Understanding Phosphate Binders: A Critical Component in Kidney Health Management
Phosphate, a mineral essential for bone health and cellular function, plays a crucial role in numerous biological processes. However, when the kidneys are unable to effectively filter excess phosphate from the blood, a condition known as hyperphosphatemia can arise. This is particularly common in individuals with chronic kidney disease (CKD). Elevated phosphate levels can lead to serious health complications, including cardiovascular disease, bone disorders (renal osteodystrophy), and the formation of painful calcium-phosphate deposits in soft tissues. Managing phosphate levels is therefore a cornerstone of treatment for patients with CKD. This is where phosphate binders, also known as phosphate-chelating agents, become indispensable. These medications are designed to work within the digestive system, binding to dietary phosphate and preventing its absorption into the bloodstream.

The Physiology of Phosphate Homeostasis and Dysregulation in CKD
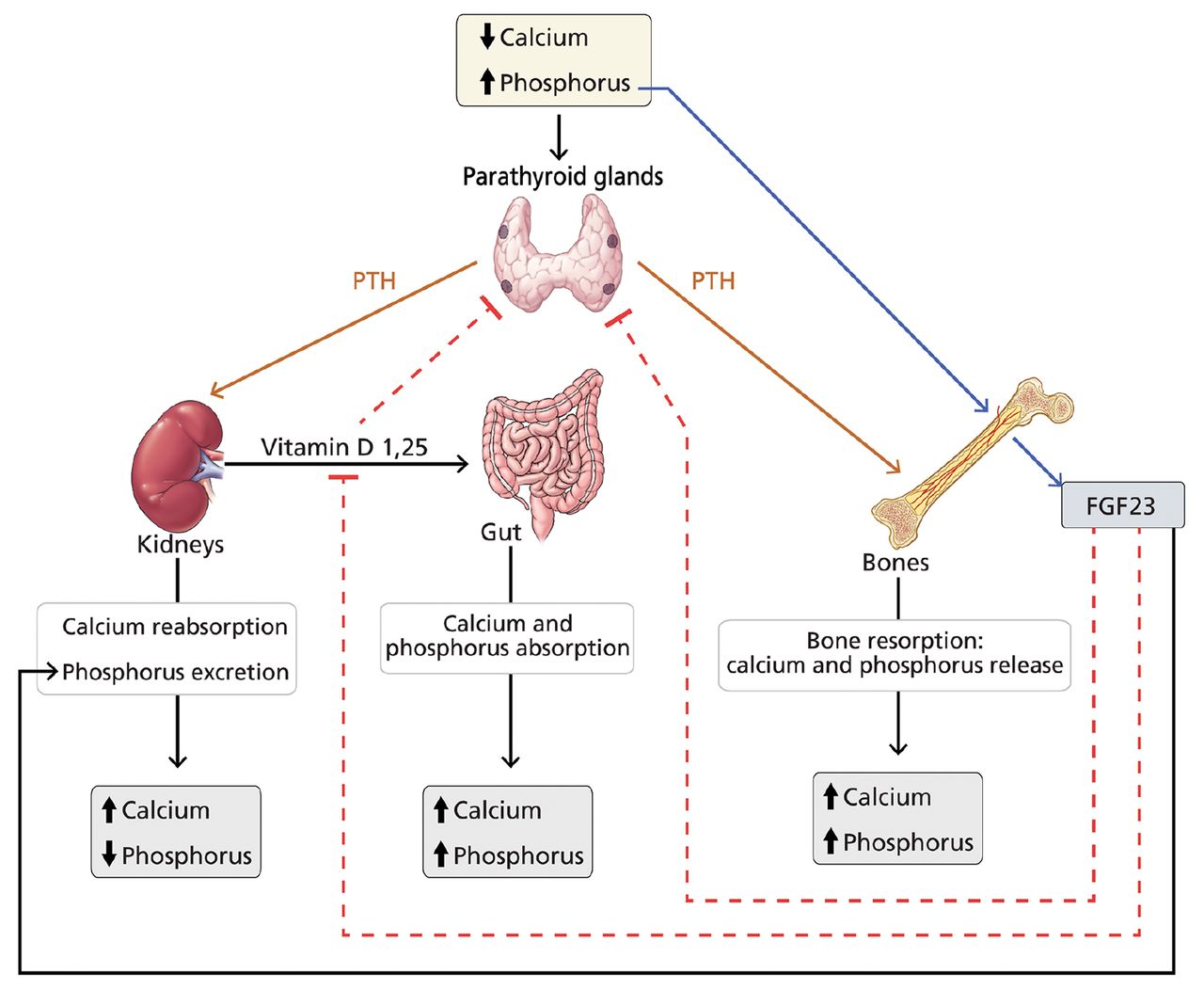
Phosphate homeostasis, the delicate balance of phosphate levels in the body, is primarily regulated by the kidneys. Through glomerular filtration and tubular reabsorption, healthy kidneys maintain serum phosphate within a narrow, optimal range. However, in CKD, the declining glomerular filtration rate (GFR) impairs the kidneys’ ability to excrete excess phosphate. This leads to a gradual increase in serum phosphate levels. Furthermore, impaired kidney function affects the production of calcitriol (the active form of Vitamin D), which is crucial for calcium absorption. Reduced calcitriol and increased serum phosphate also stimulate the parathyroid glands to produce more parathyroid hormone (PTH). Elevated PTH (secondary hyperparathyroidism) further exacerbates phosphate retention, creating a vicious cycle that contributes to complex metabolic disturbances.
