Adenoid cystic carcinoma (ACC) is a rare type of malignant (cancerous) tumor that can develop in various parts of the body, most commonly in the salivary glands. While often associated with the head and neck region, it can also arise in other glandular tissues, including those in the lacrimal glands (tear ducts), breasts, skin, and even the respiratory tract. Despite its rarity, ACC is known for its distinct histological features, slow but persistent growth, and a tendency for perineural invasion (spreading along nerves), which can contribute to its challenging treatment and management.
Understanding Adenoid Cystic Carcinoma
At its core, adenoid cystic carcinoma is a cancer that originates from the glandular cells responsible for producing secretions. These glands are found throughout the body, and their secretory function is crucial for lubrication, protection, and other physiological processes. The term “adenoid” refers to the glandular origin, while “cystic” describes the characteristic microscopic appearance of the tumor, often showing cystic spaces. The “carcinoma” designation signifies that it is a malignant epithelial tumor.
Histological Features and Subtypes
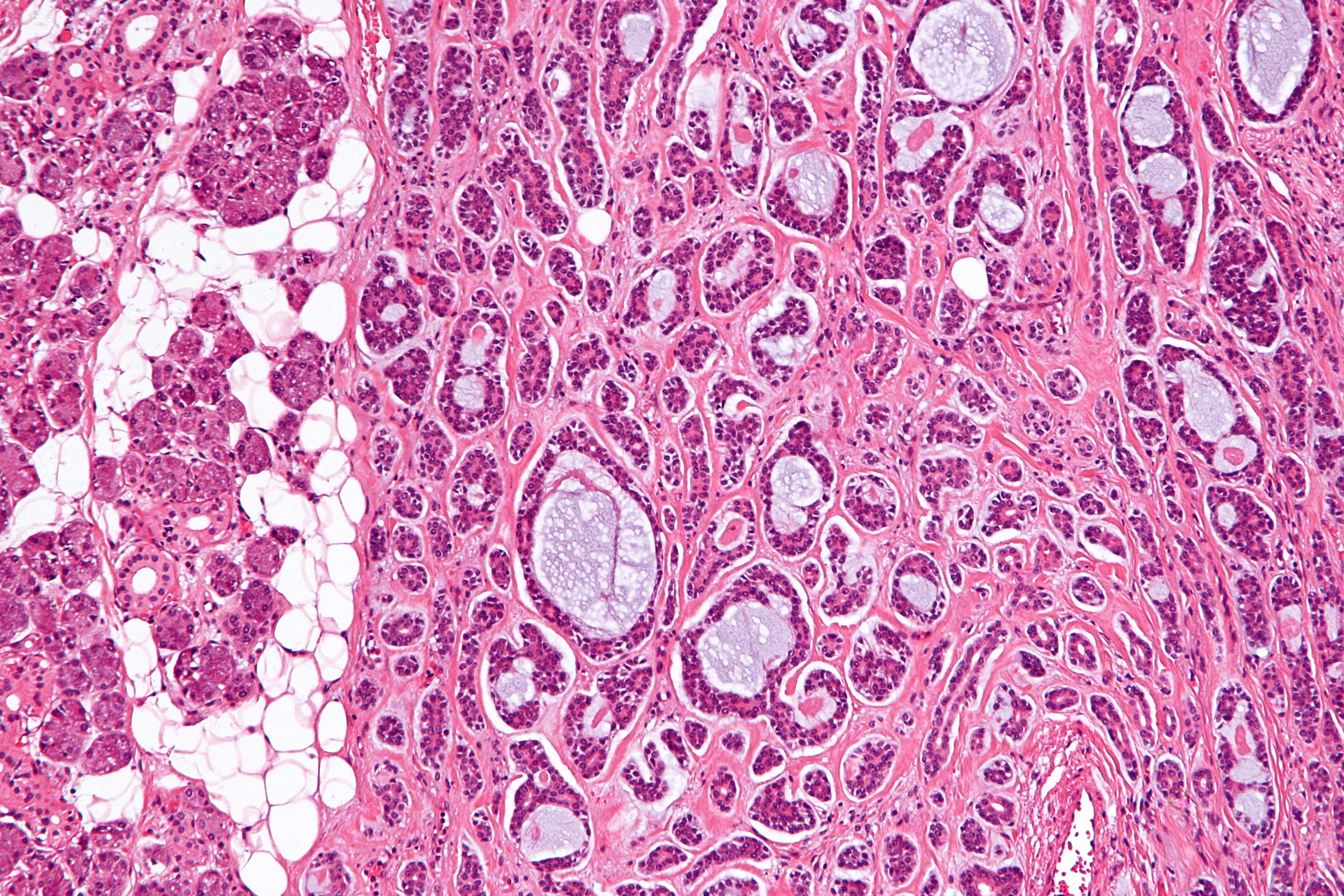
Microscopically, ACC exhibits a highly characteristic pattern that distinguishes it from other cancers. Pathologists identify three main histological patterns, though a single tumor can exhibit a combination of these:
- Cribriform Pattern: This is the most common pattern and is characterized by a sieve-like or cribriform arrangement of tumor cells, with islands of tumor cells separated by spaces that are filled with a mucoid or hyaline material. These spaces can appear as small, punched-out holes, giving the tumor a Swiss-cheese-like appearance under the microscope.
