Understanding the Landscape of Anesthesia for Total Knee Arthroplasty
Total knee replacement (TKR) is a transformative surgical procedure that significantly improves the quality of life for individuals suffering from debilitating knee osteoarthritis or other severe knee conditions. While the surgical technique itself has advanced remarkably, the perioperative pain management remains a critical component for successful recovery and patient satisfaction. Effective pain control not only alleviates discomfort but also facilitates early mobilization, reduces the risk of complications such as deep vein thrombosis and pulmonary embolism, and contributes to a smoother rehabilitation process. Among the various strategies employed for pain management, regional anesthesia, specifically nerve blocks, has emerged as a cornerstone in the multimodal approach to pain relief after TKR.
The concept of using regional anesthesia to target specific nerves that innervate the knee joint has gained considerable traction due to its potential to provide superior analgesia compared to traditional systemic pain management. By selectively blocking pain signals from the surgical site, nerve blocks can offer profound pain relief, often allowing for a significant reduction in opioid consumption. This, in turn, minimizes the adverse effects associated with opioids, such as nausea, vomiting, constipation, sedation, and respiratory depression.
However, the question of what constitutes the “best” nerve block for TKR is not a monolithic one. The optimal choice is often influenced by a confluence of factors, including the specific surgical approach, the patient’s individual pain profile, coexisting medical conditions, surgeon preference, and the anesthesiologist’s expertise. Furthermore, the field of regional anesthesia is dynamic, with ongoing research continually refining techniques and evaluating the efficacy and safety of different nerve block combinations. This article aims to navigate this complex landscape, exploring the commonly utilized nerve blocks for TKR, their respective advantages and disadvantages, and the emerging trends that are shaping future practice.
Anatomical Considerations and Target Nerves
The sensory innervation of the knee joint is complex, involving contributions from multiple nerves that originate from the lumbar and sacral plexuses. A comprehensive understanding of this innervation is paramount to designing effective nerve blockade strategies. The primary nerves responsible for transmitting pain signals from the knee are:
The Femoral Nerve
The femoral nerve, arising from the posterior divisions of the lumbar plexus (L2-L4), is a major contributor to the anterior and medial aspects of the knee. It provides sensory innervation to the quadriceps femoris muscle, the anterior thigh, and a significant portion of the anterior knee capsule, including the patella and medial femoral condyle. A femoral nerve block, therefore, targets a substantial portion of the knee’s sensory input.
The Sciatic Nerve
The sciatic nerve, the largest nerve in the body, originates from the sacral plexus (L4-S3) and travels down the posterior thigh. As it approaches the knee, it bifurcates into the tibial nerve and the common peroneal nerve.
The Tibial Nerve
The tibial nerve innervates the posterior aspect of the knee and continues down to the calf and foot. It contributes sensory fibers to the posterior capsule of the knee.
The Common Peroneal Nerve
The common peroneal nerve divides into the superficial and deep peroneal nerves, providing sensation to the lateral aspect of the knee and the anterior and lateral compartments of the lower leg.
The Obturator Nerve
While often overlooked, the obturator nerve, originating from the anterior divisions of the lumbar plexus (L2-L4), also contributes to the sensory innervation of the medial aspect of the knee and the adductor muscles of the thigh. Its contribution to perioperative pain after TKR is debated but is considered by some to be relevant, particularly in procedures that involve significant manipulation of the medial structures.
The Saphenous Nerve
The saphenous nerve, a major cutaneous branch of the femoral nerve, provides sensation to the skin of the medial leg and ankle. While its direct role in intra-articular knee pain is limited, it can contribute to superficial incisional pain, especially in approaches that involve medial skin incisions.
The goal of an effective nerve block for TKR is to provide a comprehensive blockade of these innervating nerves to achieve profound and sustained analgesia. The choice of block or combination of blocks will dictate the extent and duration of this sensory deficit.
Commonly Employed Nerve Blocks for Total Knee Replacement
The evolution of regional anesthesia has led to the development and refinement of several nerve block techniques for TKR. These blocks can be broadly categorized by the primary nerve targeted and the method of delivery.
The Femoral Nerve Block
The femoral nerve block is perhaps the most traditional and widely utilized regional anesthetic technique for TKR. It effectively blocks the anterior and medial aspects of the knee.
Ultrasound-Guided Femoral Nerve Block
The advent of ultrasound technology has revolutionized the practice of nerve blocks. Ultrasound guidance allows for real-time visualization of the femoral nerve and surrounding anatomical structures, enabling precise needle placement and accurate local anesthetic injection. This increases the success rate of the block, reduces the risk of vascular puncture, and potentially minimizes the volume of local anesthetic required. The femoral nerve is typically identified in the femoral triangle, just lateral to the femoral artery.
Advantages:
- Provides excellent analgesia for the anterior and medial aspects of the knee.
- Facilitates early mobilization due to reduced pain.
- Significantly reduces opioid requirements.
- Relatively easy to perform, especially with ultrasound guidance.
Disadvantages:
- Does not provide complete analgesia for the posterior and lateral aspects of the knee, which can lead to breakthrough pain.
