Dysplasia, in the context of biological tissues and cellular development, refers to an abnormality in the size, shape, and organization of adult cells. It is not a disease in itself but rather a precancerous condition, a significant deviation from the normal cellular structure that can, if left unaddressed, potentially progress to cancer. Understanding dysplasia is crucial for early detection and intervention, particularly in fields like medical imaging, pathology, and in the development of diagnostic technologies.
Understanding Cellular Aberrations
At its core, dysplasia represents a disruption in the normal process of cellular differentiation and maturation. Cells are the fundamental building blocks of all living organisms, and their development is meticulously regulated by genetic signals and environmental cues. When these processes go awry, cells can begin to exhibit unusual characteristics, deviating from their healthy counterparts.
Cellular Morphology
Healthy cells typically possess a predictable and consistent morphology (shape and structure). They have a well-defined nucleus, cytoplasm, and cell membrane, and these components are arranged in an orderly fashion. In dysplastic cells, this order is lost. The nucleus, often the most indicative site of abnormality, may become enlarged (macronucleosis), hyperchromatic (darkly stained due to excess DNA), irregular in shape, or exhibit an increased number of mitotic figures (cells undergoing division), which are often abnormal in appearance. The cytoplasm can also show changes, such as vacuolization or increased basophilia (a bluish tint due to increased RNA).
Tissue Architecture
Beyond individual cell changes, dysplasia also affects the overall architecture of the tissue. In normal tissues, cells are arranged in specific layers and patterns that are essential for the tissue’s function. For instance, in epithelial tissues, cells mature and differentiate as they move from the basal layer towards the surface. In dysplastic tissues, this orderly maturation is disturbed. Cells may pile up in disorganized layers, lose their polarity (orientation), and invade surrounding tissues in a less aggressive manner than invasive cancer. This disruption in architecture is a hallmark of precancerous lesions.
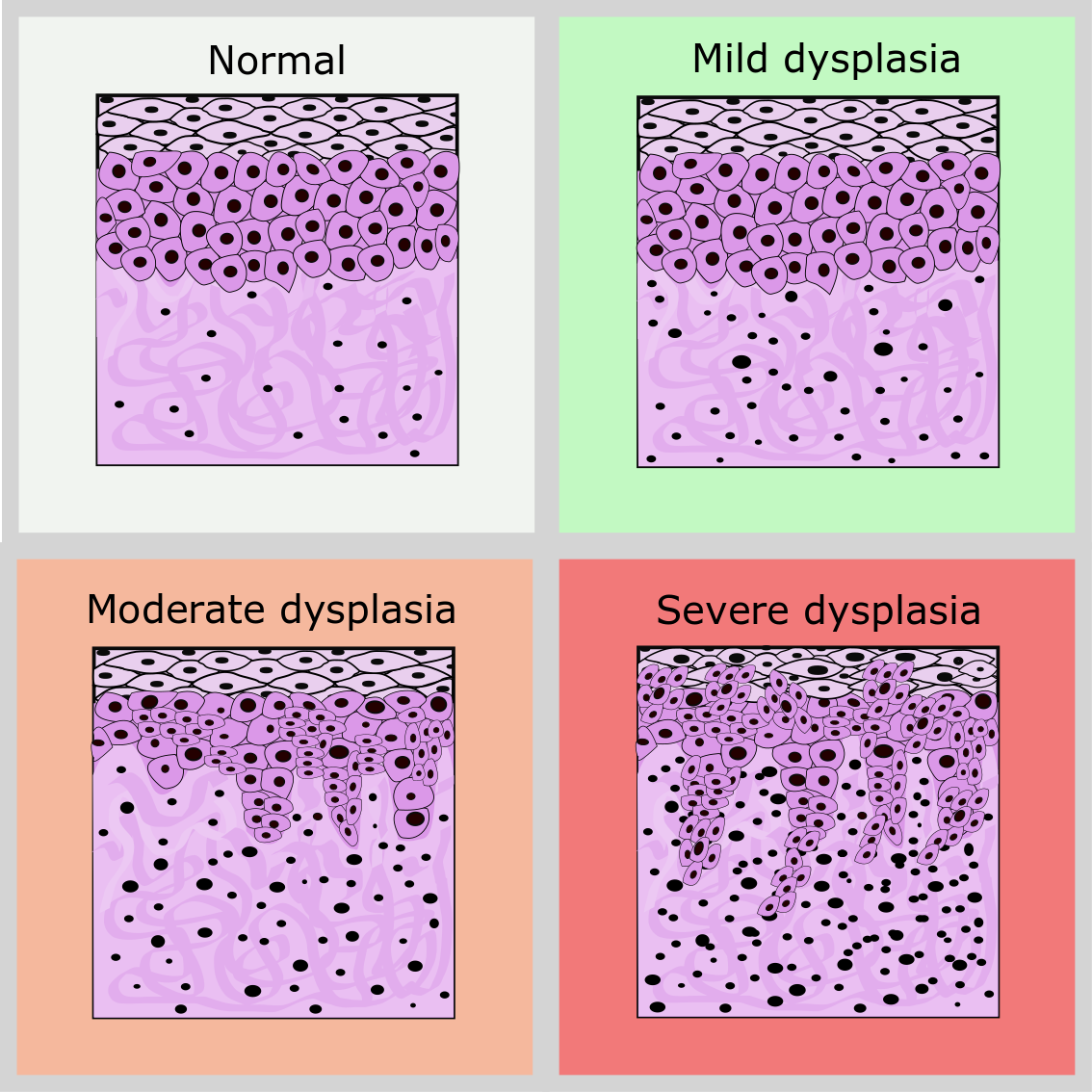
Grading of Dysplasia
The severity of dysplasia is typically graded to indicate the degree of cellular abnormality and the likelihood of progression to cancer. This grading is crucial for clinical decision-making.
