Understanding Spontaneous Pneumothorax
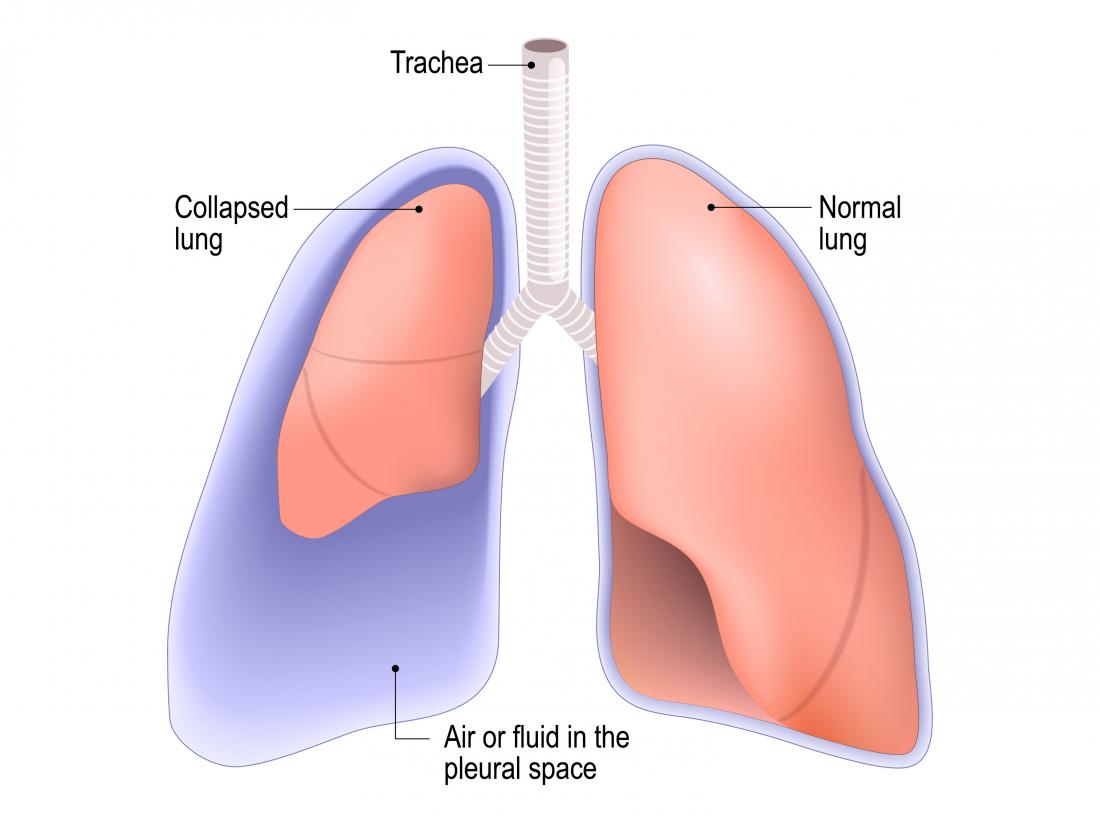
A collapsed lung, medically known as pneumothorax, is a serious condition where air accumulates in the pleural space, the thin gap between the lung and the chest wall. This accumulation of air exerts pressure on the lung, causing it to partially or completely deflate. While often associated with trauma, a spontaneous pneumothorax can occur without any apparent injury, a phenomenon that can be particularly unsettling and requires careful understanding of its mechanisms and implications. This condition disrupts the delicate balance of pressures that allow our lungs to expand and contract with each breath, leading to potentially severe respiratory distress.
Primary Spontaneous Pneumothorax (PSP)
Primary spontaneous pneumothorax (PSP) is the type that occurs in individuals with no underlying lung disease. It is most common in young, tall, and thin men, typically between the ages of 10 and 30. The exact cause of PSP is not fully understood, but it is believed to be related to the rupture of small air sacs within the lung called blebs or bullae. These are typically located at the apex of the lung. When these blebs rupture, air escapes from the lung into the pleural space. The presence of these blebs is thought to be a congenital predisposition in some individuals, making them more susceptible to this type of collapse. Factors such as smoking and rapid changes in atmospheric pressure may also play a role in precipitating the rupture. While often occurring without warning, some individuals might experience mild chest discomfort or shortness of breath for a few days prior to a significant event.
