The term “flesh-eating disease” evokes a visceral sense of dread, conjuring images of rapid tissue destruction and severe illness. While commonly used, this alarming phrase is not a formal medical diagnosis. Instead, it refers to a group of rare but extremely severe bacterial infections known medically as necrotizing fasciitis. This condition is characterized by a rapidly spreading infection that destroys tissue, including muscle, fat, and the fascia—the connective tissue that surrounds muscles, nerves, fat, and blood vessels. Its aggressive nature and potential for devastating consequences necessitate immediate medical attention and a profound understanding of its mechanisms, risk factors, and treatment protocols.

Understanding Necrotizing Fasciitis: The Medical Term
Necrotizing fasciitis is a life-threatening soft tissue infection that progresses rapidly, leading to the death (necrosis) of the affected tissues. The name itself offers clues to its pathology: “necrotizing” refers to the death of cells and tissues, while “fasciitis” indicates inflammation of the fascia. This infection is not simply an external skin issue; it burrows deep beneath the surface, along the fascial planes, causing widespread destruction before visible skin changes become apparent. This deep-seated nature contributes significantly to the challenge of early diagnosis, as initial symptoms might be misleadingly mild compared to the severe underlying pathology.
The infection typically starts from a break in the skin, however minor, and then invades the subcutaneous tissue and fascia. The bacteria produce toxins that destroy tissue, impair blood flow, and hinder the body’s immune response, creating a vicious cycle of destruction. The rapid progression can lead to sepsis, multi-organ failure, and death if not treated aggressively and promptly. There are several types of necrotizing fasciitis, categorized based on the specific bacteria involved:
Types of Necrotizing Fasciitis
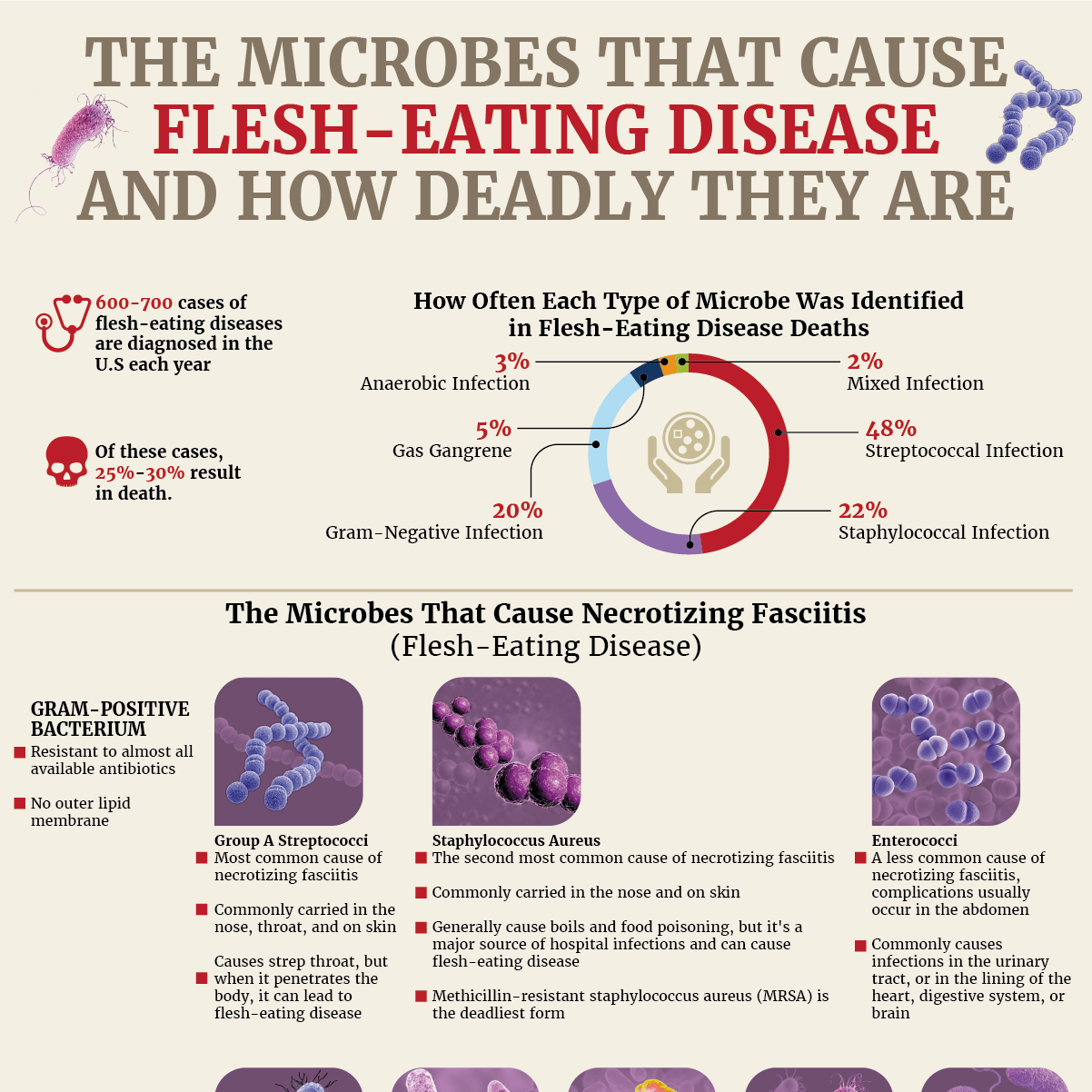
- Type I (Polymicrobial): This is the most common form, often occurring after surgery or in individuals with compromised immune systems. It involves a combination of different bacteria, typically anaerobic bacteria (like Bacteroides or Clostridium) alongside at least one facultative anaerobic bacterium (such as Escherichia coli, Klebsiella, or Group D streptococci). The synergistic action of these various bacteria contributes to its aggressive nature.
