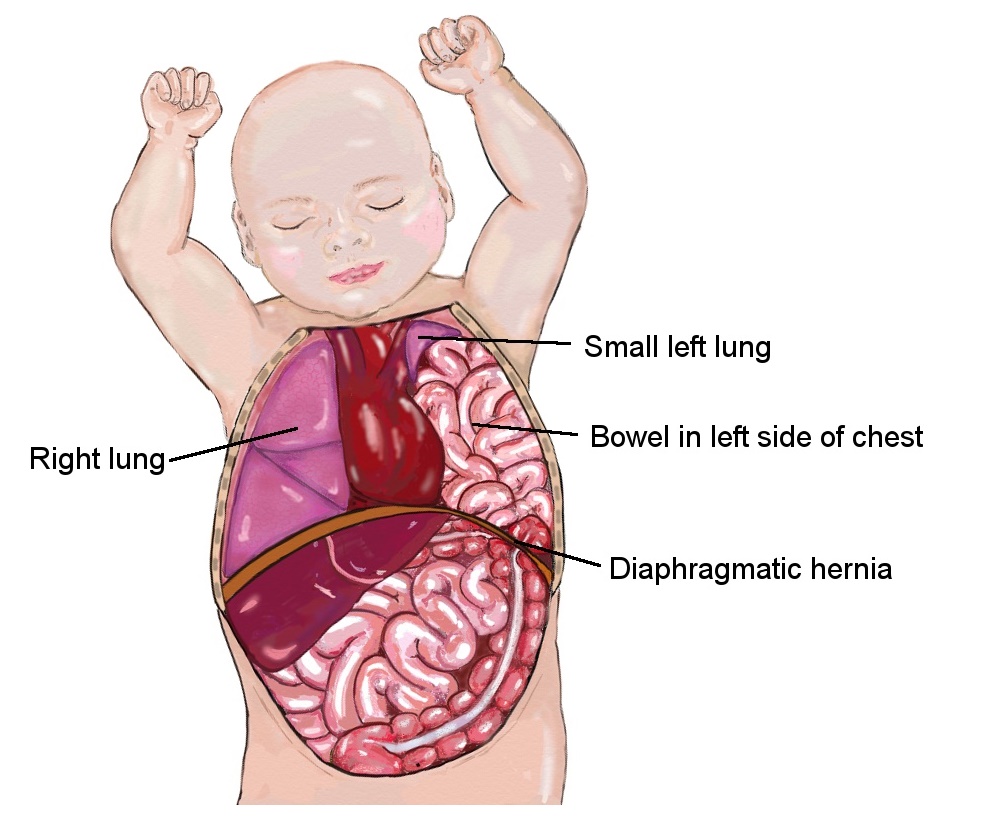
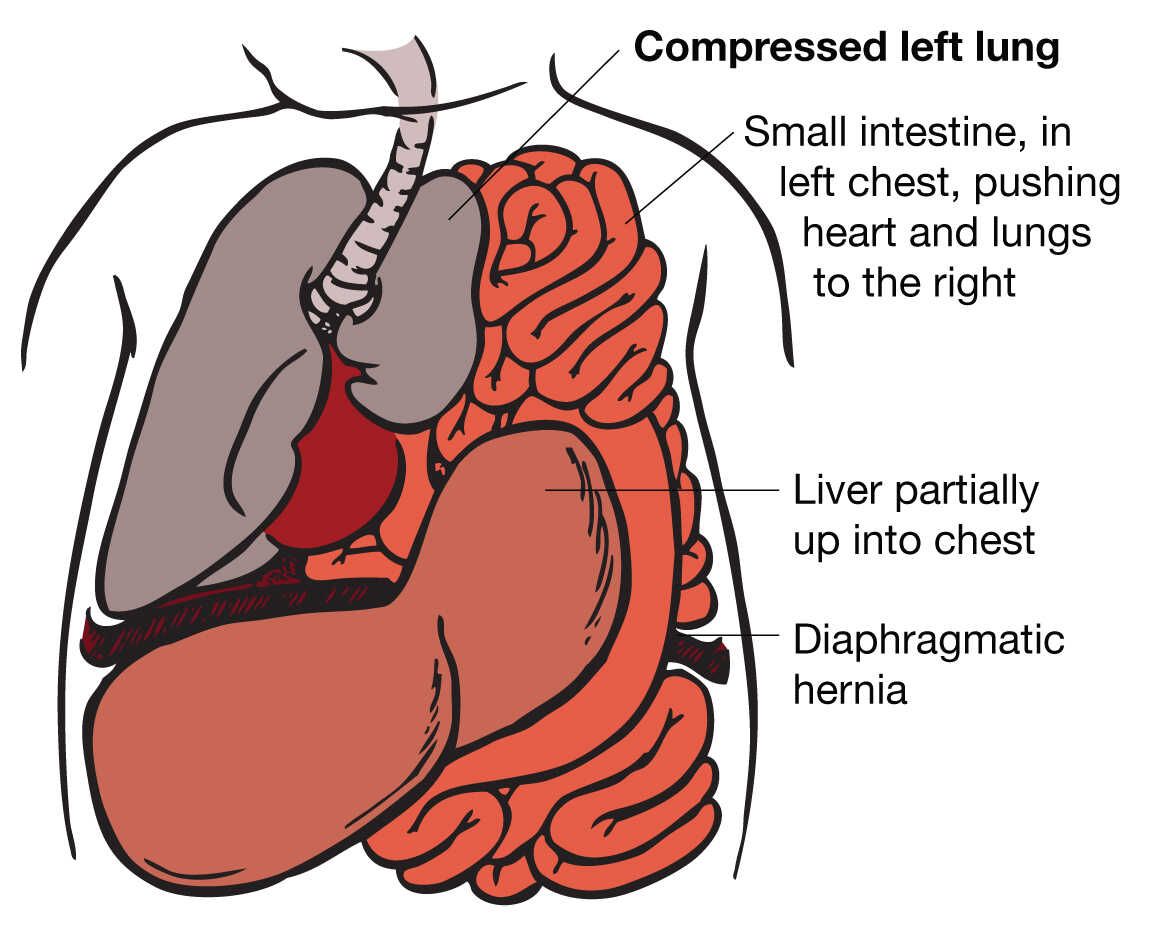
The acronym “CDH” in medical terminology stands for Congenital Diaphragmatic Hernia. This is a serious birth defect that occurs when the diaphragm, a large muscle that separates the abdomen from the chest, does not form completely. This incomplete closure allows organs from the abdomen, such as the stomach, intestines, and liver, to move into the chest cavity. This displacement can interfere with the development of the lungs, leading to breathing problems and other complications for the newborn.
Understanding Congenital Diaphragmatic Hernia
Congenital Diaphragmatic Hernia (CDH) is a complex condition with a significant impact on affected infants. Its presence during fetal development poses a substantial threat to the viability and well-being of the newborn. Understanding the intricacies of CDH is crucial for medical professionals, expectant parents, and the wider community to facilitate timely diagnosis, appropriate management, and effective support.
The Diaphragm’s Role
The diaphragm is a dome-shaped muscle situated at the base of the chest cavity, below the lungs and heart. It plays a vital role in respiration by contracting and flattening during inhalation, drawing air into the lungs, and relaxing during exhalation, expelling air. Its complete formation is essential for proper lung function and the separation of the thoracic and abdominal cavities, which house distinct organ systems.
The Defect in CDH
In CDH, a hole or defect exists in the diaphragm. This anomaly typically occurs during the early stages of fetal development, around the eighth week of gestation. The size and location of the defect can vary, but the most common type is a posterolateral defect, occurring in the back and side of the diaphragm. Less common locations include the anterior (front) or central diaphragm. The severity of CDH is often directly correlated with the size of the defect and the extent to which abdominal organs have herniated into the chest.
Impact on Fetal Development
The presence of abdominal organs in the chest cavity during fetal development has profound consequences for the lungs. This overcrowding restricts the space available for the lungs to grow and mature. As a result, the affected lung (or lungs, in some cases) may be underdeveloped, a condition known as pulmonary hypoplasia. The pulmonary arteries, which supply blood to the lungs, may also be abnormally developed, leading to high blood pressure in the lungs (pulmonary hypertension). These developmental issues can significantly impair the infant’s ability to breathe effectively after birth.
Diagnosis and Identification of CDH
The diagnosis of Congenital Diaphragmatic Hernia can occur at various stages, from prenatal screening to postnatal assessment. Early detection is paramount for optimizing outcomes.