Secondary Spontaneous Pneumothorax (SSP)
Secondary spontaneous pneumothorax (SSP) is more concerning as it arises as a complication of an existing lung disease. Conditions such as Chronic Obstructive Pulmonary Disease (COPD), asthma, cystic fibrosis, lung cancer, and infections like tuberculosis are common culprits. In these cases, the underlying lung tissue is already damaged or weakened, making it more prone to rupture. The air sacs within these diseased lungs are often larger and more fragile, increasing the likelihood of a bleb or bulla forming and subsequently bursting. SSP can occur at any age but is more prevalent in older adults. The symptoms of SSP are often more severe than PSP because the underlying lung disease already compromises respiratory function. Patients with SSP may experience more significant shortness of breath, chest pain, and may have a higher risk of developing a tension pneumothorax.
The Mechanics of Lung Collapse
The respiratory system is a finely tuned mechanism that relies on precise pressure gradients to function. The lungs themselves are not muscular organs; they are elastic structures that expand and contract passively in response to changes in the volume of the chest cavity. This process is driven by the diaphragm and the intercostal muscles, which alter the pressure within the chest. The pleural space, a potential space containing a small amount of lubricating fluid, plays a crucial role in this mechanism.
Pleural Pressure and Lung Function
Normally, the pressure within the pleural space (intrapleural pressure) is always negative relative to the atmospheric pressure. This negative pressure acts like a gentle suction, keeping the lungs expanded and adhered to the chest wall. During inhalation, the diaphragm contracts and moves downward, and the intercostal muscles lift the rib cage upward and outward. These actions increase the volume of the thoracic cavity, causing the intrapleural pressure to become even more negative. This negative pressure then pulls the lungs outward, causing them to expand and draw air in. During exhalation, these muscles relax, the chest cavity volume decreases, and the lungs recoil passively, pushing air out.
Air Entry into the Pleural Space
When a bleb or bulla ruptures, or when the chest wall is breached by trauma, air from within the lung or from the external environment enters the pleural space. As air fills this space, it disrupts the negative intrapleural pressure. The increased pressure in the pleural space pushes against the lung tissue, causing it to collapse. The extent of the collapse depends on the amount of air that enters and the duration of the leak. If the air leak is significant and continues to enter the pleural space without an exit, it can lead to a life-threatening condition called a tension pneumothorax.
Symptoms and Diagnosis
Recognizing the symptoms of a collapsed lung is crucial for seeking timely medical attention. The presentation can vary depending on the size of the pneumothorax and the underlying health of the individual.
Common Symptoms
The hallmark symptom of a pneumothorax is sudden, sharp chest pain, often described as pleuritic, meaning it worsens with breathing or coughing. Shortness of breath (dyspnea) is another common and significant symptom. The severity of breathlessness can range from mild discomfort to severe respiratory distress, especially in cases of larger pneumothoraces or in individuals with pre-existing lung conditions. Other symptoms may include a rapid heart rate (tachycardia), a dry cough, and a feeling of tightness in the chest. In some instances, particularly with smaller pneumothoraces, symptoms might be mild and even go unnoticed initially.
Diagnostic Tools
A physician will typically begin by taking a thorough medical history and performing a physical examination. During the physical exam, they may notice decreased breath sounds on the affected side of the chest, and the chest wall may appear less mobile. Percussion of the chest might reveal a hyperresonant sound, indicating the presence of air. To confirm the diagnosis and assess the severity, imaging studies are essential.
Chest X-ray
A standard chest X-ray (radiograph) is usually the first line of investigation. It can clearly visualize the pleural space and the lung margins. In a patient with pneumothorax, the X-ray will show a visible line representing the visceral pleura (the membrane covering the lung) separated from the parietal pleura (the membrane lining the chest wall) by a dark space filled with air. The lung on the affected side will appear smaller than normal.

