Fundic polyps are small growths that can develop in the stomach lining, specifically in the fundus, the upper part of the stomach. While often benign, understanding their nature, causes, symptoms, and management is crucial for maintaining gastrointestinal health. This exploration delves into the intricacies of fundic polyps, their implications, and the diagnostic and therapeutic approaches employed by medical professionals.
Understanding Gastric Polyps: A Broader Perspective
Before focusing on fundic polyps, it’s important to contextualize them within the broader category of gastric polyps. Gastric polyps are abnormal tissue growths protruding from the stomach lining. They vary significantly in size, appearance, and potential for malignancy. The classification of gastric polyps is multifaceted, often based on their histological type, which dictates their clinical significance.

Types of Gastric Polyps
Gastric polyps are broadly categorized into several types, each with distinct characteristics and implications:
-
Hyperplastic Polyps: These are the most common type of gastric polyp. They are generally small, sessile (flat-based), and found throughout the stomach, including the fundus. Histologically, they are characterized by an overgrowth of normal gastric mucosal cells. Hyperplastic polyps are almost always benign and rarely pose a significant risk of developing into cancer.
-
Adenomatous Polyps (Adenomas): These polyps are considered pre-malignant. They arise from glandular tissue and have a higher potential to transform into gastric cancer. Adenomas are less common than hyperplastic polyps but warrant careful monitoring and often removal due to this risk. Their size and degree of dysplasia (abnormal cell growth) are critical factors in determining management.
-
Fundic Gland Polyps (FGPs): This is the specific type of polyp that occurs in the fundus. Fundic polyps are essentially a subset of fundic gland polyps. They are characterized by dilated fundic glands, often containing inflamed parietal cells. FGPs are typically small, sessile, and asymptomatic. While they have a very low risk of malignant transformation, their development is often linked to certain underlying conditions.
-
Inflammatory Polyps: These polyps develop in response to chronic inflammation in the stomach lining, often associated with conditions like H. pylori infection or autoimmune gastritis. They are typically benign but can cause symptoms if they become large or bleed.
-
Gastric Hamartomas: These are benign tumors composed of disorganized but mature tissue elements normally found in the stomach. They are rare and typically not associated with malignancy.
-
Gastrointestinal Stromal Tumors (GISTs): While not technically polyps in the traditional sense, GISTs are mesenchymal tumors that can arise from the stomach wall and project into the lumen, mimicking a polyp. GISTs have the potential to be malignant and require specific diagnostic and management strategies.
The differentiation between these types is critical for appropriate patient care. A biopsy and histological examination by a pathologist are essential for accurate diagnosis.
The Fundus: A Specific Location
The fundus is the dome-shaped uppermost region of the stomach, located above the esophageal opening. It plays a role in storing food and is a primary site for the secretion of gastric acid and intrinsic factor by parietal and chief cells, respectively. The unique environment and cellular composition of the fundus contribute to the development of specific types of polyps, most notably fundic gland polyps.
Fundic Polyps: Causes and Risk Factors
Fundic polyps, specifically fundic gland polyps, are the most common type of polyp found in the stomach. While the exact cause of their formation is not fully understood, several factors are believed to contribute to their development.
Proton Pump Inhibitor (PPI) Use
One of the most significant associations with fundic polyps is the long-term use of proton pump inhibitors (PPIs). PPIs are medications widely prescribed to reduce stomach acid production, commonly used for conditions like gastroesophageal reflux disease (GERD), peptic ulcers, and Zollinger-Ellison syndrome.
The mechanism by which PPIs may lead to fundic polyps is thought to involve the sustained suppression of gastric acid. Gastric acid plays a role in regulating the proliferation of gastric epithelial cells. When acid production is chronically inhibited, there can be a compensatory increase in gastrin levels, a hormone that stimulates cell growth. Elevated gastrin can, in turn, promote the development and growth of fundic gland polyps. Studies have shown a dose-dependent and duration-dependent relationship between PPI use and the development of fundic polyps; the longer and at higher doses PPIs are used, the greater the likelihood of polyp formation.
Genetic Predisposition
While not as prominent a factor as PPI use, genetic predisposition can also play a role in the development of fundic polyps. Certain inherited conditions, such as familial adenomatous polyposis (FAP) and hereditary nonpolyposis colorectal cancer (HNPCC), can increase the risk of developing polyps throughout the gastrointestinal tract, including the stomach. However, fundic gland polyps themselves are not typically considered a direct manifestation of these hereditary syndromes.
Other Contributing Factors
Other less definitively established factors that may be associated with fundic polyp development include:
-
H. pylori Infection: While Helicobacter pylori infection is a significant risk factor for other types of gastric polyps and gastric cancer, its direct link to fundic gland polyps is less clear. Some studies suggest a potential, albeit weaker, association.
-
Age: Like many conditions affecting the gastrointestinal tract, the incidence of polyps may increase with age.
-
Sex: Some research indicates a slightly higher prevalence of fundic polyps in women.
It is important to note that in many cases, fundic polyps can develop without any identifiable risk factors, making regular gastrointestinal check-ups particularly important, especially for individuals with a history of gastric issues or those on long-term medications.