Prenatal Diagnosis
Increasingly, CDH is identified during routine prenatal ultrasounds. When a sonographer observes abnormalities in the fetal chest or abdomen, such as an enlarged chest cavity, the presence of abdominal organs in the chest, or underdeveloped lungs, further investigation is warranted. Specialized fetal echocardiograms and detailed ultrasounds may be employed to confirm the diagnosis and assess the severity of the condition. Magnetic Resonance Imaging (MRI) can also provide valuable, detailed anatomical information. Prenatal diagnosis allows for specialized care planning before birth, including identifying a delivery hospital equipped to manage neonates with CDH.
Postnatal Diagnosis
In some instances, CDH may not be detected before birth and can present immediately after delivery. Newborns with CDH often exhibit signs of respiratory distress, including rapid breathing (tachypnea), difficulty breathing, bluish discoloration of the skin (cyanosis) due to low oxygen levels, and an abnormally shaped chest (scaphoid abdomen – sunken abdomen). A physical examination may reveal diminished breath sounds on one side of the chest. Diagnostic imaging, typically a chest X-ray, is crucial for confirming the presence of abdominal organs in the chest cavity and assessing the extent of lung hypoplasia. Other tests, such as an echocardiogram, may be performed to evaluate for associated cardiac anomalies and assess the severity of pulmonary hypertension.
Management and Treatment of CDH
The management of Congenital Diaphragmatic Hernia is a multidisciplinary endeavor, requiring the coordinated efforts of neonatologists, pediatric surgeons, pulmonologists, cardiologists, and other specialists. The primary goals are to stabilize the infant’s respiratory and hemodynamic status, surgically repair the diaphragmatic defect, and manage potential long-term complications.
Immediate Stabilization
Upon diagnosis, the infant is typically transferred to a neonatal intensive care unit (NICU) equipped to handle complex surgical cases. Immediate management focuses on supporting breathing and circulation. This often involves:
- Ventilation: Mechanical ventilation is frequently required to assist the infant’s breathing. However, conventional ventilation can sometimes worsen pulmonary hypertension, so strategies like high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO) may be employed. ECMO acts as an artificial heart and lung, providing oxygen to the blood and removing carbon dioxide, allowing the infant’s lungs and heart to rest and recover.
- Medications: Medications may be administered to manage pulmonary hypertension and support cardiovascular function.
Surgical Repair
Once the infant is stabilized, surgical repair of the diaphragmatic defect is performed. The timing of surgery can vary depending on the infant’s condition, but it is generally carried out within the first few days of life.
- Surgical Approaches: The repair can be performed through open surgery (a traditional incision) or minimally invasive laparoscopic surgery. Laparoscopic surgery, when feasible, offers smaller incisions, potentially leading to less pain and faster recovery.