Mild Dysplasia
Mild dysplasia, also known as low-grade dysplasia, is characterized by minor cellular abnormalities. The cells may show some enlargement of the nucleus and slight hyperchromasia, but the overall tissue architecture remains relatively preserved. In many cases, mild dysplasia can regress spontaneously, particularly if the causative agent is removed. However, it still warrants monitoring.
Moderate Dysplasia
Moderate dysplasia exhibits more pronounced cellular abnormalities than mild dysplasia. The nuclei are larger and more irregular, and there is a significant increase in the number of mitotic figures. The orderly maturation of cells is more noticeably disrupted, affecting a larger portion of the tissue thickness. Moderate dysplasia has a higher risk of progressing to severe dysplasia or carcinoma in situ (a non-invasive form of cancer).
Severe Dysplasia
Severe dysplasia, also referred to as high-grade dysplasia, shows significant cellular atypia and architectural disarray. The cells bear little resemblance to normal cells, with markedly enlarged, hyperchromatic, and pleomorphic (variably shaped) nuclei. Mitotic figures are frequent and abnormal. In severe dysplasia, the abnormal cells occupy more than two-thirds of the epithelial thickness, and the risk of progression to invasive cancer is substantial. In some classifications, severe dysplasia is considered synonymous with carcinoma in situ, as the entire thickness of the epithelium is replaced by neoplastic cells, but without invasion into the underlying tissue.
Causes and Risk Factors
Dysplasia is often a consequence of chronic irritation or inflammation, which triggers repeated cycles of cell damage and repair. This persistent cellular stress can lead to errors in DNA replication and repair, accumulating mutations that drive the development of dysplastic changes.
Chemical Carcinogens
Exposure to various chemical carcinogens is a well-established cause of dysplasia. These include substances found in tobacco smoke (e.g., polycyclic aromatic hydrocarbons), which can cause dysplasia in the respiratory tract and oral cavity. Similarly, certain chemicals in alcohol beverages, especially when combined with smoking, can contribute to dysplasia in the esophagus and upper digestive tract.
Infectious Agents
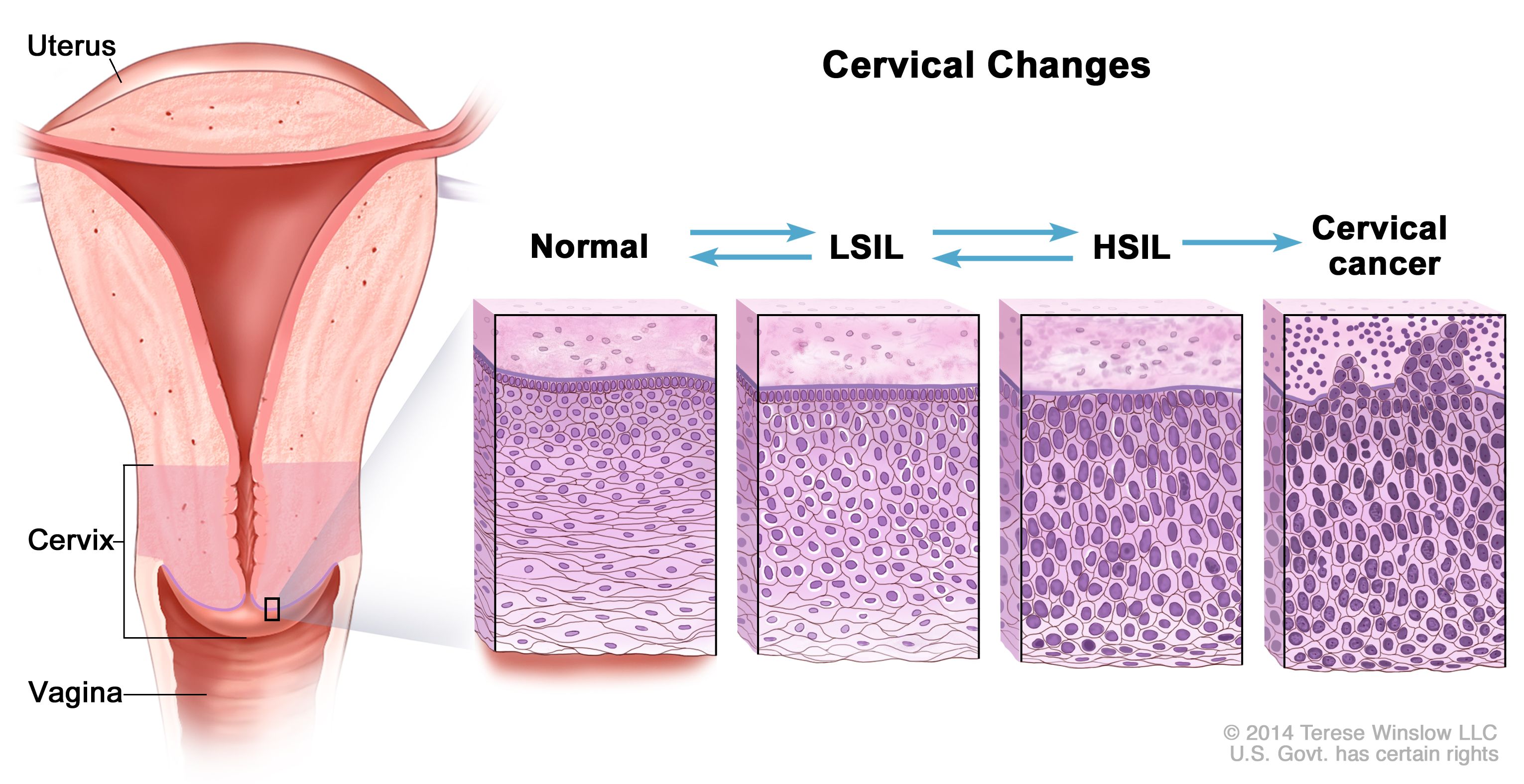
