Understanding Embolectomy: A Lifesaving Intervention
An embolectomy is a crucial surgical or minimally invasive procedure designed to remove an embolus – a blood clot or other foreign substance that has traveled through the bloodstream and become lodged in a blood vessel, obstructing blood flow. This blockage can lead to severe consequences, including tissue damage, organ failure, and even death, depending on the location and size of the embolus. While the term “embolectomy” broadly refers to clot removal, it is most commonly associated with the treatment of arterial embolisms, particularly those affecting the limbs, brain, or heart.
The underlying cause of an embolism is often a thrombus, a blood clot that forms within a blood vessel. However, emboli can also consist of other materials, such as fat globules (fat embolism), air bubbles (air embolism), or even fragments of tumors. When these substances break free and travel through the circulatory system, they can lodge in narrower vessels, causing a critical obstruction. The urgency of an embolectomy is directly proportional to the severity of the blockage and the importance of the affected organ or tissue. Prompt intervention is paramount to restore blood flow and prevent irreversible damage.
The decision to perform an embolectomy, and the specific technique employed, depends on a multitude of factors. These include the location and extent of the blockage, the patient’s overall health and comorbidities, the presence of any contraindications to surgery or certain medications, and the timeframe since the onset of symptoms. Advances in medical technology have led to the development of both traditional open surgical approaches and less invasive endovascular techniques, offering a range of options to effectively address embolic events.
The Embolus: A Wandering Threat
An embolus is essentially a mobile obstruction in the circulatory system. Unlike a thrombus, which is stationary and forms in situ, an embolus originates elsewhere and travels through the bloodstream. The most common type of embolus is a thromboembolism, which is a piece of a thrombus that has broken off and is carried by the blood flow.
Types of Emboli:
- Thromboemboli: These are the most frequent cause of embolic events. They typically arise from deep vein thrombosis (DVT) in the legs, where a clot forms and then dislodges, traveling to the lungs (pulmonary embolism) or, less commonly, to the arterial circulation through a patent foramen ovale (PFO).
- Fat Emboli: These can occur after fractures of long bones or extensive soft tissue injury, where fat globules are released into the bloodstream. Fat emboli can lodge in the lungs, brain, and other organs, causing a range of symptoms.
- Air Emboli: Introduced into the bloodstream through medical procedures (e.g., intravenous lines, surgery) or trauma, air bubbles can obstruct blood flow. The size and number of bubbles determine the severity of the obstruction.
- Amniotic Fluid Emboli: A rare but catastrophic event, amniotic fluid containing fetal cells, vernix, and meconium can enter the maternal circulation during labor or delivery, leading to a severe systemic reaction.
- Septic Emboli: These are fragments of infected material, often from a bacterial endocarditis (infection of heart valves), that break off and travel to other parts of the body, causing abscesses and further infections.
- Cholesterol Crystal Emboli: Small cholesterol crystals can break off from atherosclerotic plaques in arteries and travel downstream, causing ischemia in smaller vessels, often presenting as “trash foot” syndrome.
The journey of an embolus ends when it reaches a blood vessel too narrow for it to pass through, causing an obstruction. The consequences of this blockage are determined by the vessel’s size, the organ it supplies, and the duration of the occlusion.
Symptoms and Diagnosis of Embolic Events
The symptoms of an embolic event are highly variable and depend on the location of the blockage. However, they are generally characterized by a sudden onset of signs and symptoms related to compromised blood flow to the affected area.
Common Symptoms by Location:
- Limbs (Arterial Embolism): This is one of the most common presentations of embolic disease requiring embolectomy. Symptoms include sudden, severe pain, pallor (paleness), pulselessness, paresthesia (numbness or tingling), paralysis, and poikilothermia (coldness) in the affected limb – often referred to as the “six Ps.” This is a medical emergency, as prolonged ischemia can lead to irreversible muscle and nerve damage and necessitate amputation.
