Diver’s bends, medically known as decompression sickness (DCS), is a serious and potentially life-threatening condition that can affect divers. It arises from the rapid ascent from depth during a dive, leading to the formation of nitrogen bubbles within the body’s tissues and bloodstream. Understanding the physiological mechanisms behind DCS, its symptoms, causes, and effective prevention and treatment strategies is crucial for any recreational or professional diver. This condition underscores the importance of adhering to dive tables, dive computers, and proper safety protocols to ensure a safe return to the surface.
The Physiology of Decompression Sickness
The core of diver’s bends lies in the behavior of gases under pressure. When a diver descends into water, the surrounding water pressure increases. This increased pressure forces more atmospheric gases, primarily nitrogen, to dissolve into the diver’s bloodstream and tissues. The deeper the dive and the longer the bottom time, the greater the amount of nitrogen that becomes absorbed. This process is governed by Henry’s Law, which states that the amount of gas dissolved in a liquid is directly proportional to the partial pressure of that gas above the liquid.
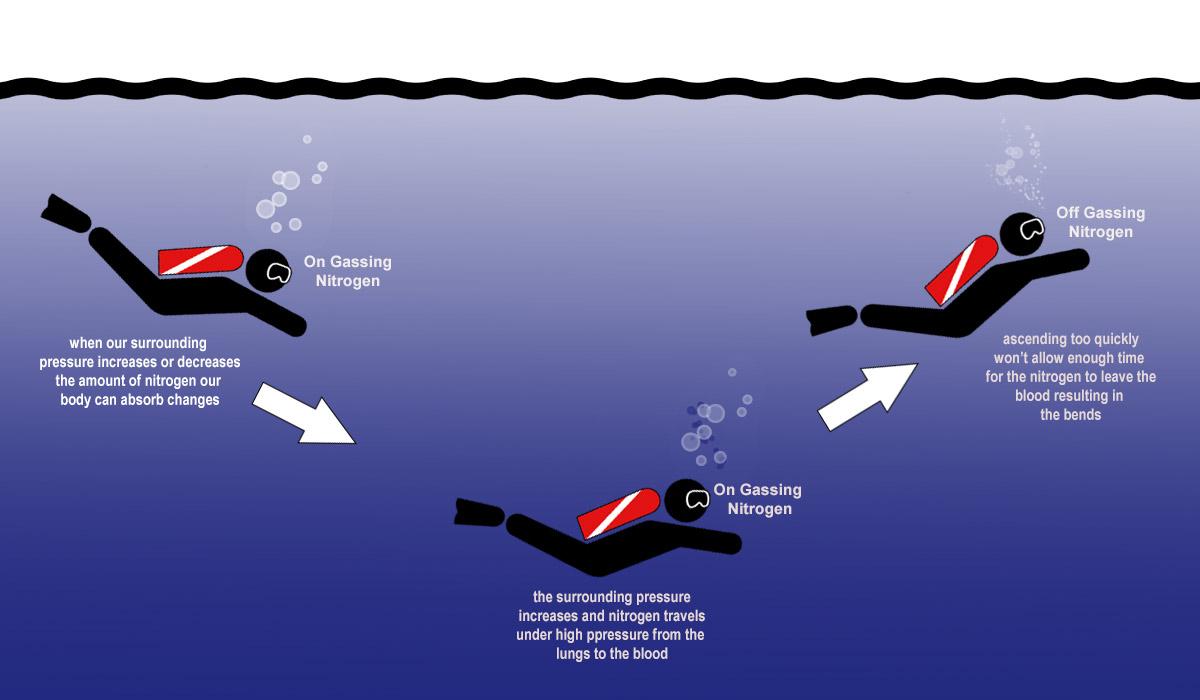
During the descent and while at depth, the diver’s body gradually saturates with nitrogen. This dissolved nitrogen is generally harmless as long as the diver remains at depth or ascends slowly and controlled. The slow ascent allows the body to gradually off-gas the excess nitrogen through respiration. The lungs act as the primary excretory organ for nitrogen during ascent.
However, if a diver ascends too rapidly, the surrounding pressure decreases abruptly. This sudden drop in pressure causes the dissolved nitrogen to come out of solution and form tiny bubbles within the blood vessels and tissues, much like the bubbles that form when opening a carbonated beverage. These bubbles can obstruct blood flow, irritate tissues, and trigger inflammatory responses, leading to the diverse range of symptoms associated with DCS. The rate at which nitrogen comes out of solution is critical, and rapid decompression bypasses the body’s natural off-gassing mechanisms.
Nitrogen Uptake and Off-gassing
The uptake of nitrogen into bodily tissues is a gradual process. Different tissues have varying blood flow rates and therefore absorb nitrogen at different speeds. Highly vascularized tissues like the brain, heart, and kidneys absorb nitrogen quickly, while less vascularized tissues such as bone and fat absorb it more slowly. Conversely, off-gassing also follows similar patterns, with highly perfused tissues releasing nitrogen more readily than poorly perfused ones.