Beyond the direct impact on bone and cardiovascular health, hyperphosphatemia can also interfere with calcium balance. When serum phosphate levels are high, they tend to bind with calcium, leading to a decrease in free, ionized calcium. This hypocalcemia can trigger further PTH release, attempting to raise both calcium and phosphate levels, a counterproductive outcome in the context of CKD. The long-term consequences of unmanaged hyperphosphatemia are severe, including increased mortality and morbidity, making effective phosphate control a paramount objective in CKD management.
The Mechanism of Action: How Phosphate Binders Work
Phosphate binders function by interacting with phosphate ions directly within the gastrointestinal tract. After ingestion, these binders are released in the stomach and small intestine where they encounter the phosphate present in food. The active component of the binder forms a chemical complex, or chelation, with the phosphate ions. This binding effectively renders the phosphate insoluble and, more importantly, unabsorbable by the intestinal lining. Consequently, the bound phosphate is then eliminated from the body through feces, bypassing the bloodstream and preventing an increase in serum phosphate levels.
The efficacy of a phosphate binder is determined by several factors, including its binding capacity (how much phosphate it can bind), its affinity for phosphate, its dissolution rate in the gastrointestinal tract, and its dosage. The goal is to achieve a significant reduction in phosphate absorption without causing undue gastrointestinal side effects or interfering with the absorption of other essential nutrients, such as calcium, iron, or vitamins. The timing of administration is also critical. Phosphate binders are most effective when taken with meals, as this is when dietary phosphate is most readily available for binding.
Types of Phosphate Binders: A Diverse Pharmacological Arsenal
The development of phosphate binders has evolved significantly, offering a range of options with different chemical compositions and varying profiles of efficacy and side effects. These can be broadly categorized based on their primary chemical constituents:
Calcium-Based Binders
Calcium carbonate and calcium acetate are among the oldest and most commonly prescribed phosphate binders.
- Calcium Carbonate: This readily available and inexpensive agent acts as a binder by forming insoluble calcium phosphate complexes in the gut. It also provides a source of supplemental calcium, which can be beneficial for patients with CKD who often have calcium deficiencies. However, excessive calcium absorption from calcium carbonate can lead to hypercalcemia, a serious condition characterized by abnormally high calcium levels. This risk is particularly elevated in patients also taking active Vitamin D supplements.
- Calcium Acetate: Calcium acetate also binds phosphate effectively and provides calcium. It is generally considered to have a higher affinity for phosphate than calcium carbonate and may result in less calcium absorption, thus potentially reducing the risk of hypercalcemia. However, it can still contribute to elevated calcium levels, and its acetate component can be metabolized to bicarbonate, which may be a concern in patients with metabolic alkalosis.
Non-Calcium, Non-Aluminum Binders
Recognizing the risks associated with both long-term calcium and aluminum accumulation, newer generations of phosphate binders have been developed.
- Sevelamer Hydrochloride and Sevelamer Carbonate: Sevelamer is a non-absorbed polymer that works by binding to phosphate in the intestinal lumen. It does not contain calcium or aluminum, thus avoiding the risks of hypercalcemia and aluminum toxicity. Sevelamer hydrochloride has an anion exchange capacity that binds phosphate. Sevelamer carbonate is a related compound that also binds phosphate and has the added benefit of increasing serum bicarbonate levels, which can be advantageous for patients with metabolic acidosis often seen in CKD. Sevelamer can also bind bile acids, potentially leading to reduced absorption of fat-soluble vitamins (A, D, E, K) and some medications, necessitating careful monitoring and potential supplementation.
- Lanthanum Carbonate: Lanthanum is a rare earth element that acts as a potent phosphate binder. Lanthanum carbonate is formulated to release lanthanum ions in the gastrointestinal tract, which then bind to dietary phosphate. Like sevelamer, it is not absorbed into the bloodstream and therefore does not contribute to systemic calcium or aluminum overload. Lanthanum has a high binding capacity and a strong affinity for phosphate. While generally well-tolerated, gastrointestinal side effects such as nausea and vomiting can occur. Long-term studies have also examined the accumulation of lanthanum in tissues, but clinical significance remains under investigation.
