals with ACL tears depends heavily on the chosen treatment pathway and adherence to rehabilitation. Those who undergo successful reconstruction and complete their rehabilitation have a good chance of returning to their previous level of activity. However, even with successful surgery, there is an increased risk of developing osteoarthritis in the injured knee later in life.
Preventing ACL injuries is a significant focus in sports medicine. Strategies include:
- Neuromuscular Training: Programs designed to improve balance, agility, landing mechanics, and muscle strength can significantly reduce the risk of ACL tears.
- Proper Technique: Emphasizing correct techniques for jumping, landing, and changing direction in sports.
- Conditioning: Maintaining adequate strength and endurance throughout the season to prevent fatigue, which can compromise biomechanics.
- Equipment: Ensuring appropriate footwear and playing surfaces can also play a role.
In conclusion, an ACL tear is a serious injury with far-reaching consequences for knee function and long-term joint health. While the immediate pain and instability are significant, the subsequent management, whether surgical or non-surgical, requires a dedicated commitment to rehabilitation to optimize recovery and mitigate future risks.