Herpangina, a term that often elicits curiosity and sometimes concern, refers to a specific viral illness that primarily affects infants and young children. While it might sound like a complex medical condition, understanding its origins, symptoms, and management is crucial for parents and caregivers. This article delves into the nuances of herpangina, exploring its viral culprits, the characteristic manifestations, and the approaches to alleviating discomfort and promoting recovery.
The Viral Origins of Herpangina
Herpangina is not caused by a single pathogen but rather a group of viruses belonging to the enterovirus family. These viruses are highly contagious and thrive in environments where close contact is common, such as daycare centers, schools, and households.

Enteroviruses: The Primary Culprits
The most frequent cause of herpangina is the coxsackievirus, particularly the A group strains (such as coxsackievirus A1, A2, A4, A5, A6, A8, A10, A16, and B strains). Other enteroviruses, including echoviruses and even the poliovirus (though less common due to widespread vaccination), can also be implicated.
Coxsackievirus A Strains
These small, RNA viruses are ubiquitous and are shed in the stool and respiratory secretions of infected individuals. Their ability to survive on surfaces for extended periods contributes to their easy transmission through direct contact or by touching contaminated objects and then touching the mouth.
Echoviruses and Other Enteroviruses
While coxsackieviruses are the most common culprits, echoviruses and other enteroviruses can also lead to the development of herpangina. The clinical presentation is often indistinguishable, with the specific viral strain identified through laboratory testing if necessary.
Transmission Pathways
Understanding how herpangina spreads is key to prevention. The primary modes of transmission include:
Fecal-Oral Route
This is the most common route. The virus is present in the stool of infected individuals and can spread when hands are not washed thoroughly after using the toilet or changing diapers, and then come into contact with the mouth. Contaminated food, water, or surfaces can also serve as vehicles.
Respiratory Droplets
Infected individuals can expel the virus in respiratory droplets when coughing or sneezing. Inhaling these droplets can lead to infection. Close contact, such as sharing utensils or kissing, can facilitate this type of transmission.
Direct Contact
Touching an infected person’s blisters or sores can also transmit the virus. This highlights the importance of hygiene when dealing with a child who has herpangina.
Manifestations of Herpangina: Symptoms and Signs
Herpangina is characterized by a sudden onset of fever and the development of small, painful blisters or sores in the back of the throat. The appearance and location of these lesions are defining features of the illness.
The Prodromal Phase
Before the characteristic sores appear, children may experience a brief period of non-specific symptoms, often referred to as the prodromal phase. This can include:
Sudden Fever
A rapid increase in body temperature, often reaching 101-104°F (38.3-40°C), is a common initial symptom. This fever can sometimes be accompanied by chills.
General Malaise
Children may appear generally unwell, exhibiting irritability, lethargy, or a lack of interest in their usual activities. This feeling of discomfort can precede the more specific symptoms.
Sore Throat
A general soreness or scratchiness in the throat might be an early indicator, though the severe pain typically associated with the sores develops later.
The Characteristic Lesions
The hallmark of herpangina is the appearance of distinctive sores, typically located in the posterior part of the mouth.
Location of the Sores
The lesions are predominantly found on the soft palate, uvula, tonsils, and the sides or back of the throat. They are rarely found on the front of the mouth, gums, or tongue, which helps differentiate herpangina from other oral conditions like hand, foot, and mouth disease (which can be caused by similar viruses but presents with lesions in different locations).