- Brain (Cerebral Embolism): This results in an ischemic stroke. Symptoms are often sudden and focal, including weakness or numbness on one side of the body, difficulty speaking or understanding speech, vision problems, dizziness, loss of balance, and severe headache. Time is critical in treating stroke, and rapid intervention can significantly improve outcomes.
- Heart (Coronary Embolism): While less common than coronary artery thrombosis, emboli can cause myocardial infarction (heart attack) by blocking coronary arteries. Symptoms include chest pain or pressure, shortness of breath, pain radiating to the arm or jaw, and sweating.
- Lungs (Pulmonary Embolism): Although embolectomy is not the primary treatment for most pulmonary embolisms, large or life-threatening PEs may necessitate surgical or mechanical removal of the clot. Symptoms include sudden shortness of breath, chest pain (often sharp and pleuritic, worsening with breathing), rapid heart rate, coughing (sometimes with bloody sputum), and lightheadedness.
Diagnostic Tools:
Accurate and swift diagnosis is critical for effective treatment. A combination of clinical assessment and imaging studies is employed:
- Medical History and Physical Examination: A detailed account of the patient’s symptoms, risk factors (such as atrial fibrillation, DVT history, recent surgery), and a thorough physical examination are the first steps. For limb emboli, the focus is on assessing pulse strength, skin color, temperature, and motor and sensory function.
- Doppler Ultrasound: This non-invasive technique uses sound waves to visualize blood flow and detect blockages. It is particularly useful for diagnosing DVT and assessing blood flow in the limbs.
- Angiography (Arteriography/Venography): This is often considered the gold standard for diagnosing embolic events. A contrast dye is injected into the blood vessel, and X-ray images are taken to visualize the extent and location of the blockage. This procedure can be both diagnostic and therapeutic, as interventions can be performed during the same session.
- CT Angiography (CTA): This imaging technique uses computed tomography (CT) scans and contrast dye to create detailed 3D images of blood vessels. It is widely used for diagnosing pulmonary emboli and arterial blockages, particularly in the brain and abdomen.
- MRI Angiography (MRA): Similar to CTA, MRA uses magnetic resonance imaging to visualize blood vessels, often without the use of ionizing radiation. It is particularly useful for assessing blood flow in the brain and in patients who cannot tolerate contrast dye.
- Echocardiography: An ultrasound of the heart, echocardiography can identify blood clots within the heart chambers (e.g., in atrial fibrillation) or on heart valves, which can be a source of emboli.
- Electrocardiogram (ECG): While not directly diagnosing an embolus, an ECG can detect abnormalities in heart rhythm (like atrial fibrillation) that are significant risk factors for embolic stroke.
The Embolectomy Procedure: Restoring Flow
Embolectomy encompasses a range of techniques, from open surgery to minimally invasive endovascular approaches, all aimed at physically removing the obstructing embolus. The choice of method is dictated by the location, size, and nature of the embolus, as well as the patient’s overall condition.
Open Surgical Embolectomy
This traditional approach involves a direct surgical incision to access the affected blood vessel. The surgeon then uses specialized instruments to manually extract the embolus.
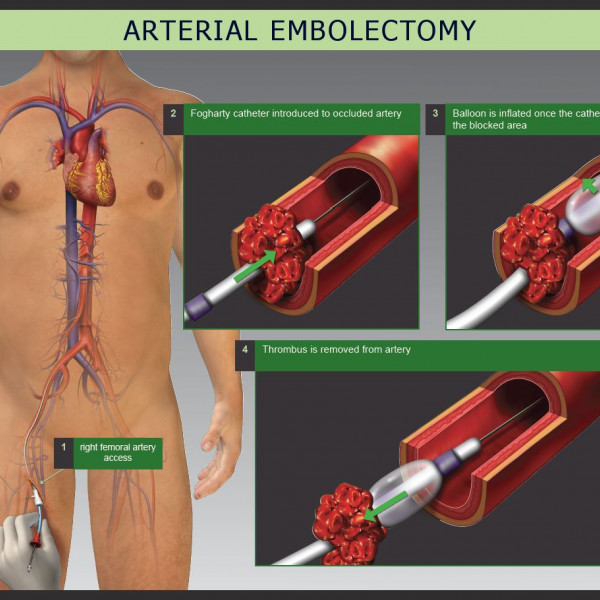
- Procedure: A surgical cut is made over the occluded artery or vein. The vessel is then carefully dissected and exposed. An arteriotomy (an incision into the artery) or venotomy (an incision into the vein) is performed. A Fogarty catheter, a flexible tube with an inflatable balloon at its tip, is then inserted into the vessel past the clot. The balloon is inflated, and the catheter is gently withdrawn, pulling the embolus with it. Multiple passes may be necessary to ensure complete removal. After the embolus is removed, the incision in the vessel is repaired with sutures.
