Understanding the nuances between comfort care and hospice is crucial for navigating end-of-life decisions and ensuring the best possible quality of life for individuals facing serious illnesses. While both approaches prioritize patient well-being and symptom management, they represent distinct phases and philosophies of care. This article delves into the core differences, similarities, and guiding principles of comfort care and hospice, providing clarity for patients, families, and healthcare providers.
Defining Comfort Care
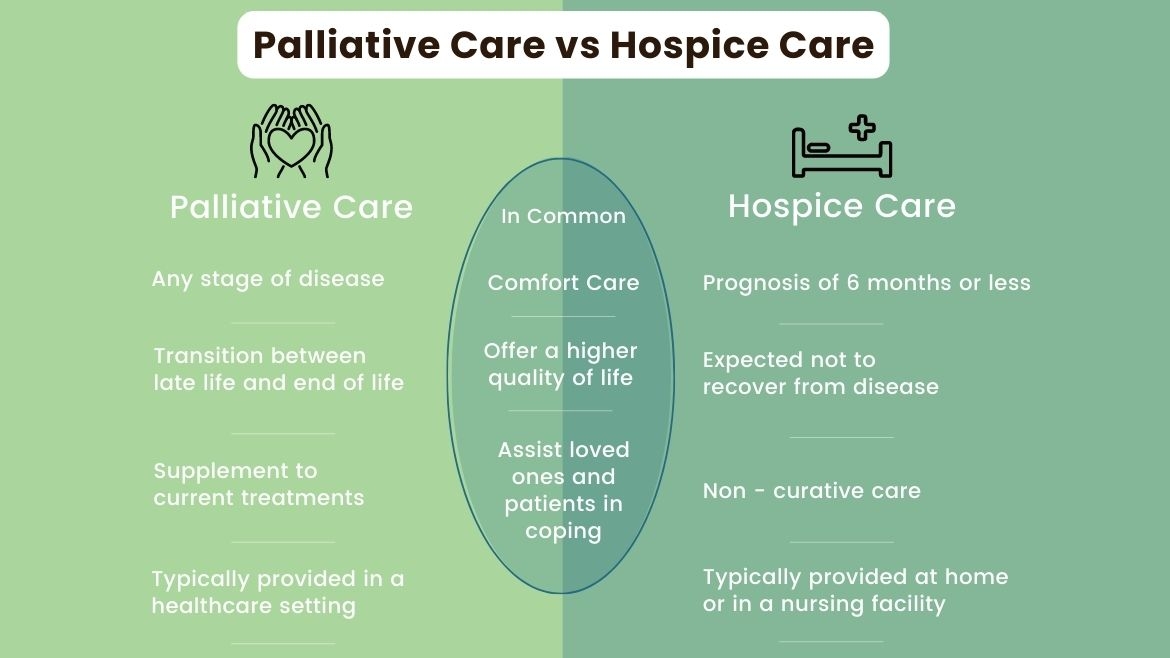
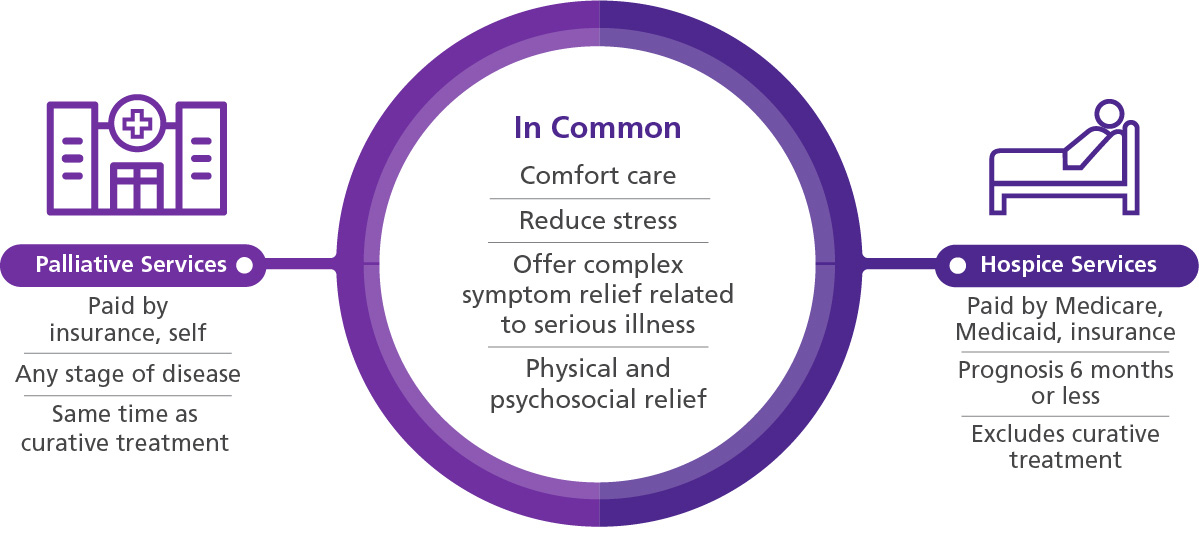
Comfort care, often referred to as palliative care in broader contexts, is a specialized type of medical care focused on providing relief from the symptoms and stress of a serious illness. The primary goal of comfort care is to improve quality of life for both the patient and the family. It can be provided at any stage of a serious illness, regardless of prognosis, and is not necessarily limited to the final months or weeks of life. Comfort care is about managing pain, other symptoms such as nausea, shortness of breath, and fatigue, and addressing the emotional, social, and spiritual needs that arise from living with a chronic or life-limiting condition.
Goals and Scope of Comfort Care
The overarching aim of comfort care is to enhance the patient’s comfort and dignity. This involves a multidisciplinary team approach, often including physicians, nurses, social workers, chaplains, and volunteers, who work collaboratively to create a personalized care plan.
Symptom Management
At its heart, comfort care is about aggressively managing distressing symptoms. This can include:
- Pain Relief: Utilizing a range of pharmacological and non-pharmacological interventions to alleviate pain. This might involve strong pain medications, nerve blocks, or complementary therapies.
- Nausea and Vomiting Control: Employing antiemetics and dietary adjustments to manage gastrointestinal distress.
- Respiratory Symptom Management: Addressing shortness of breath through medication, oxygen therapy, and positioning techniques.