- Tubular Pattern: In this pattern, the tumor cells form well-defined tubes or duct-like structures, often lined by a double layer of cells. These tubules may be scattered within the tumor mass.
- Solid Pattern: This is the least common pattern but is often associated with a more aggressive clinical course. It features nests or sheets of tumor cells with little to no intervening stromal tissue or cystic spaces.
The presence and proportion of these patterns can sometimes influence the prognosis, with the solid pattern generally considered to be more aggressive.
Epidemiology and Risk Factors
ACC is considered an uncommon malignancy, accounting for a small percentage of all salivary gland tumors. It can occur at any age, but it is more frequently diagnosed in adults, typically between the ages of 40 and 60. There is no significant gender predilection, meaning it affects men and women equally.
Unlike many other cancers, well-established environmental or lifestyle risk factors, such as smoking or alcohol consumption, are not strongly associated with ACC. The exact causes of ACC remain largely unknown. Research is ongoing to understand the genetic mutations and cellular mechanisms that drive its development. Some studies have investigated the role of certain viral infections or exposure to radiation, but definitive links are yet to be established.
Sites of Origin
While the salivary glands are the most common primary site for ACC, it’s important to recognize its potential to arise in other glandular locations:
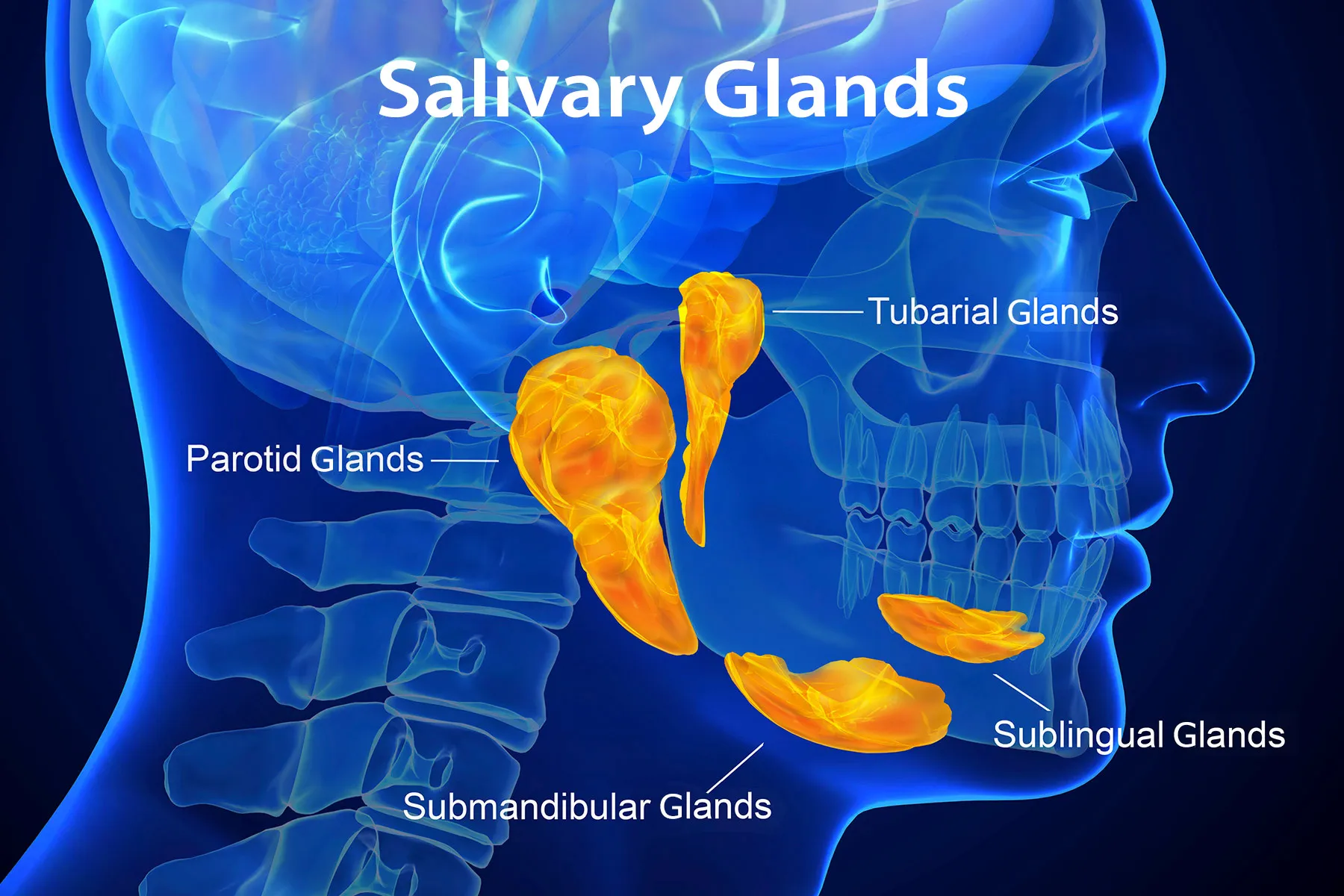
- Salivary Glands: This includes both major salivary glands (parotid, submandibular, sublingual) and minor salivary glands found throughout the oral cavity, palate, tongue, and pharynx. ACC in the salivary glands often presents as a slow-growing mass that may be painless.
- Lacrimal Glands: ACC can develop in the tear-producing glands of the eye, leading to symptoms such as swelling, pain, or vision changes.
- Breast: ACC of the breast is a rare entity, often presenting as a palpable mass.
- Skin: ACC of the skin can occur in hair follicles or sweat glands, typically appearing as a nodule or ulcer.
- Respiratory Tract: ACC can occur in the trachea, bronchi, and nasal cavity, leading to symptoms like persistent cough, shortness of breath, or nasal obstruction.
- Other Sites: Less commonly, ACC can arise in the esophagus, stomach, prostate, and cervix.
The specific symptoms associated with ACC depend heavily on its location and size.
Clinical Presentation and Diagnosis
The clinical presentation of ACC is often insidious, characterized by slow growth and nonspecific symptoms. This can sometimes lead to delayed diagnosis, as the tumor may be present for a considerable time before it becomes noticeable or causes significant discomfort.
Symptoms
Symptoms vary widely depending on the tumor’s location:
- Head and Neck (Salivary Glands): A palpable, slow-growing mass that may or may not be painful. If it affects cranial nerves, symptoms like facial weakness, numbness, or difficulty swallowing can occur. Tumors near the ear may cause ear pain or ringing.