Dive tables and dive computers are designed to calculate safe ascent profiles based on these physiological principles. They provide recommended no-decompression limits (NDLs) for specific depths, which are the maximum time a diver can stay at that depth without requiring mandatory decompression stops. For dives exceeding these limits, divers must perform staged ascents, pausing at specific depths for predetermined periods to allow for controlled off-gassing of nitrogen. These stops are known as decompression stops and are critical for preventing bubble formation.
Bubble Formation and Its Consequences
The formation of nitrogen bubbles is the direct cause of DCS symptoms. These bubbles can form in various locations within the body:
- Intravascular bubbles: These bubbles form within blood vessels, potentially blocking blood flow to vital organs and tissues. This can lead to a range of symptoms depending on the location of the blockage, from mild joint pain to severe neurological deficits.
- Extravascular bubbles: These bubbles form in tissues outside of blood vessels. While they may not directly obstruct blood flow, they can cause local irritation, inflammation, and pain.
The size and distribution of these bubbles significantly influence the severity and type of symptoms experienced. Smaller bubbles might cause mild discomfort, while larger or more numerous bubbles can lead to catastrophic blockages and severe systemic effects.
Symptoms of Diver’s Bends
The symptoms of diver’s bends can vary widely in their onset, severity, and presentation. They can appear immediately after surfacing, within minutes, or even hours after a dive. Some divers may experience only mild discomfort, while others suffer debilitating and life-threatening consequences. The symptoms are often categorized based on the affected body system.
Mild to Moderate Symptoms (Type I DCS)
These are the most common manifestations of DCS and are generally less severe.
- Joint Pain (the “bends”): This is the classic symptom and can range from a dull ache to sharp, intense pain, typically in the shoulders, elbows, or knees. The pain can be localized to a specific joint or spread across a limb. It is often exacerbated by movement.
- Skin Manifestations: These can include itching, a rash, or a mottled appearance of the skin (cutis marmorata). These symptoms are often indicative of bubbles forming in the small blood vessels of the skin.
- Fatigue and Malaise: A general feeling of extreme tiredness, weakness, and disorientation can occur.

Severe Symptoms (Type II DCS)
These symptoms indicate involvement of the central nervous system, respiratory system, or cardiovascular system and are considered medical emergencies.
- Neurological Symptoms: This is the most concerning category of DCS symptoms.
- Dizziness and Vertigo: A spinning sensation or loss of balance.
- Headache: Severe and persistent headaches.
- Visual Disturbances: Blurred vision, double vision, or temporary blindness.
- Numbness and Tingling: Sensory disturbances, often described as pins and needles.
- Weakness or Paralysis: Loss of motor function, which can affect limbs or even breathing muscles.
- Cognitive Impairment: Confusion, disorientation, memory loss, or difficulty concentrating.
- Seizures: Uncontrolled electrical activity in the brain.
- Respiratory Symptoms (“The Chokes”):
- Coughing: A persistent and often dry cough.
- Shortness of Breath: Difficulty breathing, especially on exertion.
- Chest Pain: Discomfort or pain in the chest.
These symptoms are caused by bubbles obstructing blood flow in the pulmonary circulation.
- Cardiovascular Symptoms:
- Shock: A life-threatening condition characterized by low blood pressure, rapid pulse, and cool, clammy skin.
- Cardiac Arrest: In very severe cases, bubble formation can lead to heart failure.
It is important to note that the absence of mild symptoms does not preclude the possibility of severe DCS. Even if a diver feels fine after a dive, they should remain vigilant for any developing symptoms.
Risk Factors and Prevention
Understanding the factors that increase the risk of diver’s bends and implementing robust prevention strategies are paramount for diver safety. While improper ascent rates are the primary culprit, several other factors can contribute to the likelihood of developing DCS.
Contributing Factors
- Ascent Rate: As discussed, rapid ascent is the most significant risk factor. Exceeding recommended ascent speeds allows for insufficient off-gassing.
- Dive Profile: Deeper dives and longer bottom times increase the amount of dissolved nitrogen, thus raising the risk. Repeated dives within a 24-hour period, especially without adequate surface intervals, also elevate risk.
- Dehydration: Being dehydrated thickens the blood, potentially hindering circulation and making it more difficult for the body to off-gas nitrogen efficiently.
- Fatigue and Poor Physical Condition: A fatigued or unhealthy diver may be less able to cope with the physiological stresses of diving.
- Obesity: Adipose tissue (fat) is a good solvent for nitrogen. Divers with a higher body fat percentage may absorb and retain more nitrogen, leading to a slower off-gassing process.
