Gastroesophageal reflux disease (GERD) is a common condition in infants, characterized by the backward flow of stomach contents into the esophagus. While a certain amount of reflux is normal for babies, GERD occurs when this reflux becomes problematic, leading to symptoms that affect the infant’s health and well-being. Understanding the nuances of GERD in infants is crucial for parents and caregivers to provide appropriate care and seek timely medical intervention when necessary. This article delves into the definition, causes, symptoms, diagnosis, and management of GERD in infants, offering a comprehensive overview for those navigating this challenging, yet often manageable, condition.
Understanding the Basics of Infant Reflux and GERD
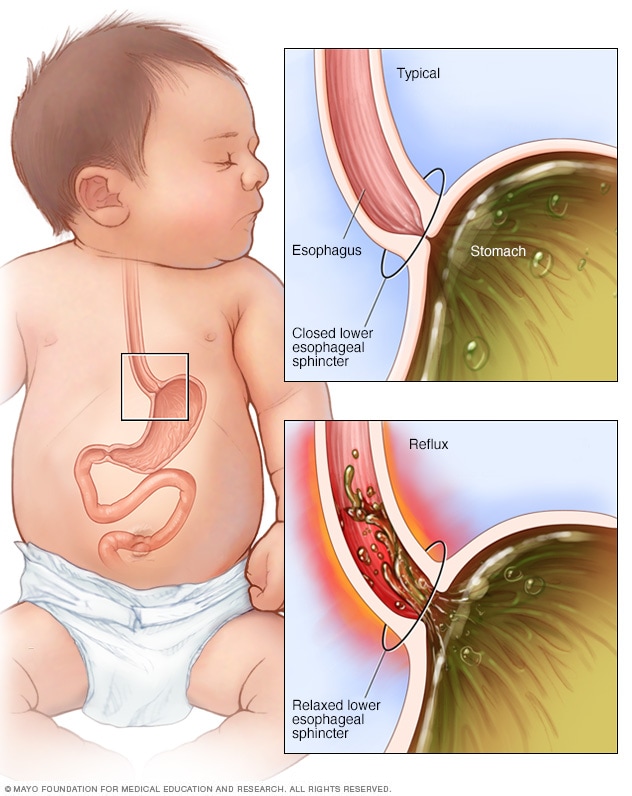
The digestive system of an infant is still developing, and this immaturity plays a significant role in the prevalence of reflux. The lower esophageal sphincter (LES), a muscular ring at the bottom of the esophagus that acts as a valve between the esophagus and the stomach, is often weaker in infants. This weakness allows stomach contents, including food and acid, to easily flow back up into the esophagus. This backward flow is known as gastroesophageal reflux (GER).
Gastroesophageal Reflux (GER) vs. Gastroesophageal Reflux Disease (GERD)
It’s important to distinguish between GER and GERD. GER is a physiological process that occurs in most infants, often during or after feeding. It is typically harmless and resolves on its own as the infant’s digestive system matures. Symptoms of simple GER might include occasional spitting up or vomiting, but without distress or complications.
GERD, on the other hand, is a more severe and persistent form of reflux. It occurs when the frequent or significant reflux of stomach contents causes troublesome symptoms or complications. These complications can include poor weight gain, respiratory problems, irritability, and feeding difficulties. GERD is a medical diagnosis that requires attention from a healthcare professional.
The Developing Digestive System
The infant digestive tract is designed for rapid growth and development. During infancy, the LES is not fully developed or coordinated. Its primary function is to prevent the reflux of stomach contents. In infants, this muscle may relax inappropriately or not close tightly enough, facilitating the upward movement of food and gastric acid. Additionally, the infant stomach empties more slowly than in older children or adults, meaning that food stays in the stomach for a longer period, increasing the chances of reflux. The upright posture of an infant after feeding can also contribute to reflux. As the infant grows, gains head and neck control, and adopts a more upright posture after meals, the LES typically matures, and the frequency and severity of reflux often decrease.
Symptoms of GERD in Infants
The symptoms of GERD in infants can vary widely in presentation and severity. Some infants may exhibit only mild discomfort, while others can experience significant distress. It’s the persistence, severity, and impact on the infant’s well-being that differentiate GERD from normal spitting up.