- Fatigue and Weakness: Developing strategies to conserve energy and improve functional capacity where possible.
- Anxiety and Depression: Providing emotional support, counseling, and potentially medication to manage psychological distress.
- Bowel and Bladder Issues: Addressing common concerns like constipation or incontinence.
Holistic Support
Beyond physical symptoms, comfort care recognizes the interconnectedness of a person’s well-being. Therefore, it encompasses:
- Emotional Support: Providing a safe space for patients and families to express their fears, anxieties, and grief. This can involve individual counseling, support groups, and family meetings.
- Spiritual Care: Offering chaplains or spiritual advisors who can assist individuals in finding meaning, peace, and spiritual comfort, irrespective of their religious beliefs.
- Social Support: Connecting patients and families with community resources, legal aid, and assistance with practical matters like advance care planning or navigating insurance.
- Family Involvement: Actively involving family members in the care planning process, providing them with education, emotional support, and respite.
When is Comfort Care Appropriate?
Comfort care is appropriate for individuals with any serious, life-limiting illness, including but not limited to:
- Cancer
- Heart failure
- Chronic obstructive pulmonary disease (COPD)
- Kidney disease
- Neurological conditions like ALS or Parkinson’s disease
- HIV/AIDS
- Dementia or Alzheimer’s disease
It can be initiated at diagnosis, concurrently with curative treatments, or when curative treatments are no longer effective or desired.
Understanding Hospice Care
Hospice care is a specific type of comfort care that is reserved for individuals with a terminal illness who have a prognosis of six months or less, assuming the illness runs its natural course. While the core philosophy of symptom management and holistic support remains the same as general comfort care, hospice care has a more defined focus on the end of life. The primary goal of hospice is to provide compassionate care and support to enable patients to live as fully and comfortably as possible during their final months.