- Cold Water: Cold can cause peripheral vasoconstriction, reducing blood flow to extremities and potentially slowing off-gassing in those areas.
- Altitude Exposure Post-Dive: Flying in an unpressurized aircraft or traveling to higher altitudes too soon after diving can significantly increase DCS risk due to the further reduction in ambient pressure.
- Alcohol and Certain Medications: Alcohol can contribute to dehydration and impaired judgment, while some medications might affect gas exchange or circulation.
- Pre-existing Medical Conditions: Certain medical conditions, such as patent foramen ovale (PFO), a small hole between the atria of the heart, can allow venous bubbles to bypass the lungs and enter the arterial circulation, increasing the risk of neurological DCS.
Prevention Strategies
The cornerstone of DCS prevention is adherence to established diving practices and guidelines.
- Follow Dive Tables and Dive Computers: Always plan dives according to reputable dive tables or use a dive computer that tracks nitrogen loading and provides ascent recommendations. Never exceed the no-decompression limits without planning for required decompression stops.
- Slow and Controlled Ascents: Ascend at a slow, controlled rate. Most dive tables and computers recommend ascent rates of 30 feet per minute (9-10 meters per minute) or slower.
- Perform Safety Stops: Even on dives well within no-decompression limits, performing a safety stop of 3-5 minutes at 15-20 feet (5-6 meters) is highly recommended. This allows for an additional period of off-gassing.
- Adequate Surface Intervals: Allow sufficient surface intervals between dives to allow the body to off-gas accumulated nitrogen.
- Stay Hydrated: Drink plenty of water before, during, and after diving. Avoid diuretics like caffeine and alcohol.
- Maintain Good Physical Fitness: Divers should be in good general health and physical condition.
- Avoid Strenuous Activity Post-Dive: Refrain from heavy exertion immediately after a dive, as this can increase the release of dissolved gases.
- Plan for Altitude Exposure: Avoid flying or traveling to significant altitudes for at least 12-24 hours after the last dive, as per standard guidelines.
- Listen to Your Body: If you feel unwell during or after a dive, report it immediately.
Diagnosis and Treatment
Prompt recognition and appropriate treatment are critical for managing diver’s bends and minimizing long-term consequences. The diagnostic process relies heavily on the diver’s history, symptoms, and a physical examination.
Diagnosis
- Diver’s History: A detailed account of the dive profile, including depth, bottom time, ascent rate, any skipped safety stops, and surface intervals, is crucial. The timeline of symptom onset is also important.
- Symptom Assessment: A thorough evaluation of the reported symptoms, their location, and severity.
- Physical Examination: This includes a neurological examination to assess motor and sensory function, balance, and cognitive status. Vital signs are also monitored.
- Exclusion of Other Conditions: It is important to rule out other potential causes of diving-related symptoms, such as nitrogen narcosis, hypoxia, decompression sickness caused by gases other than nitrogen (e.g., helium in technical diving), ear or sinus barotrauma, and pre-existing medical conditions.

Treatment
The definitive treatment for diver’s bends is recompression therapy. This involves returning the affected individual to a pressurized environment, typically in a hyperbaric chamber.
- Recompression Therapy: The patient is placed in a hyperbaric chamber and subjected to increased atmospheric pressure. This increased pressure serves two primary functions:
- Reduces Bubble Size: According to Boyle’s Law, as pressure increases, the volume of the nitrogen bubbles decreases, making them smaller and less likely to cause obstruction.
- Facilitates Off-gassing: The increased ambient pressure, often with a high concentration of oxygen, drives the dissolved nitrogen back into solution and facilitates its elimination through respiration.
- Treatment Protocols: Specific recompression protocols, such as the U.S. Navy Treatment Table 6 or Table 7, are followed. These protocols involve staged increases in pressure and periods of breathing 100% oxygen, followed by periods of breathing air. The duration and depth of treatment vary depending on the severity and type of DCS symptoms.
- Supportive Care: While in the hyperbaric chamber and afterwards, supportive care may include:
- Oxygen Administration: Supplemental oxygen is crucial during treatment and can be beneficial even outside the chamber for mild cases.
- Fluid Resuscitation: Intravenous fluids are administered to combat dehydration and maintain circulation.
- Pain Management: Medications may be used to alleviate pain.
- Steroids and Anti-inflammatories: In some cases, corticosteroids may be prescribed to reduce inflammation.
- Neurological Management: For severe neurological symptoms, specific medical interventions may be required.
It is imperative that anyone suspecting diver’s bends seeks immediate medical attention. Delaying treatment can lead to irreversible damage and increased morbidity. Divers should be aware of the signs and symptoms and know how to respond appropriately, which includes contacting emergency medical services and informing them of the diving incident. Early recognition and prompt recompression are the keys to a successful recovery from decompression sickness.