Certain viral infections are also strongly linked to dysplasia. The human papillomavirus (HPV) is a prime example, particularly high-risk strains that can cause dysplasia in the cervix, anus, penis, and oropharynx. HPV integrates its genetic material into host cells, disrupting cell cycle regulation and promoting the development of precancerous lesions. Hepatitis B and C viruses can lead to chronic inflammation of the liver, increasing the risk of hepatic dysplasia and hepatocellular carcinoma.
Chronic Inflammation
Chronic inflammatory conditions can create an environment conducive to dysplasia. For instance, long-standing gastroesophageal reflux disease (GERD) can lead to Barrett’s esophagus, a condition where the normal squamous epithelium of the esophagus is replaced by metaplastic columnar epithelium, which can then undergo dysplastic changes and progress to esophageal adenocarcinoma. Inflammatory bowel disease (IBD), such as ulcerative colitis and Crohn’s disease, is associated with an increased risk of dysplasia and colorectal cancer due to chronic inflammation in the colon.
Hormonal Influences
Hormonal factors can also play a role in the development of dysplasia, particularly in hormone-sensitive tissues. For example, estrogen exposure has been implicated in the development of endometrial hyperplasia and dysplasia, which can precede endometrial cancer.
Genetic Predisposition
While most dysplasia is acquired, certain genetic predispositions can increase an individual’s susceptibility to developing dysplastic changes. For instance, individuals with certain inherited syndromes, like Lynch syndrome, have a higher risk of developing colorectal and other cancers due to inherited mutations in DNA mismatch repair genes, which can lead to a higher accumulation of mutations and an increased likelihood of dysplasia.
Diagnostic Approaches and Technologies

The accurate diagnosis of dysplasia is paramount for effective patient management. This relies on a combination of clinical assessment, imaging techniques, and histopathological examination. The advent of advanced imaging and analytical technologies is continuously improving the precision and efficiency of dysplasia detection.
Histopathology
The gold standard for diagnosing dysplasia remains the microscopic examination of tissue biopsies by a pathologist. This involves obtaining a tissue sample from the area of concern and processing it to create thin sections that can be viewed under a microscope. The pathologist meticulously examines the cellular morphology, nuclear features, and tissue architecture, grading the dysplasia as mild, moderate, or severe. This detailed analysis provides definitive diagnostic information.