- Risk of motor block in the quadriceps, which can hinder gait training and increase the risk of falls.
- Potential for systemic local anesthetic toxicity if large volumes are injected.
The Sciatic Nerve Block
To address the limitations of the femoral nerve block in covering the posterior knee, a sciatic nerve block is often performed in conjunction with or as an alternative to the femoral block.
Ultrasound-Guided Sciatic Nerve Block
Similar to the femoral nerve block, ultrasound guidance enhances the accuracy and safety of sciatic nerve blockade. The sciatic nerve can be targeted in the popliteal fossa or more proximally in the posterior thigh. Blocking the sciatic nerve provides analgesia to the posterior and lateral aspects of the knee, as well as the calf and foot.

Advantages:
- Complements the femoral nerve block by providing analgesia to the posterior and lateral aspects of the knee.
- Can be performed as a single injection technique for some approaches, if combined with a more distal femoral block.
- Provides analgesia to the entire leg below the knee.
Disadvantages:
- Can be technically more challenging to perform compared to the femoral nerve block, especially in obese patients or those with limited mobility.
- Higher risk of motor block in the calf and foot, which can interfere with ambulation.
- Potential for nerve injury or hematoma formation.
Combined Femoral and Sciatic Nerve Blocks (3-in-1 Block)
The concept of a “3-in-1 block” aims to achieve a more comprehensive blockade by combining the femoral, lateral femoral cutaneous, and obturator nerve blocks with a single injection near the femoral nerve. However, its efficacy for comprehensive knee analgesia, particularly for the posterior structures, remains a subject of debate. In practice, the term is often used loosely to describe a femoral nerve block and a separate sciatic nerve block performed to achieve comprehensive lower extremity analgesia.
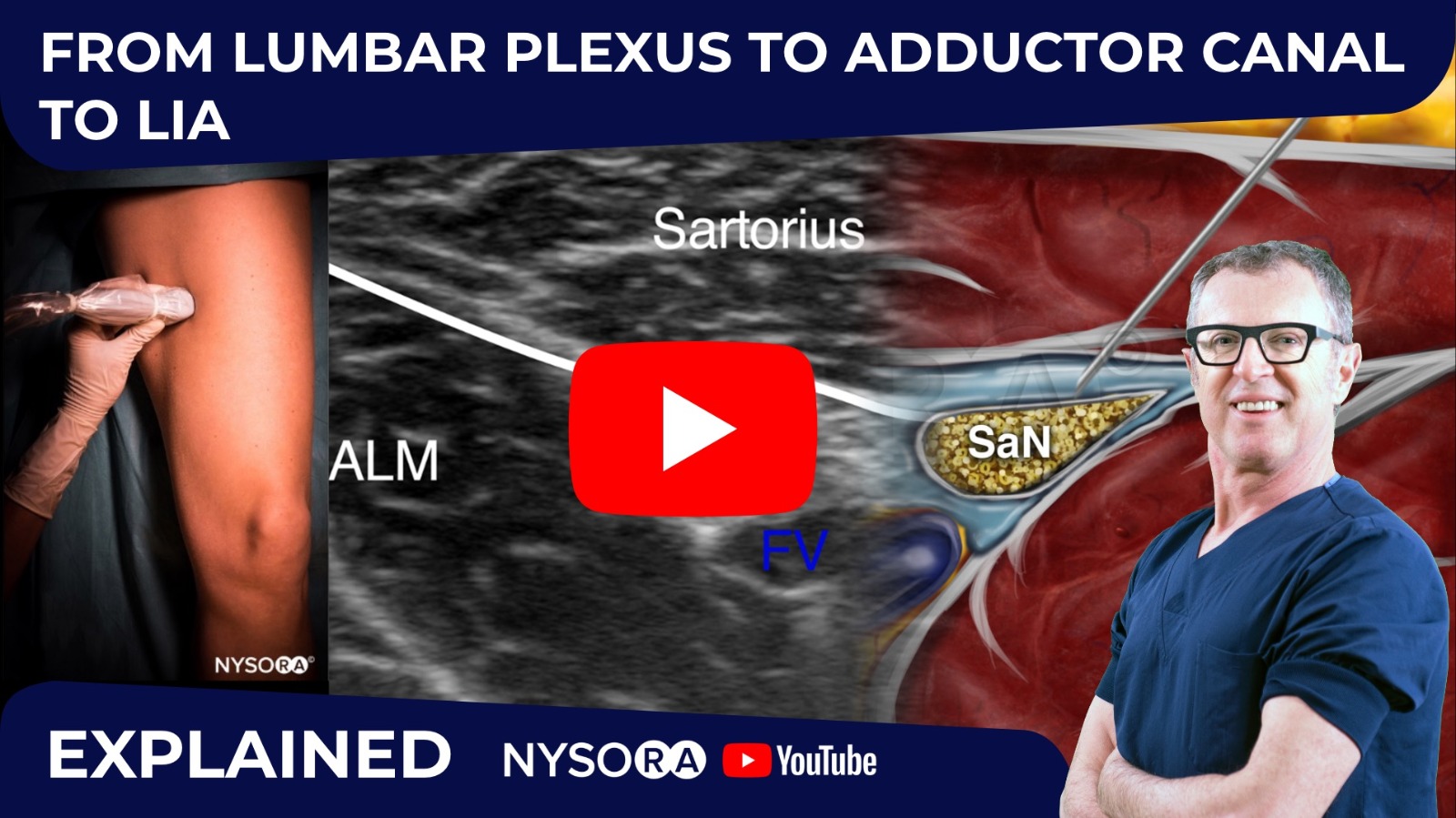
Adductor Canal Block (ACB)
The adductor canal block targets the saphenous nerve and its articular branches as they travel through the adductor canal. This block primarily provides sensory blockade to the medial and distal aspects of the knee and the skin of the medial leg.