- Indications: Open surgical embolectomy is often preferred for large, proximal emboli, or when endovascular approaches are not feasible or have failed. It is also considered when there is associated damage to the blood vessel wall that requires direct repair. It is commonly performed for acute limb ischemia.
- Advantages: Can be very effective in removing large or complex emboli and allows for direct visualization and repair of the vessel.
- Disadvantages: More invasive, requiring a larger incision, longer recovery time, and carrying higher risks of infection and bleeding compared to endovascular techniques.

Endovascular Embolectomy
Endovascular techniques involve performing the procedure from within the blood vessel, using catheters and specialized devices inserted through small puncture sites, typically in the groin or arm. This approach offers significant advantages in terms of reduced invasiveness and faster recovery.
Catheter-Directed Embolus Removal
This technique utilizes catheters to reach the embolus and then employs various methods to break it down or remove it.
- Thrombolysis: This involves infusing a potent clot-dissolving medication (thrombolytic agent) directly into or around the embolus. The medication works by activating plasmin, an enzyme that breaks down fibrin, the protein that forms the meshwork of a blood clot. Thrombolysis can take several hours, and the patient is closely monitored. It is often used in conjunction with mechanical removal.
- Mechanical Thrombectomy/Thrombolysis: This category encompasses a variety of devices designed to physically break up or extract the clot.
- Aspiration Thrombectomy: Catheters with large lumens are used to suck out the clot. Smaller clots can often be removed in this manner.
- Rotational Atherectomy Devices: These devices use a rotating catheter tip to fragment the clot, which can then be aspirated or allowed to pass.
- Pharmacomechanical Thrombectomy: This combines the use of thrombolytic drugs with mechanical disruption of the clot. For instance, a catheter might deliver micro-bubbles using ultrasound to enhance the penetration and effectiveness of thrombolytic agents.
- Angioplasty Balloons: After clot removal or lysis, angioplasty balloons may be used to open up any residual narrowed segments (stenosis) in the artery.
Embolectomy Devices and Techniques
Beyond the general categories, specific devices and techniques are employed for endovascular embolectomy:
- Fogarty Embolectomy Catheter (Endovascular Use): While originally used in open surgery, modified Fogarty catheters can be advanced endovascularly to snare and remove emboli.
- AngioVac System: This system uses a large-bore suction catheter with a vacuum pump to aspirate large volumes of blood and clot, particularly effective in large veins and the right side of the heart.
- Stent Retrievers: Primarily used for acute ischemic stroke, these devices are designed to capture and retrieve clots from cerebral arteries. They are deployed like a stent, trapping the clot, and then retracted.
- Suction Catheters: Various designs of suction catheters are available for aspirating thrombus from different vessel sizes.
Indications for Endovascular Embolectomy:
- Acute limb ischemia, especially in patients who are poor surgical candidates.
- Cerebral ischemia (stroke) due to arterial embolism.
- Peripheral arterial emboli where surgical access is challenging.
- Pulmonary embolism where thrombolysis is contraindicated or has failed.
Advantages of Endovascular Embolectomy:
- Minimally invasive, with smaller incisions and less trauma to the blood vessel.
- Shorter hospital stays and faster recovery times.
- Reduced risk of infection and bleeding.
- Can be performed under local anesthesia or conscious sedation.