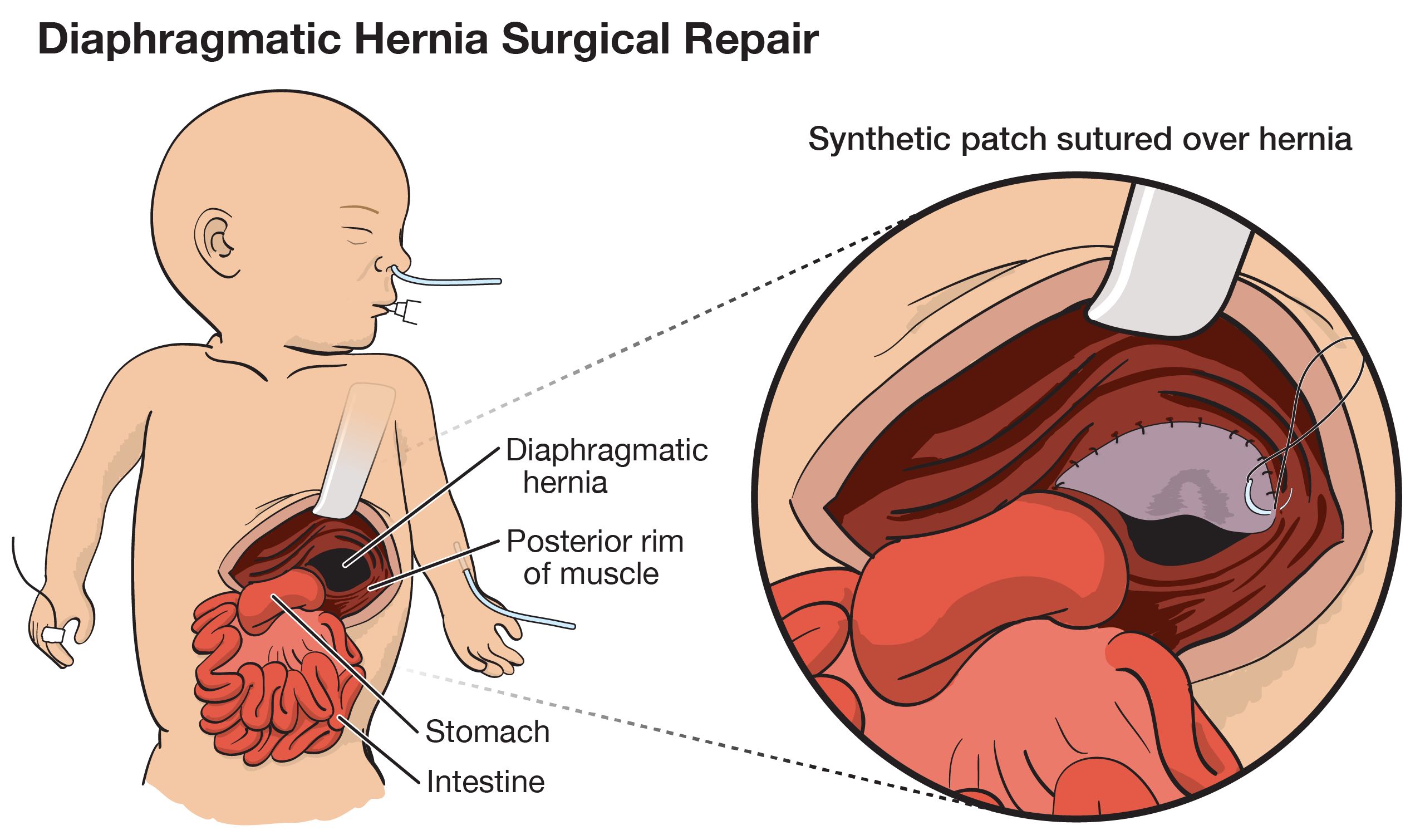
- The Repair Process: During surgery, the abdominal organs are carefully returned to their proper position in the abdomen. The defect in the diaphragm is then closed. In cases of large defects where direct closure is not possible, a synthetic patch or the infant’s own tissue (fascia lata) may be used to reconstruct the diaphragm.
Post-operative Care and Long-Term Management
The recovery period following surgery can be lengthy and complex. Infants often require prolonged stays in the NICU, continuing respiratory support, and careful monitoring for complications.
- Respiratory Support: Many infants continue to require some form of respiratory support even after surgery. Gradual weaning from mechanical ventilation is a key goal.
- Nutritional Support: Feeding difficulties are common, and infants may require specialized feeding methods, such as nasogastric or gastrostomy tubes, to ensure adequate nutrition for growth and healing.
- Gastrointestinal Issues: Abdominal organs that were displaced into the chest may have altered motility, leading to issues like reflux or delayed gastric emptying.
- Growth and Development: Infants with CDH are at increased risk for developmental delays. Comprehensive developmental follow-up, including monitoring for gross and fine motor skills, cognitive development, and speech, is essential.
- Pulmonary Surveillance: Ongoing monitoring of lung function is crucial. Recurrent respiratory infections are common, and some individuals may require long-term management for chronic lung disease.
- Cardiac Monitoring: Given the frequent association with cardiac anomalies, continued cardiac evaluation may be necessary.
Prognosis and Outlook for CDH
The prognosis for infants with Congenital Diaphragmatic Hernia has significantly improved over the past few decades due to advancements in prenatal diagnosis, surgical techniques, and neonatal intensive care. However, outcomes remain variable and depend on several factors, including:
- Severity of Lung Hypoplasia: The degree of underdeveloped lungs is a primary determinant of survival and long-term respiratory function.
- Presence of Other Anomalies: CDH can occur in isolation or in conjunction with other birth defects, which can impact prognosis.
- Timing of Diagnosis and Intervention: Early and effective management is crucial.
- Response to Treatment: The infant’s ability to tolerate ventilation, surgical repair, and recovery plays a significant role.
While many infants with CDH can survive and lead fulfilling lives, they may face lifelong challenges related to respiratory health, feeding, and development. Comprehensive, long-term follow-up care is essential to address these ongoing needs and optimize their quality of life. Continued research into the causes of CDH, improved diagnostic tools, and innovative treatment strategies remains vital to further enhance outcomes for affected children.