Cytology
Cytology involves the examination of individual cells or small clusters of cells, often obtained through non-invasive or minimally invasive methods such as scrapings, brushings, or fine-needle aspirations. The Papanicolaou (Pap) smear, used for cervical cancer screening, is a classic example of a cytological test that detects dysplastic cells in the cervix. While cytology can be highly effective for screening, it is generally less definitive than histopathology for grading dysplasia, as it lacks the architectural context of tissue.
Imaging Modalities
Various imaging techniques play a crucial role in identifying suspicious areas that may harbor dysplasia, guiding biopsies, and monitoring treatment response.
Endoscopy and Colposcopy
Endoscopic procedures, such as esophagogastroduodenoscopy (EGD) for the upper gastrointestinal tract, colonoscopy for the lower gastrointestinal tract, and bronchoscopy for the airways, allow direct visualization of internal organs. Specialized instruments can be used to magnify the view and identify abnormal-looking areas indicative of dysplasia. Colposcopy is a procedure used to examine the cervix, vagina, and vulva, often employing magnification and special dyes to highlight dysplastic lesions.
Optical Coherence Tomography (OCT)
OCT is a non-invasive imaging technique that uses light waves to create cross-sectional images of biological tissues. In the context of dysplasia, OCT can provide high-resolution, real-time imaging of tissue microstructure, allowing for the detection of subtle architectural changes and cellular abnormalities that might be missed by the naked eye. This technology is particularly promising for evaluating dysplasia in the esophagus, airways, and skin.
Advanced Microscopy Techniques
Beyond traditional light microscopy, advanced techniques are enhancing diagnostic capabilities. Confocal microscopy allows for optical sectioning of tissues, providing detailed three-dimensional images of cellular structures without physical sectioning. Digital pathology, which involves scanning glass slides to create high-resolution digital images, facilitates remote consultation, quantitative analysis of cellular features, and the application of artificial intelligence algorithms for improved diagnostic accuracy and efficiency in identifying dysplastic cells.
Biomarker Analysis
Research is ongoing to identify specific molecular biomarkers that can indicate the presence and grade of dysplasia. These biomarkers, which can be proteins, nucleic acids, or metabolites, are often overexpressed or altered in dysplastic cells. Detecting these biomarkers in tissue samples or bodily fluids could lead to less invasive diagnostic methods and more personalized treatment strategies. For example, detection of specific DNA mutations or methylation patterns associated with cancer development can aid in risk stratification for patients with known dysplasia.
Clinical Implications and Management
The clinical implications of a dysplasia diagnosis are significant, necessitating careful management strategies tailored to the grade of dysplasia, its location, and the individual patient’s risk factors. The primary goal is to prevent progression to invasive cancer.
Surveillance and Monitoring
For low-grade dysplasia, especially in certain locations like the esophagus (Barrett’s esophagus) or cervix, regular surveillance is often recommended. This involves periodic endoscopic examinations or colposcopies with biopsies to monitor for any progression in the severity of dysplasia or the development of cancer. The frequency of surveillance depends on the specific condition and individual risk factors.
Treatment Modalities
The treatment approach for dysplasia depends on its grade and location.
Local Excision or Ablation
For high-grade dysplasia or dysplasia that shows no signs of regression, local treatment is often employed. This can involve surgical excision of the affected tissue or ablative therapies. For instance, endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) can be used to remove dysplastic lesions in the gastrointestinal tract. Radiofrequency ablation (RFA) is a common treatment for Barrett’s esophagus with high-grade dysplasia, using heat to destroy the abnormal cells. Cryotherapy, which uses extreme cold, can also be used for ablation.
Medical Therapy
In some cases, particularly for mild dysplasia related to reversible causes, medical management might be considered. This could involve treating underlying conditions like GERD or stopping exposure to irritants such as smoking or alcohol. While medical therapy alone is rarely sufficient for significant dysplasia, it plays a crucial role in managing causative factors.
Prophylactic Surgery
In specific high-risk situations, where the likelihood of progression to cancer is exceptionally high and less invasive treatments are not feasible or have failed, prophylactic surgery to remove the affected organ or tissue may be considered. This is a more aggressive approach and is typically reserved for advanced stages of dysplasia or in individuals with strong genetic predispositions and multiple risk factors.
Patient Education and Lifestyle Modifications
Patient education is a vital component of managing dysplasia. Understanding the precancerous nature of the condition and the importance of adherence to surveillance and treatment plans empowers patients to actively participate in their healthcare. Lifestyle modifications, such as quitting smoking, reducing alcohol consumption, adopting a healthy diet, and managing chronic inflammatory conditions, are often recommended to minimize further cellular damage and promote a healthier cellular environment. The goal is to create an environment that discourages the progression of cellular abnormalities and supports cellular repair and regeneration.