Feeding and Digestive Symptoms
- Spitting Up and Vomiting: This is the most common symptom. While occasional spitting up is normal, frequent, forceful, or large volume vomiting can be indicative of GERD. The vomitus may be curdled milk or appear clear if it contains stomach acid.
- Poor Weight Gain or Weight Loss: If the reflux is severe enough to cause pain during feeding or significant nutrient loss, an infant may struggle to gain weight appropriately or even lose weight. This is a serious concern and warrants medical evaluation.
- Feeding Refusal or Difficulties: Infants with GERD may associate feeding with pain or discomfort. This can lead to arching their backs, crying, or pulling away from the breast or bottle during or after feeds. They may also take only small amounts of milk or refuse to eat altogether.
- Irritability and Fussiness: GERD can cause significant discomfort, leading to constant fussiness, crying, and difficulty soothing the infant, particularly after feedings or when lying flat.
Respiratory and Other Symptoms
- Choking or Gagging: The refluxed stomach contents can irritate the airway, leading to choking or gagging episodes, sometimes even during feeding.
- Coughing: A persistent, dry cough, especially one that worsens when lying down or after feeding, can be a symptom of GERD. The stomach acid can irritate the throat and airways.
- Wheezing and Respiratory Distress: In more severe cases, refluxed material can be aspirated into the lungs, leading to inflammation, wheezing, and difficulty breathing. This can mimic symptoms of other respiratory conditions like asthma or bronchiolitis.
- Arching of the Back (Sandifer Syndrome): Some infants with GERD develop a characteristic posture of arching their back and stiffening their body during or after feeding. This is thought to be an attempt to relieve discomfort by changing body position and reducing pressure on the esophagus.
- Sleep Disturbances: Discomfort from reflux can disrupt an infant’s sleep, leading to frequent awakenings, difficulty settling, and shorter sleep durations.
Causes and Risk Factors for Infant GERD
While an immature LES is the primary physiological factor contributing to reflux in infants, other factors can exacerbate or contribute to the development of GERD.
Immaturity of the Lower Esophageal Sphincter (LES)
As mentioned, the LES is a crucial muscle preventing the backward flow of stomach contents. In infants, this sphincter is often weak and may relax at inappropriate times, allowing stomach contents to reflux into the esophagus. This immaturity is a normal developmental phase, but in some infants, it leads to symptomatic GERD.
Other Contributing Factors
- Overfeeding: Feeding an infant too much can increase the volume of stomach contents, potentially leading to more frequent or severe reflux.
- Feeding Position: Feeding an infant in a reclined position, rather than a more upright one, can make it easier for stomach contents to flow back into the esophagus.
- Certain Food Allergies or Intolerances: In some cases, allergies or intolerances to proteins in the infant’s diet (e.g., cow’s milk protein) can trigger inflammation and irritation in the digestive tract, potentially worsening reflux symptoms.
- Prematurity: Premature infants often have more underdeveloped digestive systems, including a weaker LES, making them more prone to GERD.
- Neurological Conditions: Infants with certain neurological conditions that affect muscle control and coordination may be at higher risk for GERD due to impaired esophageal motility or LES function.
- Anatomical Abnormalities: While less common, certain congenital anatomical abnormalities in the digestive tract can contribute to reflux.
Diagnosis of GERD in Infants

Diagnosing GERD in infants often involves a combination of medical history, physical examination, and sometimes diagnostic tests. Because many symptoms overlap with normal infant behavior, a careful evaluation by a pediatrician is essential.
Medical History and Physical Examination
The pediatrician will begin by taking a detailed medical history, asking about the infant’s feeding patterns, weight gain, crying episodes, sleep habits, and any other symptoms observed. The physical examination will assess the infant’s overall health, growth parameters, and check for any physical signs that might indicate an underlying problem.
Diagnostic Tests (When Necessary)
In most cases, GERD is diagnosed clinically based on the infant’s symptoms and response to initial treatment. However, in more complex or persistent cases, or when other conditions are suspected, the pediatrician may recommend one or more of the following tests:
- Esophageal pH Monitoring: This test involves placing a thin, flexible tube with a sensor through the infant’s nose into the esophagus. The sensor measures the acidity of the contents in the esophagus over a 24-hour period. Frequent episodes of low pH indicate significant acid reflux. This is considered the gold standard for diagnosing acid reflux.