Symptoms and Diagnosis of Fundic Polyps
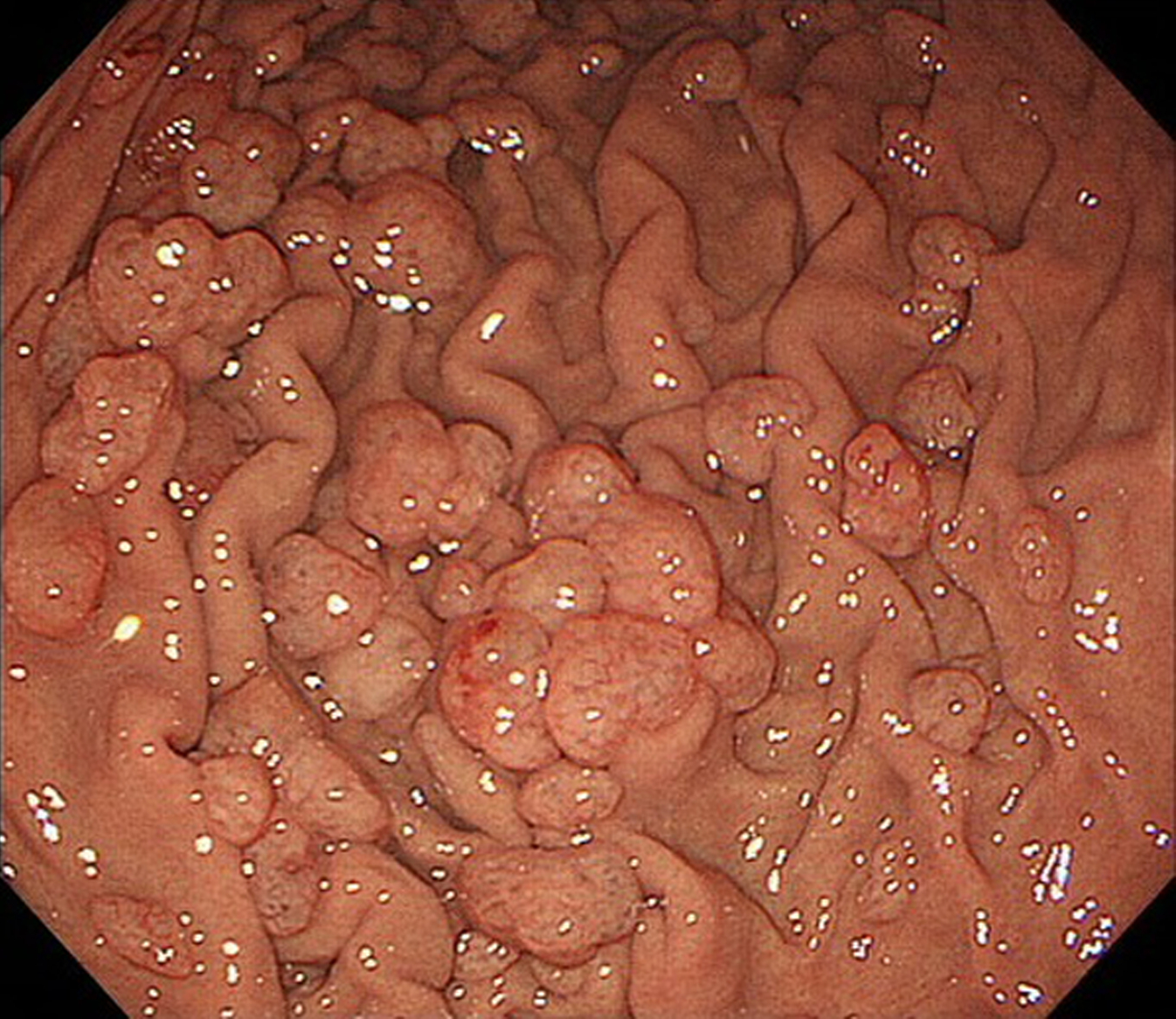
The majority of fundic polyps are small and asymptomatic, meaning they do not cause any noticeable symptoms. They are often discovered incidentally during endoscopic examinations performed for other reasons. However, when symptoms do occur, they can be related to the size or number of polyps, or if they cause complications.
Potential Symptoms
While rare, larger fundic polyps or a significant number of polyps can potentially lead to:
- Abdominal Pain or Discomfort: This can manifest as a dull ache or pressure in the upper abdomen.
- Nausea and Vomiting: Especially if the polyps cause any obstruction or irritation.
- Bleeding: Polyps can sometimes erode, leading to slow, chronic bleeding that may not be apparent without testing, or in rare cases, more significant bleeding that can cause anemia. This chronic bleeding might present as iron deficiency anemia, characterized by fatigue, pallor, and shortness of breath.
- Changes in Bowel Habits: While less common with fundic polyps compared to colonic polyps, significant bleeding can affect stool appearance (e.g., black, tarry stools if bleeding is in the upper GI tract).
The absence of symptoms does not preclude the presence of fundic polyps, highlighting the importance of routine screenings.