Ultrasound-Guided Adductor Canal Block
Ultrasound guidance is essential for accurate identification of the adductor canal and the nerves within it. The block is typically performed in the mid-thigh.
Advantages:
- Provides analgesia to the medial aspect of the knee with minimal motor weakness in the quadriceps, allowing for better quadriceps function and potentially earlier ambulation.
- Reduced risk of systemic local anesthetic toxicity compared to femoral blocks.
- Effective for providing sensory block without significant motor impairment.
Disadvantages:
- Does not provide analgesia to the anterior or posterior aspects of the knee as effectively as femoral or sciatic blocks.
- May not be sufficient as a sole anesthetic modality for TKR pain.
Periarticular Injection
While not a nerve block in the traditional sense, periarticular injections involve injecting a mixture of local anesthetics, opioids, and anti-inflammatory agents directly into the surgical site around the knee joint. This technique aims to provide localized pain relief.
Advantages:
- Minimally invasive.
- Can be performed at the end of surgery.
- Contributes to multimodal pain management.
Disadvantages:
- Effectiveness can be variable.
- Risk of infection or tissue damage.
- Pain relief may be less profound and shorter-lasting compared to nerve blocks.
Emerging Techniques and Future Directions
The quest for optimal pain management in TKR continues, with ongoing research focusing on improving the efficacy, duration, and safety of nerve blocks. Several exciting developments are shaping the future of this field.
Continuous Popliteal Sciatic Nerve Blocks
For prolonged analgesia, continuous sciatic nerve blocks using an indwelling catheter have been employed. A catheter is inserted near the sciatic nerve in the popliteal fossa, and a continuous infusion of local anesthetic is administered.
Advantages:
- Provides extended pain relief for several days postoperatively.
- Allows for patient-controlled analgesia.
- Reduces the need for repeated injections.
Disadvantages:
- Requires specialized equipment and expertise.
- Risk of catheter dislodgement or infection.
- Potential for motor block to persist if the infusion rate is too high.
Regional Anesthesia Combined with Local Anesthetic Infusion Pumps
The integration of nerve blocks with indwelling local anesthetic infusion pumps, such as the On-Q system, offers a sophisticated approach to postoperative analgesia. These systems deliver a continuous or patient-controlled infusion of local anesthetic directly to the surgical site or a targeted nerve.
Novel Local Anesthetic Formulations and Adjuvants
Research is also exploring novel local anesthetic formulations, such as liposomal bupivacaine, which provide prolonged drug release and extended analgesia. Furthermore, the use of adjuvants like dexmedetomidine or opioids in combination with local anesthetics is being investigated to enhance the quality and duration of nerve blockade.
Ultrasound Technology Advancements
The continuous improvement in ultrasound technology, including higher resolution imaging and Doppler capabilities, further enhances the precision and safety of nerve blocks. The development of portable, high-definition ultrasound devices will likely increase the accessibility and utilization of ultrasound-guided regional anesthesia.
Patient-Centered Approaches
Ultimately, the “best” nerve block is one that is tailored to the individual patient’s needs and preferences. Factors such as the patient’s pain tolerance, mobility goals, and concerns about motor weakness are increasingly being considered when selecting a nerve block strategy. Open communication between the patient, surgeon, and anesthesiologist is crucial in achieving optimal outcomes.
Conclusion: A Multimodal Approach for Optimal Pain Relief
The debate surrounding the “best” nerve block for total knee replacement is not a simple matter of declaring one technique superior to all others. Instead, it underscores the importance of a comprehensive, multimodal approach to perioperative pain management. While the femoral nerve block remains a stalwart, its limitations in covering the entire knee necessitate consideration of adjuncts like the sciatic nerve block or alternative strategies such as the adductor canal block.
The advent of ultrasound guidance has undeniably elevated the standard of care in regional anesthesia, offering enhanced precision, safety, and efficacy. Continuous nerve blocks and innovative local anesthetic formulations are further extending the duration and quality of analgesia, facilitating earlier rehabilitation and improved patient satisfaction.
The future of pain management after TKR lies in the judicious selection and combination of these techniques, guided by a thorough understanding of knee innervation, patient-specific factors, and the evolving landscape of anesthetic practice. By embracing a personalized and evidence-based approach, clinicians can effectively mitigate postoperative pain, optimize recovery, and ensure that total knee replacement continues to deliver its promise of restored mobility and improved quality of life.