Other and Emerging Binders
The pursuit of even more effective and better-tolerated phosphate binders continues.
-
Iron-Based Binders (e.g., Ferric Citrate): Ferric citrate is a relatively newer phosphate binder that offers a dual benefit. It binds to dietary phosphate, forming insoluble ferric phosphate, thereby reducing absorption. Importantly, it also delivers a modest amount of elemental iron, which can help improve iron deficiency anemia – a common comorbidity in CKD patients. This dual action can simplify treatment regimens. However, potential side effects include gastrointestinal disturbances and the risk of iron overload if not managed carefully.
-
Other Novel Agents: Research and development are ongoing, exploring new chemical entities and delivery mechanisms for phosphate binders. These may include compounds with enhanced binding capacities, improved gastrointestinal tolerability, or novel mechanisms of action.
Clinical Considerations and Management Strategies
The selection of an appropriate phosphate binder is a personalized decision that takes into account a patient’s individual clinical profile, including their degree of hyperphosphatemia, the presence of hypercalcemia or hypocalcemia, the status of secondary hyperparathyroidism, comorbidities, and tolerance to previous treatments. A collaborative approach involving the nephrologist, registered dietitian, and pharmacist is crucial for optimal management.
Dosing and Administration
The effectiveness of phosphate binders is highly dependent on proper dosing and adherence to administration schedules.
- Timing: As mentioned, phosphate binders are most effective when taken with meals or snacks that contain phosphate. This ensures that the binder is present in the digestive tract concurrently with dietary phosphate. Patients are typically advised to take their binders with the first bite of food.
- Dosage Titration: The dosage of phosphate binders is not fixed and often needs to be adjusted based on regular monitoring of serum phosphate levels. The goal is to achieve and maintain target phosphate levels as recommended by clinical guidelines.
- Adherence: Patient adherence is a significant challenge in the management of CKD. The need to take multiple medications with meals can be burdensome. Education about the importance of phosphate control and strategies to improve adherence, such as pill organizers or simplified dosing regimens, are vital.
Monitoring and Side Effects
Regular monitoring of serum phosphate, calcium, PTH, and alkaline phosphatase levels is essential to assess the efficacy of phosphate binders and to detect potential adverse effects.
- Gastrointestinal Side Effects: Nausea, vomiting, diarrhea, constipation, and abdominal pain are common side effects associated with many phosphate binders. These can impact adherence and quality of life.
- Hypercalcemia: As discussed, calcium-based binders carry a risk of hypercalcemia. Monitoring calcium levels regularly is crucial, especially when using these agents in conjunction with active Vitamin D analogs.
- Drug Interactions: Phosphate binders can interfere with the absorption of other medications. It is important to advise patients to separate the administration of their phosphate binders from other oral medications by at least one to two hours.
- Nutritional Deficiencies: Non-calcium, non-aluminum binders, such as sevelamer, can potentially reduce the absorption of fat-soluble vitamins and other micronutrients. Regular assessment of nutritional status and appropriate supplementation may be necessary.
The Role of Diet
While phosphate binders are critical for managing hyperphosphatemia, dietary modification remains a fundamental component of therapy. A low-phosphate diet, limiting intake of high-phosphate foods such as dairy products, processed meats, colas, and certain grains, is essential. A registered dietitian specializing in renal nutrition plays a pivotal role in educating patients about dietary choices and developing personalized meal plans that are both nutritionally sound and effectively manage phosphate intake. The interplay between diet and medication is symbiotic; a well-managed diet reduces the burden on the phosphate binder, while the binder helps mitigate the absorption of any unavoidable dietary phosphate.

Conclusion: Optimizing Phosphate Control for Improved Renal Outcomes
Phosphate binders are indispensable tools in the multifaceted management of chronic kidney disease. By effectively binding dietary phosphate within the gastrointestinal tract, they prevent its absorption into the bloodstream, thereby mitigating the detrimental effects of hyperphosphatemia on bone health, cardiovascular function, and overall morbidity and mortality. The evolution of phosphate binders from early calcium-based agents to more sophisticated polymeric and metal-based compounds reflects a continuous effort to enhance efficacy while minimizing adverse effects.
The successful management of phosphate levels requires a comprehensive strategy that integrates pharmacological therapy with careful dietary counseling and regular clinical monitoring. Patient education, adherence support, and a personalized approach to binder selection are paramount. As research progresses, the development of novel binders with improved safety profiles and enhanced efficacy promises further advancements in the care of patients with kidney disease, ultimately aiming to improve their quality of life and long-term health outcomes.