- Esophageal Impedance Testing: This test can detect both acid and non-acidic reflux. A similar tube is placed in the esophagus, and it measures changes in electrical resistance as fluid moves through the esophagus. This test is particularly useful for infants whose symptoms are not solely due to acid.
- Upper Endoscopy: In rare and severe cases, an upper endoscopy may be performed. This involves inserting a thin, flexible tube with a camera (endoscope) into the infant’s esophagus, stomach, and duodenum. This allows the doctor to directly visualize the lining of these organs and take biopsies if necessary to check for inflammation, irritation, or other abnormalities.
- Barium Swallow (Esophagram): This test involves the infant drinking a liquid containing barium, which coats the digestive tract and makes it visible on X-rays. It can help identify structural abnormalities in the esophagus or stomach and assess the degree of reflux. However, it doesn’t measure the frequency or duration of reflux.
Management and Treatment of Infant GERD
The primary goal of managing infant GERD is to alleviate symptoms, ensure adequate growth, and prevent complications. Treatment strategies are often tiered, starting with conservative measures and progressing to medication if necessary.
Lifestyle and Feeding Modifications
These are typically the first line of treatment and are often highly effective for milder cases.
- Thickening Feedings: Healthcare providers may recommend adding a thickening agent (e.g., rice cereal or specialized infant thickeners) to formula or breast milk. This can help keep the milk in the stomach longer, reducing the likelihood of reflux. It’s important to follow specific guidelines from a healthcare professional regarding the type and amount of thickener.
- Smaller, More Frequent Feedings: Instead of large, infrequent feeds, offering smaller volumes of milk more often can help prevent the stomach from becoming too full.
- Upright Posture: Keeping the infant in an upright position during and for at least 20-30 minutes after feedings can help gravity keep stomach contents down. Avoid placing the infant flat on their back immediately after feeding.
- Burping: Ensuring the infant is adequately burped during and after feedings can help release swallowed air, which can contribute to reflux.
- Avoiding Overstimulation: Sometimes, a calm feeding environment can help.
Positioning and Sleep
- Elevating the Head of the Crib: While not universally recommended due to potential safety concerns like suffocation, some healthcare providers may suggest elevating the head of the crib by placing firm blocks or books under the mattress legs. Crucially, never prop an infant up with pillows or wedges in the crib as this poses a serious suffocation risk. The infant should always sleep on their back on a firm, flat surface.
- Side Sleeping: While infants should always sleep on their back for safety, some temporary side positioning might be discussed with a doctor for short periods while awake and supervised, if deemed appropriate for reflux relief.
Medications
If lifestyle modifications are insufficient, a pediatrician may prescribe medications to reduce stomach acid or improve LES function.
- Acid Reducers (H2 Blockers and Proton Pump Inhibitors – PPIs): Medications like ranitidine (though less commonly used now), famotidine (H2 blockers), or omeprazole, lansoprazole (PPIs) work by reducing the amount of acid produced by the stomach. This can help alleviate the burning sensation and pain associated with acid reflux. These medications are typically used for short periods to manage symptoms.
- Prokinetics: In some rare instances, medications that help the stomach empty faster or improve the coordination of the digestive tract may be considered, but these are used cautiously due to potential side effects.
Surgical Intervention
Surgery for GERD in infants is very rare and is usually reserved for severe cases that do not respond to medical management and have led to serious complications, such as failure to thrive or severe respiratory problems. The most common surgical procedure is a fundoplication, where the upper part of the stomach is wrapped around the LES to strengthen it and prevent reflux.

When to Seek Medical Advice
It is vital for parents and caregivers to consult a pediatrician if they suspect their infant has GERD or if the infant exhibits any of the following:
- Persistent vomiting that is forceful or in large volumes.
- Poor weight gain or weight loss.
- Difficulty feeding, refusal to eat, or significant distress during feeding.
- Frequent choking or gagging episodes.
- Blood in vomit or stool.
- Signs of respiratory distress, such as wheezing, rapid breathing, or pauses in breathing.
- Excessive irritability and inconsolable crying that is not relieved by usual comforting measures.
- Green or yellow vomit.
While reflux is a common part of infancy, recognizing the signs and symptoms of GERD and seeking professional guidance ensures that infants receive the appropriate care to thrive. With proper diagnosis and management, most infants with GERD can experience significant relief and continue to grow and develop healthily.