Pregnancy is a journey filled with new terminology, and understanding these terms is crucial for effective communication with healthcare providers. Among the most fundamental concepts in obstetric history are “gravida” and “para.” These two terms, often used in conjunction, provide a concise yet powerful snapshot of a woman’s reproductive history. While they might seem like simple counts, their implications extend to assessing risks, planning care, and understanding a woman’s unique obstetric background. This article delves into the definitions, significance, and practical applications of gravida and para in the context of pregnancy and beyond.

Understanding Gravida: The Foundation of Pregnancy Count
Gravida, often abbreviated as “G,” refers to the total number of times a woman has been pregnant, regardless of the outcome. This includes current pregnancies, miscarriages, abortions, and births. The key distinction is that it counts the pregnancies themselves, not the number of fetuses or the number of babies delivered. For instance, a woman who is currently pregnant for the first time, has had one miscarriage, and has given birth to twins would have a gravida of 3.
The Nuances of Gravidity
It is important to clarify what constitutes a “pregnancy” for the purpose of gravidity. Generally, a pregnancy is counted from the first day of the last menstrual period (LMP) and is typically considered viable if it progresses beyond a certain gestational age, often around 20 weeks. However, some definitions may vary slightly. For practical clinical purposes, any pregnancy that results in a detectable gestational sac or implantation is usually counted.
- Current Pregnancy: A woman’s ongoing pregnancy is always included in her gravida count.
- Miscarriages (Spontaneous Abortions): Pregnancies that end spontaneously before the point of viability are counted.
- Induced Abortions: Pregnancies terminated intentionally are also included in the gravida count.
- Ectopic Pregnancies: These are pregnancies that occur outside the uterus. Despite not resulting in a viable intrauterine pregnancy, they are still counted as a pregnancy.
- Molar Pregnancies (Hydatidiform Moles): These are abnormal pregnancies where tissue from the placenta grows abnormally. They are also counted towards the gravida.
The gravida number is a straightforward count, and it serves as the initial step in understanding a woman’s obstetric history. It’s a fundamental piece of information that immediately tells a healthcare provider how many times a woman has experienced pregnancy.