- Lacrimal Glands: Swelling in the upper eyelid, pain around the eye, decreased tearing, or vision disturbances.
- Respiratory Tract: Persistent cough, hoarseness, difficulty breathing, or wheezing. Tumors in the nasal passages can cause nasal obstruction, bleeding, or facial pain.
- Breast: A firm, palpable lump that is usually painless.
A key characteristic of ACC, regardless of its site of origin, is its tendency to spread along nerves. This perineural invasion can lead to localized pain that may be out of proportion to the visible or palpable tumor, or it can cause neurological deficits in the affected area.
Diagnostic Process
The diagnostic process for ACC typically involves a multi-faceted approach:
-
Medical History and Physical Examination: A thorough review of the patient’s symptoms, medical history, and a detailed physical examination are the initial steps. For tumors in accessible areas, a clinician will carefully palpate for masses and assess for any signs of nerve involvement or other abnormalities.
-
Imaging Studies: Various imaging techniques are crucial for determining the tumor’s size, location, and extent, as well as identifying any potential spread to nearby structures. These may include:
- Computed Tomography (CT) Scan: Provides detailed cross-sectional images of the body, useful for evaluating bone involvement and the tumor’s relationship to surrounding tissues.
- Magnetic Resonance Imaging (MRI): Offers excellent soft tissue contrast, making it particularly valuable for visualizing tumors in the head and neck, brain, and other areas where detailed soft tissue assessment is needed. It is also superior for detecting perineural invasion.
- Positron Emission Tomography (PET) Scan: Can help identify metabolically active areas, indicating the presence of cancer cells, and assess for distant metastases.
-
Biopsy and Histopathology: The definitive diagnosis of ACC is made through a biopsy. This involves obtaining a tissue sample from the suspected tumor, which is then examined under a microscope by a pathologist. The pathologist will identify the characteristic histological features of ACC, including the cribriform, tubular, or solid patterns, and assess for perineural invasion. The biopsy can be performed through a fine-needle aspiration (FNA), core needle biopsy, or an excisional biopsy (surgical removal of the entire lesion).
-
Other Tests: Depending on the suspected site and extent of the cancer, other tests might be performed, such as blood tests, endoscopic examinations, or chest X-rays, to rule out spread to other organs or to assess general health.
Treatment Modalities for Adenoid Cystic Carcinoma
The treatment of ACC is complex and often requires a multidisciplinary approach involving surgeons, oncologists, radiation oncologists, and other specialists. The primary goals of treatment are to achieve local control of the tumor, prevent recurrence, and manage any spread of the cancer. Due to the slow but persistent nature of ACC and its propensity for local recurrence and distant metastasis, treatment plans are often tailored to the individual patient and the specific characteristics of their tumor.
Surgical Management
Surgery is typically the cornerstone of ACC treatment, especially for localized disease. The extent of surgery depends on the tumor’s location, size, and involvement of surrounding structures.