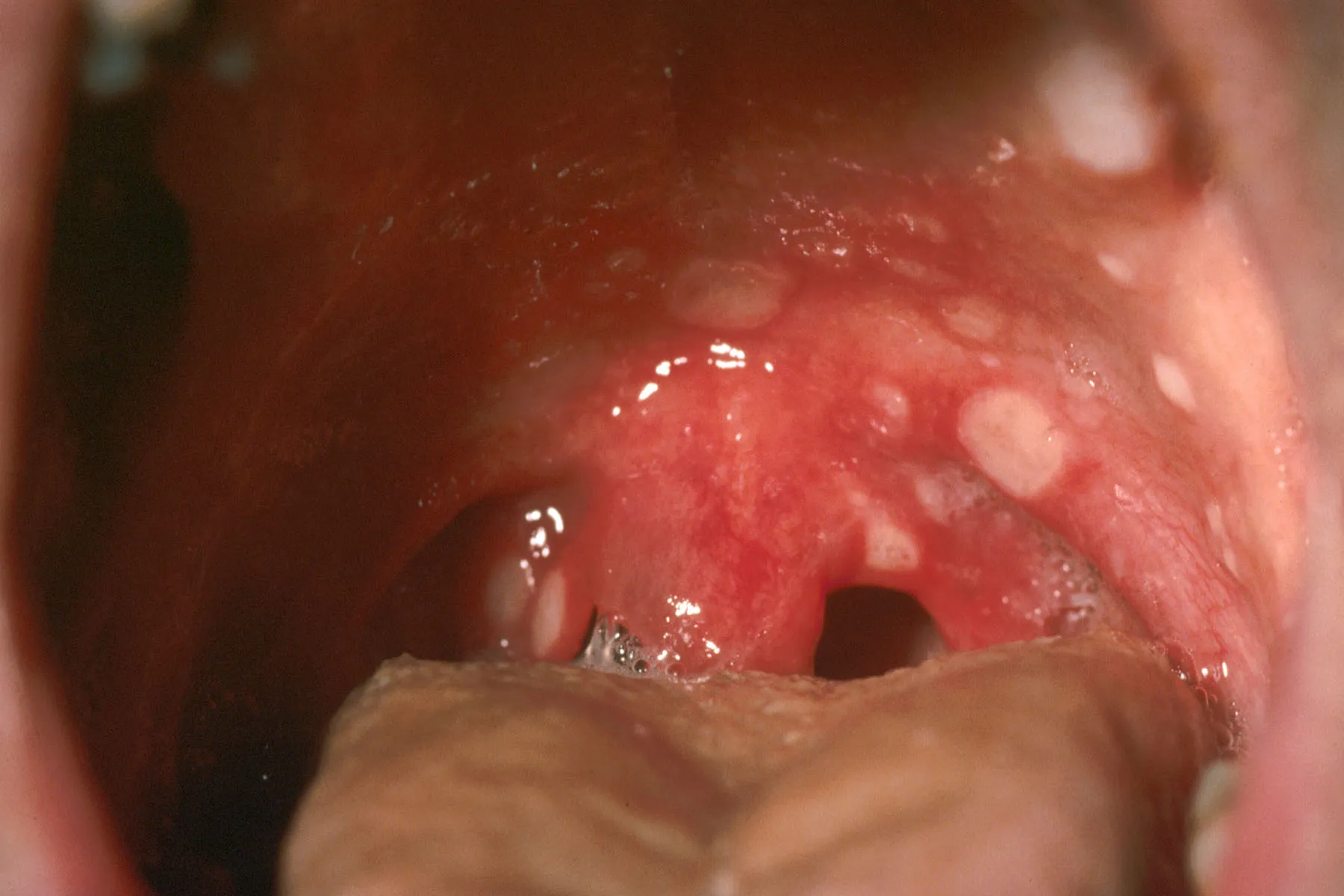
Appearance of the Sores
Initially, the sores begin as small, reddish papules (raised bumps). These quickly develop into vesicles (fluid-filled blisters), which are typically 1-5 millimeters in diameter. Within a day or two, these vesicles rupture, leaving behind small, shallow ulcers that are covered with a grayish-white exudate and surrounded by a red border. These ulcers are exquisitely painful.
Number and Progression
The number of lesions can vary from a few to over a dozen. They tend to appear in crops, meaning new sores can develop as older ones begin to heal. The entire process of lesion development and healing usually spans about a week.
Associated Symptoms
Beyond the fever and oral sores, other symptoms can accompany herpangina, contributing to the child’s discomfort.
Difficulty Swallowing (Odynophagia)
The intense pain from the ulcers makes swallowing extremely difficult and painful. This can lead to dehydration and a reluctance to eat or drink.
Drooling
Younger children, unable to swallow effectively due to the pain, may drool excessively.
Loss of Appetite
Discomfort during eating naturally leads to a reduced appetite.
Headache and Muscle Aches
Some children may complain of headaches or experience general muscle aches, consistent with a viral illness.
Vomiting and Abdominal Pain
In some cases, especially with certain enterovirus strains, vomiting or abdominal discomfort may also occur.
Diagnosis and Management of Herpangina
Diagnosing herpangina is typically based on a physical examination and the characteristic presentation of symptoms. While specific laboratory tests can confirm the viral strain, they are rarely necessary for routine management. The focus of care is on alleviating symptoms and preventing complications.
Clinical Diagnosis
Physicians often diagnose herpangina based on:
Medical History
Gathering information about the onset of fever, sore throat, and any other reported symptoms.
Physical Examination
A thorough examination of the child’s mouth and throat to identify the characteristic lesions. The location and appearance of the sores are key diagnostic indicators.
When to Seek Medical Attention
While herpangina is generally a self-limiting illness, it is important to consult a healthcare provider if:
Severe Dehydration is Suspected
If the child is refusing to drink fluids for an extended period, showing signs of decreased urination (dry diapers), sunken eyes, or listlessness.