- Type II (Monomicrobial): This type is most frequently caused by Group A Streptococcus pyogenes (GAS), often referred to as “strep throat” bacteria. It can sometimes occur in conjunction with Staphylococcus aureus, including methicillin-resistant S. aureus (MRSA). Type II necrotizing fasciitis is particularly aggressive and is sometimes associated with streptococcal toxic shock syndrome.
- Type III (Gram-negative monomicrobial): Less common, this type is typically caused by marine bacteria, such as Vibrio vulnificus, and is often linked to exposure to contaminated seawater or raw seafood, especially in individuals with liver disease.
- Type IV (Fungal): Extremely rare, this form involves fungal pathogens and is usually seen in severely immunocompromised patients.
Understanding these distinctions helps medical professionals tailor treatment strategies, though the core principles of rapid intervention remain universal.
Causes and Risk Factors of Necrotizing Fasciitis
Necrotizing fasciitis is not contagious in the casual sense, meaning it doesn’t spread easily from person to person through simple contact like a common cold. Instead, it typically arises when bacteria enter the body through a break in the skin and find conditions conducive to rapid growth and spread. While anyone can develop necrotizing fasciitis, certain individuals are at a significantly higher risk due to pre-existing conditions or circumstances that compromise their immune system or skin integrity.
Entry Points and Bacterial Sources
The bacteria responsible for necrotizing fasciitis are ubiquitous in the environment and on human skin. Common entry points include:
- Cuts, scrapes, and punctures: Even minor skin injuries can provide an opening for bacteria.
- Surgical wounds: Post-operative sites can become infected, especially if proper wound care is not maintained.
- Insect bites and animal scratches: These can break the skin and introduce bacteria.
- Burns: Damaged skin from burns is highly susceptible to infection.
- Trauma: Any form of physical trauma that breaks the skin can be a portal of entry.
- Intravenous drug use: Contaminated needles and injection sites are significant risk factors.
- Childbirth: Rarely, bacteria can enter during the birthing process.
- Exposure to water: Certain bacteria like Vibrio vulnificus thrive in warm saltwater or brackish water and can infect open wounds exposed to it.