Diagnostic Methods
The primary method for diagnosing fundic polyps is through upper endoscopy, also known as esophagogastroduodenoscopy (EGD).
-
Upper Endoscopy (EGD): This procedure involves a gastroenterologist inserting a flexible tube with a camera attached (endoscope) through the mouth, down the esophagus, and into the stomach and duodenum (the first part of the small intestine). The endoscope allows for direct visualization of the stomach lining, enabling the identification of any polyps. During the procedure, the endoscopist can assess the size, shape, and number of polyps.
-
Biopsy and Histological Examination: The crucial step in diagnosing fundic polyps accurately is taking a biopsy. Small tissue samples of the polyps are removed during the endoscopy using specialized instruments. These samples are then sent to a pathologist, who examines them under a microscope to determine the type of polyp (hyperplastic, adenomatous, etc.) and to assess for any precancerous changes or malignancy. This histological examination is vital for guiding treatment and management decisions.
-
Imaging Studies (Less Common for Initial Diagnosis): While endoscopy is the gold standard, in some specific circumstances or for assessing larger lesions or complications, other imaging techniques might be employed. These could include:
- Barium Swallow: This involves drinking a barium solution, which coats the lining of the esophagus and stomach, making them visible on X-rays. It can help identify larger polyps or irregularities in the stomach lining but is less sensitive than endoscopy for small lesions.
- CT Scan or MRI: These may be used to assess the extent of larger tumors or to investigate for metastasis if malignancy is suspected, but they are not primary tools for diagnosing typical fundic polyps.
The comprehensive diagnostic approach, starting with endoscopy and biopsy, ensures accurate identification and characterization of fundic polyps, paving the way for appropriate clinical management.
Management and Treatment of Fundic Polyps
The management of fundic polyps is largely determined by their type, size, number, and the presence of any associated symptoms or risk factors. For the most part, fundic gland polyps, which are the most common type of fundic polyp, have a very low risk of becoming cancerous.
Watchful Waiting for Benign Polyps
For small, asymptomatic fundic gland polyps, especially those confirmed to be hyperplastic or benign fundic gland polyps, a strategy of watchful waiting is often employed. This typically involves:
-
Regular Endoscopic Surveillance: The gastroenterologist may recommend periodic follow-up endoscopies to monitor the polyps for any changes in size, number, or appearance. The frequency of these surveillance procedures will depend on individual factors, such as the patient’s medical history, the characteristics of the polyps, and the treating physician’s judgment. For many small fundic gland polyps, surveillance might be recommended every 1-3 years.
-
Addressing Underlying Causes: If the fundic polyps are associated with long-term PPI use, a discussion with the physician may involve evaluating the necessity and dosage of the PPI. In some cases, the PPI might be reduced or stopped, if medically appropriate, to see if the polyps regress. However, this decision must be made in consultation with the doctor, as discontinuing PPIs for conditions like severe GERD can lead to symptom recurrence and complications.
Endoscopic Removal (Polypectomy)
While many fundic polyps are managed conservatively, endoscopic removal is recommended in certain situations:
-
Suspicion of Adenoma or Malignancy: If a polyp appears suspicious during endoscopy, or if a biopsy reveals it to be an adenoma or shows precancerous changes (dysplasia), it will almost always be removed to prevent the development of gastric cancer. Adenomatous polyps have a clear potential for malignant transformation.
-
Large Polyps: Even if benign, very large polyps (typically over 1 cm or 2 cm, though this threshold can vary) may be removed due to a slightly increased risk of bleeding or obstruction, or simply for ease of monitoring.
-
Symptomatic Polyps: If polyps are causing symptoms such as pain, bleeding, or nausea, removal might be considered to alleviate these issues.
-
Multiple or Recurring Polyps: In cases of numerous polyps or those that recur frequently, a more aggressive approach to removal might be adopted.
The endoscopic removal of polyps is known as polypectomy. This procedure is typically performed during an EGD using various techniques, such as:
- Hot Biopsy Forceps: For very small polyps, a heated forceps can be used to cut and cauterize the polyp stalk.
- Snare Polypectomy: For larger polyps, a wire loop snare is passed through the endoscope. The snare is looped around the base of the polyp and tightened, and then an electrical current is used to cut the polyp away and cauterize the base to prevent bleeding.
- Endoscopic Mucosal Resection (EMR): This technique is used for larger or flatter polyps. A fluid is injected under the polyp to lift it away from the deeper layers of the stomach wall, making it easier to resect with a snare, reducing the risk of perforation.
Medical Management
Beyond addressing PPI use, there is generally no specific medication to shrink or eliminate existing fundic polyps. The focus of medical management is on diagnosis, monitoring, and the removal of polyps when indicated. However, managing underlying conditions that might contribute to gastric inflammation or dysregulation is a crucial aspect of overall gastrointestinal health.

Follow-up Care
After a polyp has been removed, or if a patient is on a surveillance program, regular follow-up is essential. This may involve repeat endoscopies at intervals determined by the pathologist’s findings, the number and size of the polyps, and the patient’s individual risk factors. Adhering to the recommended follow-up schedule is paramount for early detection of any recurrence or the development of new polyps.