High Fever Persists
If the fever is very high and does not respond to fever-reducing medications, or if it persists for more than 3-4 days.
Symptoms Worsen
If the child appears to be getting sicker, develops a stiff neck, or shows signs of significant distress.
Other Underlying Conditions are Suspected
If there is any doubt about the diagnosis or if the child has other health issues.
Treatment and Symptom Relief
There is no specific antiviral medication for herpangina. Treatment is primarily supportive, aimed at managing pain, fever, and preventing dehydration.
Pain and Fever Management
- Acetaminophen or Ibuprofen: These over-the-counter medications are effective in reducing fever and relieving pain. It is crucial to use the correct dosage based on the child’s weight and age. Aspirin should generally be avoided in children due to the risk of Reye’s syndrome.
- Topical Anesthetics: For older children who can tolerate it, a topical anesthetic mouthwash or spray might offer temporary relief from the pain of the sores. However, these should be used cautiously and under the guidance of a healthcare provider.
Hydration
Maintaining adequate fluid intake is paramount.
- Offer Fluids Frequently: Provide small, frequent sips of cool liquids. Good options include water, milk, diluted juice, or oral rehydration solutions.
- Avoid Irritating Foods: Steer clear of acidic, spicy, or salty foods and drinks that can further irritate the sores.
- Soft and Cold Foods: Offer soft, bland foods that are easy to swallow, such as yogurt, applesauce, pudding, or smoothies. Cold foods, like popsicles or ice cream (sugar-free options are preferred to avoid dental issues), can also be soothing.
Preventing Spread
Good hygiene practices are essential to prevent the spread of the virus to others.
- Handwashing: Frequent and thorough handwashing with soap and water is the most effective way to prevent transmission. This should be done after changing diapers, using the toilet, and before preparing food.
- Disinfection: Regularly disinfect frequently touched surfaces, toys, and changing areas.
- Isolation: While not always practical, keeping the infected child away from other children, especially infants and those with compromised immune systems, can help limit spread.
Prognosis and Complications
Herpangina is typically a mild illness with a favorable prognosis, meaning most children recover fully without long-term issues. However, in rare instances, complications can arise.
Recovery Timeline
The duration of herpangina is generally short.
Resolution of Symptoms
Fever usually subsides within 2-3 days. The oral sores typically begin to heal within a week, although complete resolution can take up to 10-14 days. The most intense discomfort usually lasts for the first few days of the illness.
Immunity
While infection with one strain of enterovirus may confer immunity to that specific strain, it does not protect against other strains. Therefore, it is possible for an individual to experience herpangina more than once in their lifetime if infected by different enteroviruses.
Potential Complications
Although uncommon, herpangina can occasionally lead to more serious issues, particularly if the underlying viral infection is severe or if dehydration is significant.
Dehydration
This is the most common complication, arising from the inability to swallow due to pain. Severe dehydration can require hospitalization and intravenous fluid administration.
Viral Meningitis or Encephalitis
In very rare cases, enteroviruses can spread to the central nervous system, leading to aseptic meningitis (inflammation of the membranes surrounding the brain and spinal cord) or encephalitis (inflammation of the brain itself). These are serious conditions requiring immediate medical attention.
Other Systemic Infections
Certain enteroviruses have the potential to cause more widespread infections, affecting other organs. However, this is extremely rare in otherwise healthy children.
Differentiating from Other Conditions
It is important for healthcare providers to differentiate herpangina from other conditions that can cause oral lesions in children, such as:
- Hand, Foot, and Mouth Disease (HFMD): While caused by similar viruses (often coxsackievirus A16 or enterovirus 71), HFMD typically presents with a rash on the hands, feet, and sometimes buttocks, in addition to oral sores. The oral sores in HFMD can be more widespread and may involve the front of the mouth and tongue.
- Aphthous Ulcers (Canker Sores): These are common in children and adults but are typically not associated with fever or the widespread, rapidly appearing lesions characteristic of herpangina. They also tend to occur more on the front of the mouth.
- Herpes Simplex Virus (HSV) Infection: Primary herpetic gingivostomatitis, caused by HSV-1, can present with fever and painful sores in the mouth. However, the sores are often more diffuse, can involve the gums and lips, and may be accompanied by swollen gums.
In conclusion, herpangina is a common childhood viral illness characterized by fever and painful sores in the back of the throat. While it can be distressing for both children and parents, understanding its causes, symptoms, and management strategies allows for effective care, ensuring a swift and comfortable recovery. Maintaining good hygiene remains the cornerstone of preventing its spread.