High-Risk Groups and Underlying Conditions
Several factors increase an individual’s susceptibility to developing necrotizing fasciitis:
- Compromised Immune System: Conditions that weaken the immune system, such as HIV/AIDS, cancer, or organ transplantation (requiring immunosuppressive drugs), significantly reduce the body’s ability to fight off infection.
- Diabetes Mellitus: Individuals with diabetes are particularly vulnerable due to impaired immune function, poor circulation, and nerve damage that can lead to unnoticed skin injuries.
- Peripheral Vascular Disease: Reduced blood flow to the extremities can impair tissue healing and make areas more prone to infection.
- Chronic Kidney Disease: Patients undergoing dialysis or with advanced kidney disease have a weakened immune response.
- Liver Disease (Cirrhosis): Particularly increases the risk of Vibrio vulnificus infections.
- Obesity: Increased tissue mass and potential for skin folds can create environments for bacterial growth.
- Intravenous Drug Use: Shared or unsterile needles can introduce bacteria directly into the bloodstream and tissues.
- Alcoholism: Chronic alcohol abuse can weaken the immune system and lead to nutritional deficiencies.
- Advanced Age: Elderly individuals often have weaker immune systems and more comorbidities.
- Malnutrition: A poorly nourished body is less equipped to fight off severe infections.
While these factors increase risk, it’s crucial to remember that even healthy individuals with no apparent risk factors can develop necrotizing fasciitis, emphasizing the need for vigilance regarding any unusual skin infection.
Recognizing the Symptoms: Early Detection is Crucial
The insidious nature of necrotizing fasciitis lies in its ability to mimic less severe infections in its early stages. This delay in recognition is often the most critical factor influencing patient outcomes, as the infection spreads rapidly. Early and accurate diagnosis is paramount to initiating life-saving treatment.
The symptoms typically progress over a period of hours to days, becoming increasingly severe:
Initial Symptoms (often within 24-48 hours)
- Severe pain disproportionate to the visible injury: This is a hallmark symptom. The pain is far more intense than one would expect from the apparent size or nature of the wound. It may also extend beyond the visible area of redness.
- Intense redness, warmth, and swelling: Similar to cellulitis or other localized infections, but often spreading very quickly.
- Fever and flu-like symptoms: Chills, fatigue, and general malaise are common as the body fights the infection.
- Tenderness to the touch: The affected area is extremely sensitive.
Later Symptoms (within days)
As the infection progresses, more alarming signs begin to appear:
- Blisters (bullae): Fluid-filled blisters may form on the skin, often containing dark, foul-smelling fluid.
- Skin discoloration: The skin may change from red to purple, then to a dusky blue or grayish color, indicating tissue death.
- Numbness: As nerves are destroyed, the intense pain may give way to numbness in the affected area, which is a very concerning sign.
- Skin necrosis: Patches of skin may turn black and slough off.
- Crepitus: A crackling sensation under the skin, indicating the presence of gas produced by certain bacteria.
- Systemic toxicity/Sepsis: Signs of severe systemic illness include low blood pressure, rapid heart rate, confusion, dizziness, and organ failure, as the infection overwhelms the body.
If any of these symptoms, especially the disproportionate pain or rapid progression, are suspected, immediate medical evaluation is critical. Do not wait for symptoms to worsen; every hour counts.
Diagnosis and Treatment: A Race Against Time
Diagnosing necrotizing fasciitis is primarily a clinical assessment, given the urgency. While laboratory and imaging tests provide valuable support, treatment often begins based on strong clinical suspicion. The overarching goal is to identify the infection and intervene aggressively before irreversible damage or systemic collapse occurs.
Diagnostic Approaches
- Clinical Examination: The characteristic signs and symptoms, especially the severe pain out of proportion to skin findings, are key.
- Blood Tests: Elevated white blood cell count, markers of inflammation (e.g., C-reactive protein), and signs of kidney or liver dysfunction can point to severe infection and sepsis.
- Imaging Studies:
- X-rays: May show gas in the soft tissues, though this is not always present.
- CT Scans or MRI: Can reveal swelling and fluid collection along the fascial planes, helping to define the extent of the infection and guide surgical planning.