Computed Tomography (CT) Scan
In some cases, a CT scan may be ordered, especially if the diagnosis is uncertain from a chest X-ray or if the clinician suspects an underlying lung abnormality contributing to the pneumothorax, such as blebs or bullae. A CT scan provides more detailed cross-sectional images of the lungs and can help identify the cause and extent of the lung collapse with greater precision.
Treatment and Management
The management of a collapsed lung depends on the size of the pneumothorax, the severity of symptoms, and the presence of any underlying lung disease. The goal of treatment is to remove the air from the pleural space, allowing the lung to re-expand and restore normal breathing function.
Observation and Oxygen Therapy
For small, asymptomatic, or minimally symptomatic pneumothoraces in otherwise healthy individuals, observation may be the initial approach. This involves close monitoring of the patient’s vital signs and oxygen saturation. Supplemental oxygen is often administered, as it can help accelerate the reabsorption of air from the pleural space into the bloodstream. The body’s natural processes can sometimes resolve small pneumothoraces over a period of days without invasive intervention.
Needle Aspiration
If a pneumothorax is larger or causing more significant symptoms but not yet considered a medical emergency requiring a chest tube, needle aspiration may be considered. This minimally invasive procedure involves inserting a needle or small catheter into the pleural space to withdraw the accumulated air. This can provide immediate relief of symptoms by allowing the lung to re-expand. It is a less invasive option than a chest tube but may be less effective for persistent air leaks.
Chest Tube (Thoracostomy) Insertion
For larger pneumothoraces, significant air leaks, or tension pneumothorax, the insertion of a chest tube (also known as a chest drain or thoracostomy tube) is the standard treatment. This procedure involves making a small incision in the chest wall and inserting a flexible tube into the pleural space. The tube is then connected to a sealed drainage system, which typically includes a water seal and sometimes suction. The water seal prevents air from re-entering the pleural space, while suction helps to actively remove air and fluid, encouraging the lung to re-expand. The chest tube is usually left in place until the air leak has stopped and the lung has fully re-inflated, which can take several days.
Surgical Interventions
In recurrent cases of pneumothorax or when conservative measures fail, surgical intervention may be necessary.
Pleurodesis
Pleurodesis is a procedure designed to prevent future lung collapses. It involves creating inflammation or scarring within the pleural space, which causes the visceral and parietal pleura to adhere to each other. This adhesion obliterates the pleural space, making it impossible for air to accumulate and cause a collapse. Pleurodesis can be performed surgically (mechanical pleurodesis) or chemically (chemical pleurodesis) by instilling an irritant solution into the pleural space.
Bullectomy
If the pneumothorax is caused by a large bleb or bulla, surgical removal of this abnormal air sac, known as a bullectomy, may be performed. This procedure is often done via video-assisted thoracoscopic surgery (VATS), a minimally invasive technique. By removing the source of the air leak, the likelihood of future collapses is significantly reduced.
Recovery and Prevention
The recovery period following a pneumothorax varies depending on the treatment received and the individual’s overall health. Following medical advice and making lifestyle adjustments can play a significant role in preventing recurrence.
Post-Treatment Recovery
After treatment, patients are typically advised to avoid strenuous activity for several weeks to allow the lung and chest wall to heal properly. Pain management is important during the recovery phase. Follow-up appointments with a healthcare provider are crucial to monitor lung function and check for any signs of recurrence. It is imperative to be aware of any returning symptoms, such as increased chest pain or shortness of breath, and to seek immediate medical attention if they occur.

Lifestyle Modifications and Recurrence
Smoking is a significant risk factor for both primary and secondary spontaneous pneumothorax and significantly increases the risk of recurrence. Therefore, quitting smoking is the most important preventative measure. Individuals who have experienced a pneumothorax are at a higher risk of it happening again, particularly those with underlying lung conditions. Avoiding activities that involve rapid pressure changes, such as scuba diving, may also be recommended. Understanding personal risk factors and discussing them with a healthcare professional is key to developing a personalized prevention strategy. Regular medical check-ups can help monitor lung health and detect any early signs of potential issues.