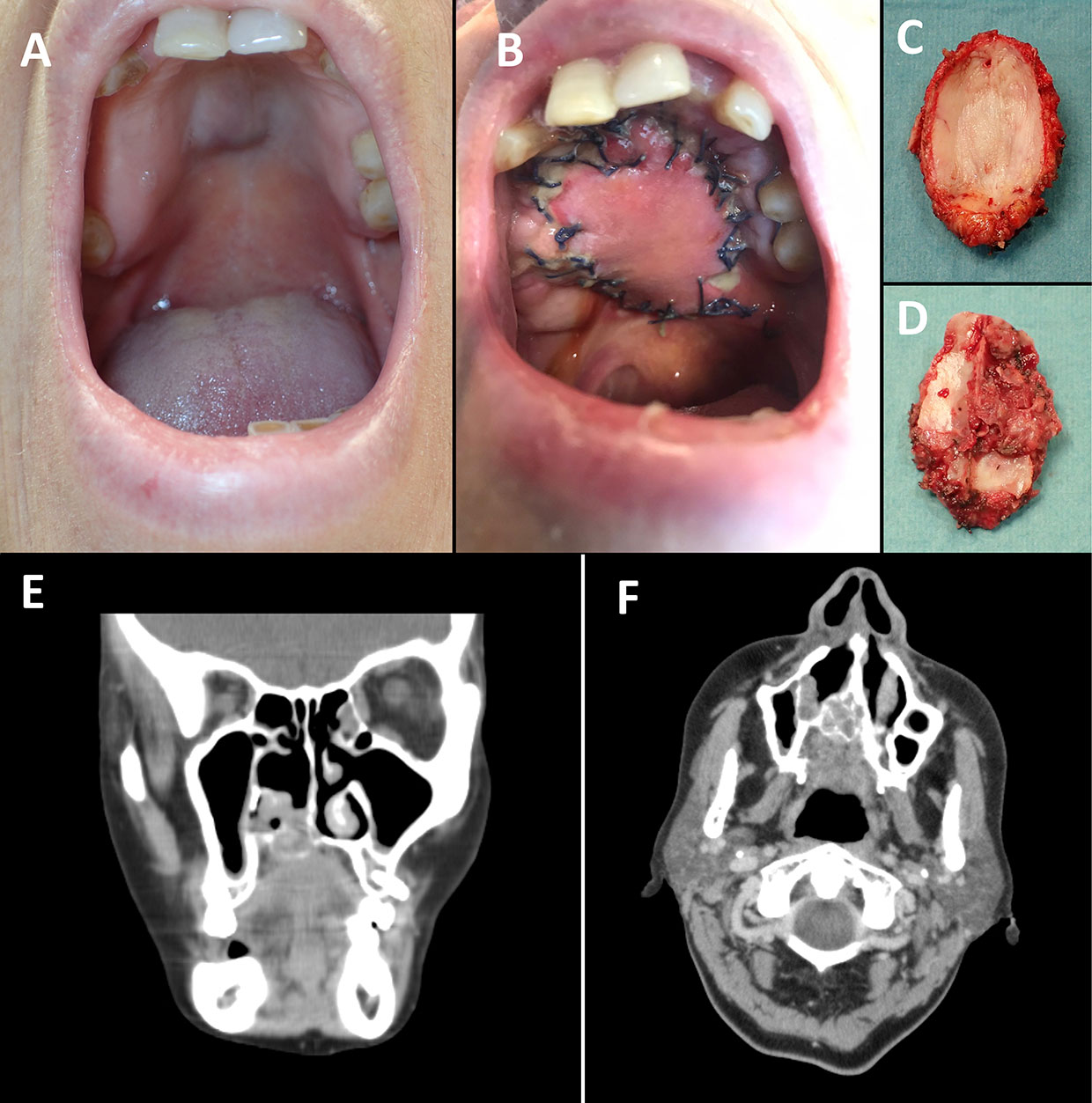
- Wide Local Excision: This involves surgically removing the tumor along with a margin of healthy tissue around it. The goal is to remove all visible cancerous cells and reduce the risk of local recurrence.
- Resection of Adjacent Structures: If the tumor has invaded nearby nerves, blood vessels, or organs, these structures may also need to be removed to achieve complete tumor clearance. For example, in salivary gland ACC, this might involve removal of portions of the facial nerve or nearby lymph nodes.
- Reconstructive Surgery: Following extensive tumor removal, reconstructive surgery may be necessary to restore function and cosmetic appearance. This can involve skin grafts, flaps of tissue from other parts of the body, or prosthetics.
Radiation Therapy
Radiation therapy plays a crucial role in ACC management, particularly when the tumor cannot be completely removed by surgery, or when there is a high risk of recurrence.
- Adjuvant Radiation Therapy: This is given after surgery to eliminate any microscopic cancer cells that may have been left behind. It is often recommended for tumors with high-risk features, such as positive surgical margins, perineural invasion, or a solid histological pattern.