- Tissue Biopsy and Culture: The definitive diagnosis is often made by surgical exploration and tissue biopsy, where samples of the affected tissue are sent for Gram stain and bacterial culture to identify the specific pathogens and their antibiotic sensitivities. This is crucial for guiding targeted antibiotic therapy.
Treatment Strategies
Treatment for necrotizing fasciitis is intensive and multifaceted, often requiring a multidisciplinary team approach.
- Emergency Surgical Debridement: This is the cornerstone of treatment and must be performed immediately upon diagnosis. The surgeon removes all dead and infected tissue until healthy, bleeding tissue is reached. Multiple surgical procedures may be necessary as the infection can continue to spread, requiring repeated debridement every 12-24 hours. The goal is to remove the source of bacterial proliferation and toxin production.
- Broad-Spectrum Intravenous Antibiotics: High-dose antibiotics are administered intravenously as soon as necrotizing fasciitis is suspected, even before definitive culture results are available. These antibiotics are chosen to cover a wide range of potential bacteria (broad-spectrum) and are later tailored once culture results and sensitivities are known.
- Intensive Supportive Care: Patients typically require admission to an intensive care unit (ICU) for close monitoring and support of vital organ function. This may include intravenous fluids to combat dehydration and shock, medications to support blood pressure, blood transfusions, and respiratory support if lung function is compromised.
- Adjunctive Therapies (Less Common but Used in Specific Cases):
- Hyperbaric Oxygen Therapy (HBOT): Some evidence suggests that HBOT, which involves breathing pure oxygen in a pressurized chamber, can help by increasing oxygen delivery to infected tissues, inhibiting anaerobic bacteria, and enhancing the effect of certain antibiotics.
- Intravenous Immunoglobulin (IVIG): For cases involving Group A Streptococcus, IVIG may be considered as it contains antibodies that can help neutralize bacterial toxins.
Amputation of a limb may be necessary if the infection is too widespread or untreatable by debridement alone to save the patient’s life. Rehabilitation, including physical therapy and wound care, is a long and challenging process for survivors.
Prevention and Prognosis
While necrotizing fasciitis is rare, understanding how to minimize risk and recognizing the critical role of early intervention is essential.
Prevention Strategies
- Proper Wound Care: Clean all cuts, scrapes, and wounds thoroughly with soap and water. Cover open wounds with clean bandages.
- Hygiene: Regular handwashing, especially after outdoor activities or contact with potential sources of bacteria, can reduce the risk of infection.
- Avoid Contaminated Water with Open Wounds: If you have an open wound, avoid swimming in or exposing it to warm brackish or saltwater, especially if you have liver disease or a weakened immune system.
- Manage Chronic Conditions: Individuals with diabetes, liver disease, or other chronic conditions should diligently manage their health to strengthen their immune system.
- Prompt Medical Attention: Do not delay seeking medical care for any wound that appears infected or is accompanied by severe, rapidly worsening pain.

Prognosis and Long-Term Outcomes
The prognosis for necrotizing fasciitis depends heavily on the speed of diagnosis and the aggressiveness of treatment. Despite advances in medical care, the mortality rate remains significant, ranging from 20% to as high as 70% in some severe cases or delayed presentations.
Survivors often face a long and challenging recovery. Long-term complications can include:
- Extensive Scarring and Disfigurement: The surgical removal of large amounts of tissue leaves significant scarring, often requiring reconstructive surgery or skin grafting.
- Limb Amputation: If the infection cannot be controlled, amputation may be necessary to save the patient’s life.
- Functional Impairment: Damage to muscles and nerves can lead to chronic pain, weakness, and loss of function in the affected area, requiring intensive physical therapy and rehabilitation.
- Psychological Impact: The traumatic experience of necrotizing fasciitis, combined with physical disfigurement and functional limitations, can lead to significant psychological distress, including anxiety, depression, and post-traumatic stress disorder.
The term “flesh-eating disease” truly reflects the devastating power of necrotizing fasciitis. While terrifying, awareness of its medical name, risk factors, and particularly its early symptoms empowers individuals to seek immediate help, which remains the single most important factor in improving outcomes and saving lives.