- Allows for treatment of multiple lesions or concurrent angioplasty and stenting if needed.
Disadvantages of Endovascular Embolectomy:
- May not be effective for very large, firm, or organized clots.
- Risk of vessel perforation or dissection.
- Potential for distal embolization of clot fragments if not carefully managed.
- Requires specialized equipment and highly skilled interventional radiologists or vascular surgeons.
Post-Embolectomy Care and Long-Term Management
Following an embolectomy, meticulous post-operative care and long-term management are critical to ensure successful recovery, prevent recurrent embolic events, and manage underlying conditions. The goals are to restore optimal circulation, minimize complications, and address the root cause of the embolism.
Immediate Post-Operative Care
The immediate post-operative period focuses on monitoring the patient for signs of complications and ensuring the success of the intervention.
- Hemodynamic Monitoring: Vital signs, including blood pressure, heart rate, and oxygen saturation, are closely monitored. Continuous cardiac monitoring is essential, especially after procedures involving the heart or major arteries.
- Pain Management: Adequate pain relief is provided through intravenous medications or patient-controlled analgesia to ensure comfort and facilitate early mobilization.
- Wound Care: Incision sites are kept clean and dry, and signs of infection, such as redness, swelling, or discharge, are closely watched for.
- Neurological and Vascular Assessment: For limb embolectomies, the affected limb is regularly assessed for warmth, color, sensation, and motor function. For cerebral embolectomies, neurological status is continuously evaluated for any changes.
- Fluid and Electrolyte Balance: Intravenous fluids are administered to maintain hydration and electrolyte balance, especially if thrombolytic agents were used, as these can sometimes affect clotting factors.
- Anticoagulation: Anticoagulant medications, such as heparin or warfarin, are typically initiated or continued post-procedure to prevent the formation of new clots and reduce the risk of re-occlusion. The specific anticoagulant and duration will depend on the underlying cause of the embolism.

Long-Term Management and Prevention
Preventing future embolic events is paramount. This involves addressing the underlying risk factors and adopting lifestyle modifications.
- Anticoagulation Therapy: For many patients, long-term anticoagulation therapy is a cornerstone of prevention. The choice of anticoagulant (e.g., warfarin, direct oral anticoagulants like rivaroxaban, apixaban, dabigatran) depends on the specific cause of the embolism, patient comorbidities, and individual response. Regular monitoring of blood thinning levels may be required.
- Antiplatelet Therapy: In cases where atherosclerosis is a contributing factor, or after procedures like angioplasty and stenting, antiplatelet medications (e.g., aspirin, clopidogrel) may be prescribed to prevent clot formation on plaques or stents.
- Management of Underlying Conditions:
- Atrial Fibrillation: This is a major cause of embolic stroke. Effective rate or rhythm control and anticoagulation are vital.
- Peripheral Artery Disease (PAD): Lifestyle modifications, medication, and possibly further revascularization procedures are crucial for managing PAD.
- Heart Valve Disease: If a malfunctioning heart valve was the source of emboli, surgical repair or replacement may be necessary.
- Deep Vein Thrombosis (DVT): Adequate anticoagulation and, in some cases, inferior vena cava filters are used to prevent pulmonary embolisms.
- Lifestyle Modifications:
- Smoking Cessation: Smoking significantly damages blood vessels and increases clot risk.
- Healthy Diet: A balanced diet low in saturated fats and cholesterol can help manage conditions like atherosclerosis.
- Regular Exercise: Physical activity improves circulation and cardiovascular health.
- Weight Management: Obesity is a risk factor for cardiovascular disease and DVT.
- Follow-up Imaging and Vascular Surveillance: Regular check-ups with vascular specialists or cardiologists may include imaging studies (e.g., ultrasound, angiography) to monitor the treated vessel, assess for new blockages, and evaluate the effectiveness of ongoing treatment.
The success of an embolectomy extends beyond the removal of the immediate clot. Comprehensive post-operative care and a proactive approach to long-term management are essential to restore quality of life and prevent the devastating consequences of recurrent embolic events.