Key Characteristics of Hospice Care
Hospice care is distinguished by several key characteristics:
Prognosis and Eligibility
The most significant differentiator is the eligibility criteria. Hospice is typically for individuals who have stopped curative treatments and whose medical team believes they have a life expectancy of six months or less. This does not mean that care stops if a patient lives longer than six months; rather, the certification of prognosis is re-evaluated.
Medicare and Insurance Coverage
Hospice care is often covered by Medicare under the Medicare Hospice Benefit, as well as by most private insurance plans. This coverage typically includes:
- Physician services
- Nursing care
- Durable medical equipment (e.g., hospital beds, wheelchairs)
- Medications related to the terminal illness
- Respite care
- Inpatient respite care
- Continuous home care
- Grief and bereavement counseling for the family
Setting of Care
Hospice care can be provided in various settings, reflecting the desire to keep patients in their preferred environment:
- Home: The most common setting, allowing patients to remain in the familiar comfort of their own homes, surrounded by loved ones.
- Hospice Centers/Inpatient Units: Specialized facilities designed to provide intensive symptom management and respite for patients and families.
- Skilled Nursing Facilities (SNFs) and Assisted Living Facilities: Hospice teams can work in collaboration with staff at these facilities to provide specialized end-of-life care.
- Hospitals: For short-term periods when more acute symptom management is needed.
The Hospice Team
The hospice team is a multidisciplinary group dedicated to providing comprehensive end-of-life care. This team typically includes:
- Hospice Physician: Oversees the medical care and works with the patient’s primary physician.
- Registered Nurses (RNs) and Licensed Practical Nurses (LPNs): Provide direct patient care, administer medications, monitor symptoms, and educate families.
- Certified Nursing Assistants (CNAs): Assist with personal care, such as bathing, dressing, and feeding.
- Social Workers: Provide emotional support, connect families with resources, and assist with practical concerns.
- Chaplains: Offer spiritual guidance and support.
- Volunteers: Provide companionship, run errands, and offer respite for caregivers.
- Bereavement Counselors: Support the family after the patient’s death.
Key Differences Summarized
While comfort care and hospice care share a common foundation of patient-centered symptom management and holistic support, their primary distinctions lie in their timing, eligibility, and focus.