Deciphering Para: The Outcomes of Pregnancy
Para, often abbreviated as “P,” is a more detailed measure that refers to the number of times a woman has given birth to a fetus reaching at least 20 weeks of gestation, or weighing at least 500 grams, regardless of whether the baby was born alive or stillborn. The para count focuses solely on the outcomes of pregnancies that reached a certain stage of development.
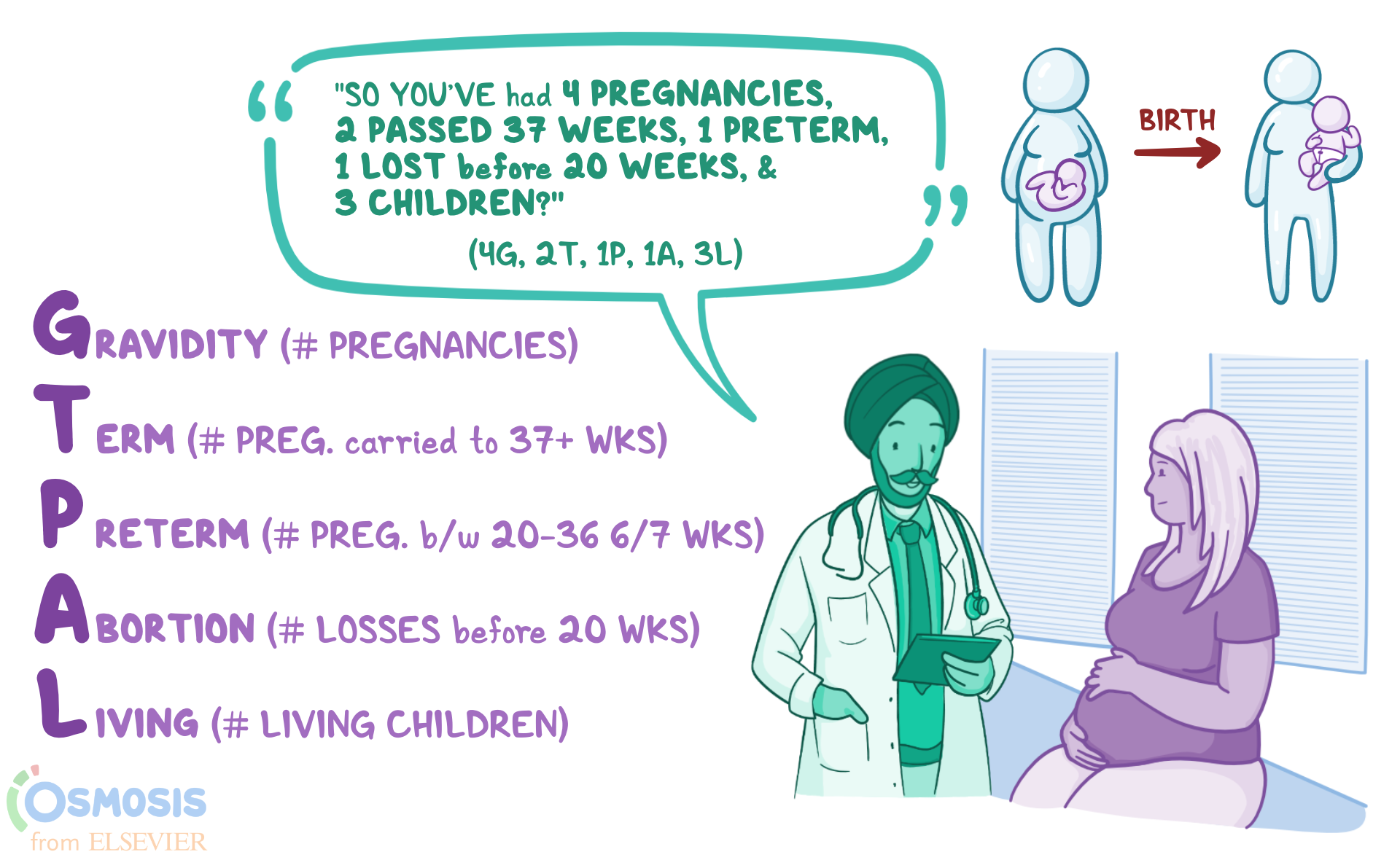
The para notation is often presented as a set of four numbers (TPAL), though sometimes it’s simplified. The most common and comprehensive notation is TPAL, which breaks down the para count further:
- T (Term): The number of deliveries at or after 37 completed weeks of gestation. This includes both vaginal births and Cesarean sections.
- P (Preterm): The number of deliveries between 20 completed weeks of gestation and 36 completed weeks and 6 days of gestation.
- A (Abortions): The number of pregnancies terminated before 20 completed weeks of gestation. This includes both spontaneous miscarriages and induced abortions.
- L (Living): The number of children currently living from previous pregnancies.
Let’s consider an example to illustrate the TPAL system:
A woman has:
- One pregnancy that resulted in a vaginal birth at 39 weeks.
- One pregnancy that ended in a miscarriage at 10 weeks.
- One pregnancy that resulted in a Cesarean section at 35 weeks.
- One current pregnancy at 28 weeks.
Her Gravida (G) would be 4 (one current pregnancy + one vaginal birth + one miscarriage + one C-section).
Her Para (P) would be represented by TPAL:
- T (Term): 1 (the vaginal birth at 39 weeks)
- P (Preterm): 1 (the C-section at 35 weeks)
- A (Abortions): 1 (the miscarriage at 10 weeks)
- L (Living): 2 (assuming the vaginal birth resulted in one living child and the C-section resulted in one living child).
Therefore, her obstetric history would be documented as G4, P1112.
Simplified Para Notation
In some contexts, a simpler para notation might be used, such as “Para X,” where X represents the total number of births after 20 weeks of gestation. For instance, if a woman has given birth to three babies after 20 weeks, her para would be 3. This simplified notation can be less informative than the TPAL system as it doesn’t distinguish between term and preterm births or include abortion history.