- Primary Radiation Therapy: In cases where surgery is not feasible or is considered too risky, radiation therapy may be used as the primary treatment.
- Palliative Radiation Therapy: Radiation can also be used to manage symptoms caused by advanced or metastatic ACC, such as pain or bleeding.
External beam radiation therapy, using high-energy X-rays or protons, is the most common form of radiation used for ACC. The precise dosage and delivery schedule are carefully planned to maximize the tumor-killing effect while minimizing damage to surrounding healthy tissues.
Systemic Therapies (Chemotherapy and Targeted Therapy)
Systemic therapies, which circulate throughout the body, are generally less effective for ACC compared to surgery and radiation, especially in the early stages. However, they are considered for:
- Metastatic Disease: When ACC has spread to distant parts of the body (e.g., lungs, liver, bones), systemic therapies may be used to control the cancer’s growth and manage symptoms.
- Recurrent Disease: In cases of recurrent ACC that cannot be adequately treated with surgery or radiation.
Chemotherapy regimens for ACC often involve combinations of drugs. However, ACC is known to be relatively resistant to traditional chemotherapy. Research is ongoing to identify more effective chemotherapy agents and combinations.
Targeted therapies and immunotherapies are areas of active research for ACC. These therapies aim to specifically target the molecular pathways that drive cancer growth or to harness the body’s own immune system to fight the cancer. While some targeted agents have shown limited success in clinical trials, the field is evolving, and new agents are continuously being investigated.
Prognosis and Future Directions
The prognosis for adenoid cystic carcinoma is variable and depends on several factors, including the tumor’s location, stage at diagnosis, histological pattern, and the effectiveness of treatment. While ACC is known for its slow but persistent growth and a propensity for late recurrences, many patients can achieve long-term survival.
Factors Influencing Prognosis
- Location: ACC in the major salivary glands, particularly the parotid gland, generally has a better prognosis than ACC in the palate or lacrimal glands. Tumors in the head and neck region often have better outcomes than those in other sites.
- Stage at Diagnosis: As with most cancers, earlier stage at diagnosis is associated with a better prognosis.
- Histological Pattern: The solid pattern is often associated with a less favorable prognosis due to its more aggressive behavior and higher rates of metastasis.
- Perineural Invasion: The presence of perineural invasion is a significant negative prognostic factor, indicating a higher risk of local recurrence and distant spread.
- Surgical Margins: Achieving clear surgical margins (i.e., no cancer cells at the edge of the removed tissue) is critical for reducing the risk of recurrence.
- Distant Metastasis: The development of distant metastases significantly worsens the prognosis. The lungs are the most common site for ACC metastasis.
Recurrence and Long-Term Follow-Up
A notable characteristic of ACC is its tendency for late recurrence, even years after initial treatment. Therefore, patients diagnosed with ACC require long-term follow-up with their medical team. This typically involves regular physical examinations, imaging studies, and sometimes symptom monitoring to detect any signs of recurrence as early as possible. Early detection of recurrence can allow for timely intervention and potentially improve outcomes.
Research and Future Therapies
Ongoing research is crucial for improving the understanding and management of ACC. Key areas of investigation include:
- Molecular Biology: Identifying the specific genetic mutations and molecular pathways that drive ACC development and progression. This could lead to the development of more targeted therapies.
- Novel Therapies: Exploring new chemotherapy drugs, targeted agents (e.g., inhibitors of specific growth factor receptors or signaling pathways), and immunotherapies that may be effective against ACC.
- Improved Imaging Techniques: Developing more sensitive imaging methods to detect subtle signs of recurrence or metastatic disease earlier.
- Biomarker Discovery: Identifying biomarkers that can predict treatment response or prognosis, allowing for more personalized treatment strategies.
While ACC presents unique challenges due to its rarity and specific biological behavior, advancements in research and treatment offer hope for improved outcomes for patients. A comprehensive and multidisciplinary approach, coupled with diligent long-term follow-up, remains the standard of care for managing this complex malignancy.