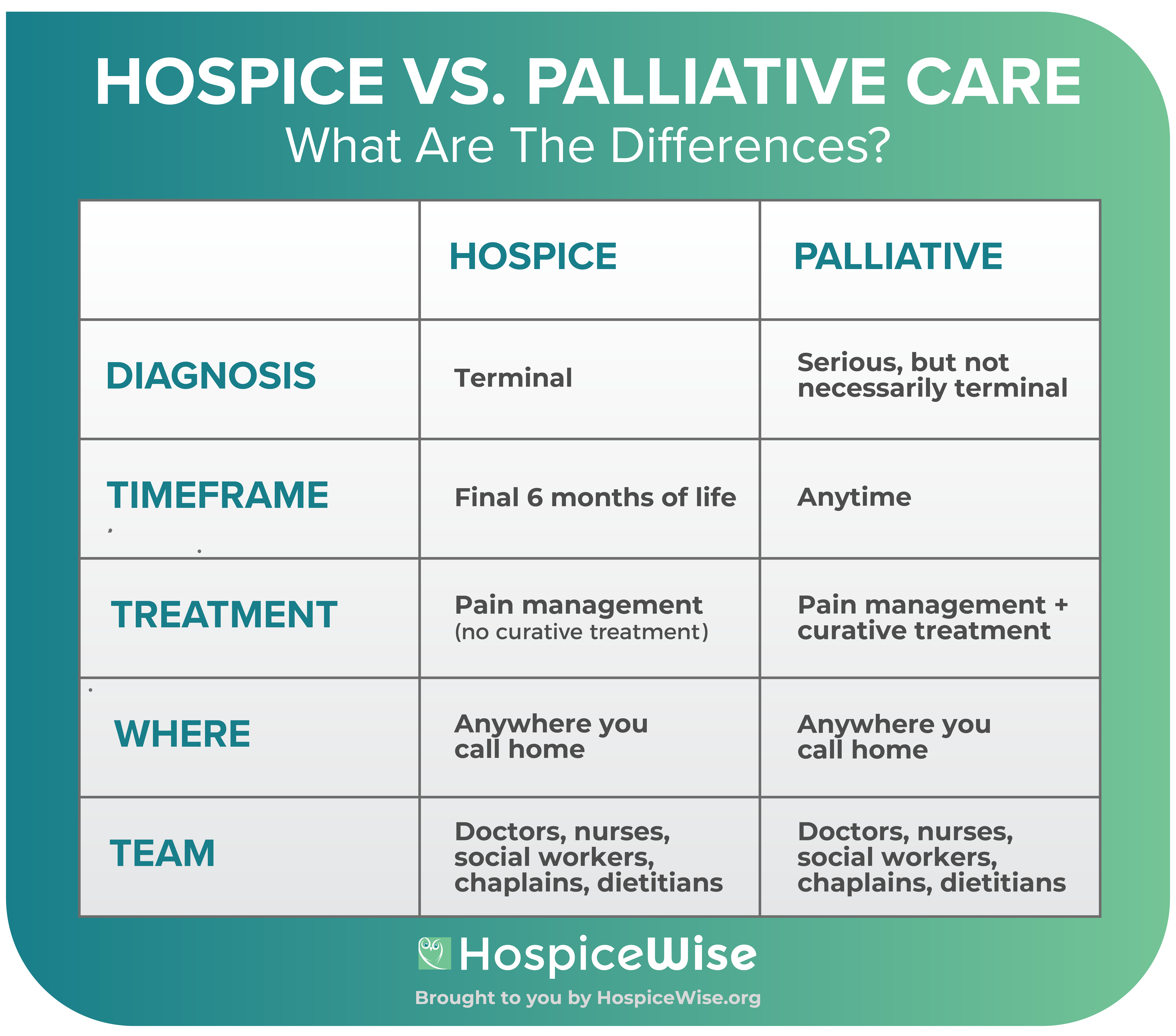
| Feature | Comfort Care | Hospice Care |
|---|---|---|
| Timing | Can be provided at any stage of a serious illness. | For individuals with a terminal illness and a prognosis of six months or less. |
| Goal | Improve quality of life, manage symptoms, and provide support throughout the illness. | Focuses on comfort and quality of life during the final months of life. |
| Eligibility | Broad; for any serious illness. | Limited; requires a medical prognosis of six months or less and discontinuation of curative treatments. |
| Curative Treatment | Can be provided concurrently with curative treatments. | Typically provided when curative treatments are no longer pursued. |
| Focus | Symptom management, emotional, social, and spiritual support for the duration of illness. | Aggressive symptom management, emotional, social, and spiritual support specifically for end-of-life. |
Similarities and Overlap
It is important to recognize that comfort care and hospice are not mutually exclusive; rather, hospice is a specialized form of comfort care. Both prioritize:
- Symptom Management: Alleviating pain, nausea, shortness of breath, and other distressing symptoms is paramount in both approaches.
- Patient Autonomy: Respecting the patient’s wishes and involving them in decision-making.
- Holistic Care: Addressing the physical, emotional, social, and spiritual needs of the patient and their family.
- Dignity and Quality of Life: Ensuring the patient lives with as much comfort, peace, and dignity as possible.
- Family Support: Recognizing the crucial role of the family and providing them with education, emotional support, and resources.
Making the Right Choice
Deciding when to transition from general comfort care to hospice care is a significant decision that should be made in consultation with the patient’s medical team, family, and the patient themselves. Open and honest communication is key. If an individual has a serious illness and is experiencing significant symptoms, or if their prognosis is becoming more limited, discussing the benefits and eligibility for hospice care is a vital step.
Comfort care serves as an umbrella under which hospice operates. It represents a continuum of care focused on alleviating suffering and enhancing well-being. Whether at the early stages of a serious illness or in its final months, the principles of comfort care and hospice aim to ensure that individuals face their health challenges with dignity, support, and the highest possible quality of life.