Key Considerations for Para
- Gestational Age: The 20-week mark is a critical threshold for defining a “para.” Pregnancies ending before this are considered abortions.
- Viability: While the 20-week mark is a general guideline, some institutions might use a specific weight (e.g., 500 grams) or a specific gestational age based on local definitions of viability.
- Multiple Births: A single pregnancy resulting in twins or triplets counts as one birth for the para notation. For example, delivering twins at term contributes ‘1’ to the ‘T’ category, not ‘2’. The number of living children is what reflects the actual number of babies.
- Stillbirths: A stillbirth occurring at or after 20 weeks of gestation is counted as a birth for the para notation but would not be included in the “Living” count if the baby did not survive.
The Clinical Significance of Gravida and Para
The gravida and para notation is more than just a way to record a woman’s reproductive history; it’s a vital tool for healthcare providers. It offers a rapid assessment of a woman’s obstetric risk factors and helps tailor her care plan.
Risk Assessment
A woman’s obstetric history, as summarized by G and P, can indicate potential risks for future pregnancies. For instance:
- High Gravida: A high gravida might suggest a woman who has experienced multiple pregnancies, which can sometimes be associated with increased risks such as uterine atony (poor uterine tone after birth), placenta previa, or placental abruption.
- Multiple Preterm Births (High P): A history of preterm births increases the risk of future preterm deliveries. This can prompt closer monitoring for signs of preterm labor and interventions like progesterone therapy.
- History of Abortions (High A): Recurrent miscarriages can be a sign of underlying reproductive issues that may need investigation and management.
- Multiple Cesarean Sections (High T/P with C-sections): Multiple C-sections increase the risk of complications in subsequent pregnancies, such as placenta accreta spectrum disorders, uterine rupture, and adhesions.
Planning Care
Understanding a woman’s gravida and para helps healthcare providers anticipate potential complications and plan accordingly. For example:
- Previous Large Babies: If a woman has delivered large babies in the past (reflected in the ‘T’ category), there might be a higher risk of cephalopelvic disproportion or birth trauma in a current pregnancy, influencing delivery mode decisions.
- Previous Uterine Surgeries: A history of myomectomies or other uterine surgeries can impact the mode of delivery and require careful management during pregnancy and labor.
- Maternal Health Conditions: A woman with a history of gestational diabetes or preeclampsia in previous pregnancies (which might be inferred from the TPAL breakdown if specific conditions are noted alongside deliveries) will require closer monitoring in subsequent pregnancies.
Communication
Gravida and para serve as a standardized language among healthcare professionals. When a new provider reviews a patient’s chart, this notation provides an immediate and concise summary of her obstetric background, allowing them to quickly grasp her reproductive history and any associated risks. This efficiency is crucial in busy clinical settings and ensures continuity of care.

Beyond the Numbers: Context and Individualization
While gravida and para are invaluable statistical tools, it is essential to remember that they are just a snapshot. The numbers do not tell the whole story of a woman’s reproductive journey. A comprehensive understanding of her health requires a thorough discussion that goes beyond these simple counts.
Factors that are not explicitly captured by gravida and para include:
- Complications of Past Pregnancies/Deliveries: The TPAL notation might indicate a preterm birth, but it doesn’t detail the specific reasons for that preterm birth (e.g., preeclampsia, placental abruption, infection).
- Maternal Health Status: Chronic conditions like diabetes, hypertension, or autoimmune disorders can significantly impact pregnancy outcomes, regardless of the gravida and para.
- Socioeconomic Factors: Factors such as access to prenatal care, nutrition, and stress levels can play a crucial role in pregnancy outcomes.
- Emotional and Psychological Impact: The experience of pregnancy loss, difficult births, or preterm deliveries can have profound emotional and psychological effects that are not reflected in the G/P numbers.
Therefore, while gravida and para provide a vital framework for understanding a woman’s obstetric history, they must always be considered within the broader context of her individual health, experiences, and the clinical picture. Healthcare providers must engage in open and empathetic communication with their patients to fully appreciate the nuances of their reproductive lives and provide the most appropriate and personalized care. This holistic approach ensures that every woman’s unique journey is acknowledged and supported.