High-grade dysplasia and carcinoma in situ (CIS) are terms that describe pre-cancerous changes in cells that have the potential to develop into invasive cancer. While they represent significant abnormalities, they are distinct from invasive cancer because the abnormal cells are confined to the original site of development and have not yet spread into surrounding tissues. Understanding the nuances between these two terms, their implications, and their management is crucial for effective medical intervention and patient prognosis.
Understanding Dysplasia and Carcinoma In Situ
At their core, both high-grade dysplasia and carcinoma in situ signify abnormal cellular growth. However, the terminology and precise definition can vary slightly depending on the organ system or tissue being discussed. Generally, dysplasia refers to a reversible or irreversible change in the size, shape, and organization of mature cells. It’s an intermediate stage between normal cellular development and cancer. Carcinoma in situ (CIS), on the other hand, is considered a more advanced form of pre-cancerous lesion. It denotes a more severe degree of cellular abnormality and is characterized by the presence of malignant-appearing cells that are confined to the epithelial layer of the tissue.
The Spectrum of Cellular Abnormalities
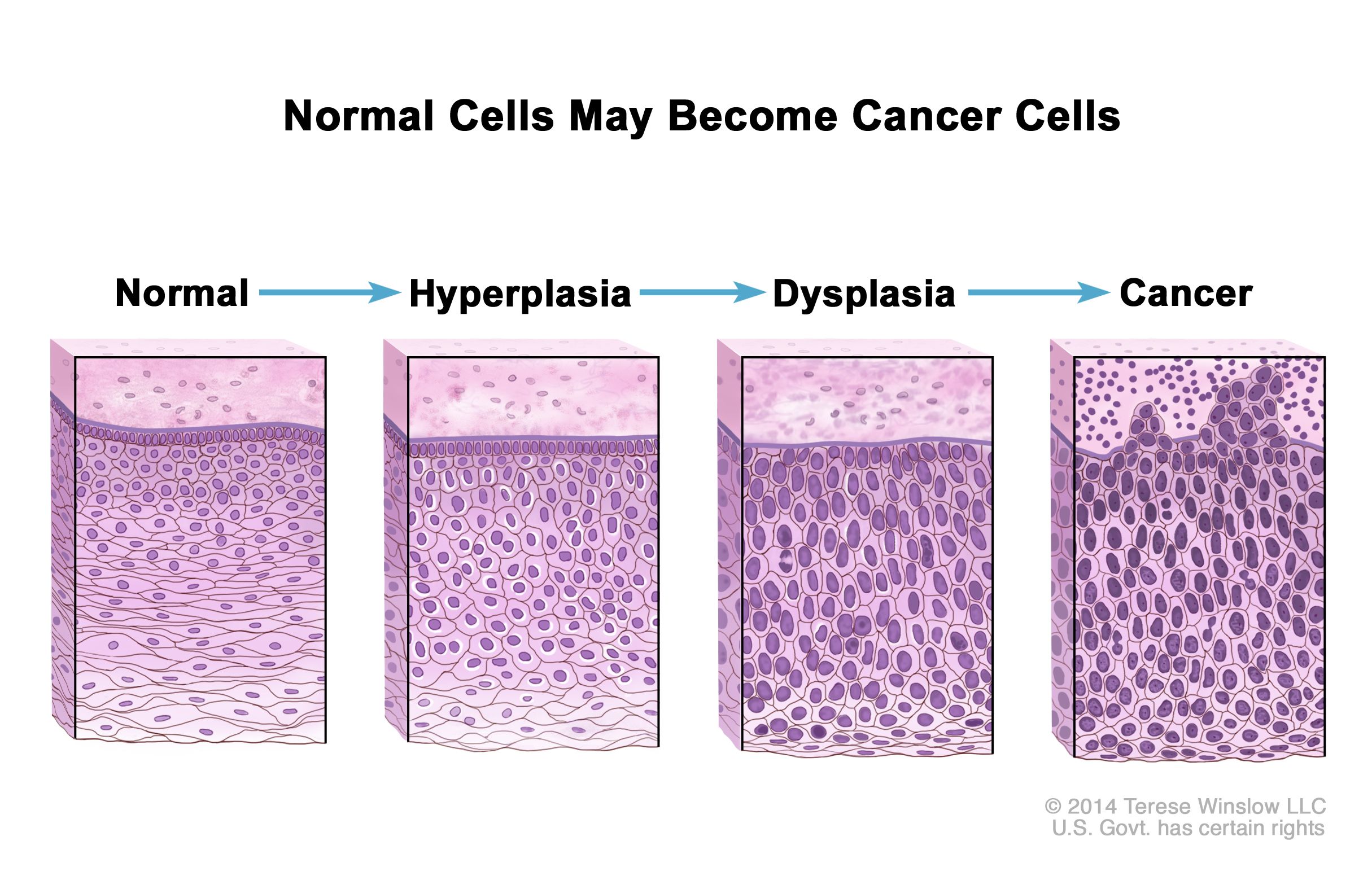
To fully grasp high-grade dysplasia and CIS, it’s helpful to consider the spectrum of cellular abnormalities. This spectrum typically begins with normal cells, progresses through mild or low-grade dysplasia, then to moderate or high-grade dysplasia, and finally, to carcinoma in situ.
Low-Grade Dysplasia
Low-grade dysplasia involves subtle changes in cell morphology. The cells may show some degree of nuclear enlargement or hyperchromasia (darker staining of the nucleus), but the overall cellular architecture remains relatively preserved. In many cases, low-grade dysplasia can regress spontaneously, meaning the cells can return to a normal appearance without intervention. However, it still warrants monitoring, as it can progress to higher grades.
High-Grade Dysplasia
High-grade dysplasia signifies more significant cellular abnormalities. The cells exhibit pronounced changes in their nucleus, which may be larger, irregularly shaped, and darker than normal. There can be a loss of cellular organization and differentiation, meaning the cells are less specialized and more primitive in appearance. Unlike low-grade dysplasia, high-grade dysplasia has a higher probability of progressing to carcinoma in situ and eventually to invasive cancer. Therefore, it typically requires more assertive management.
Carcinoma In Situ (CIS)
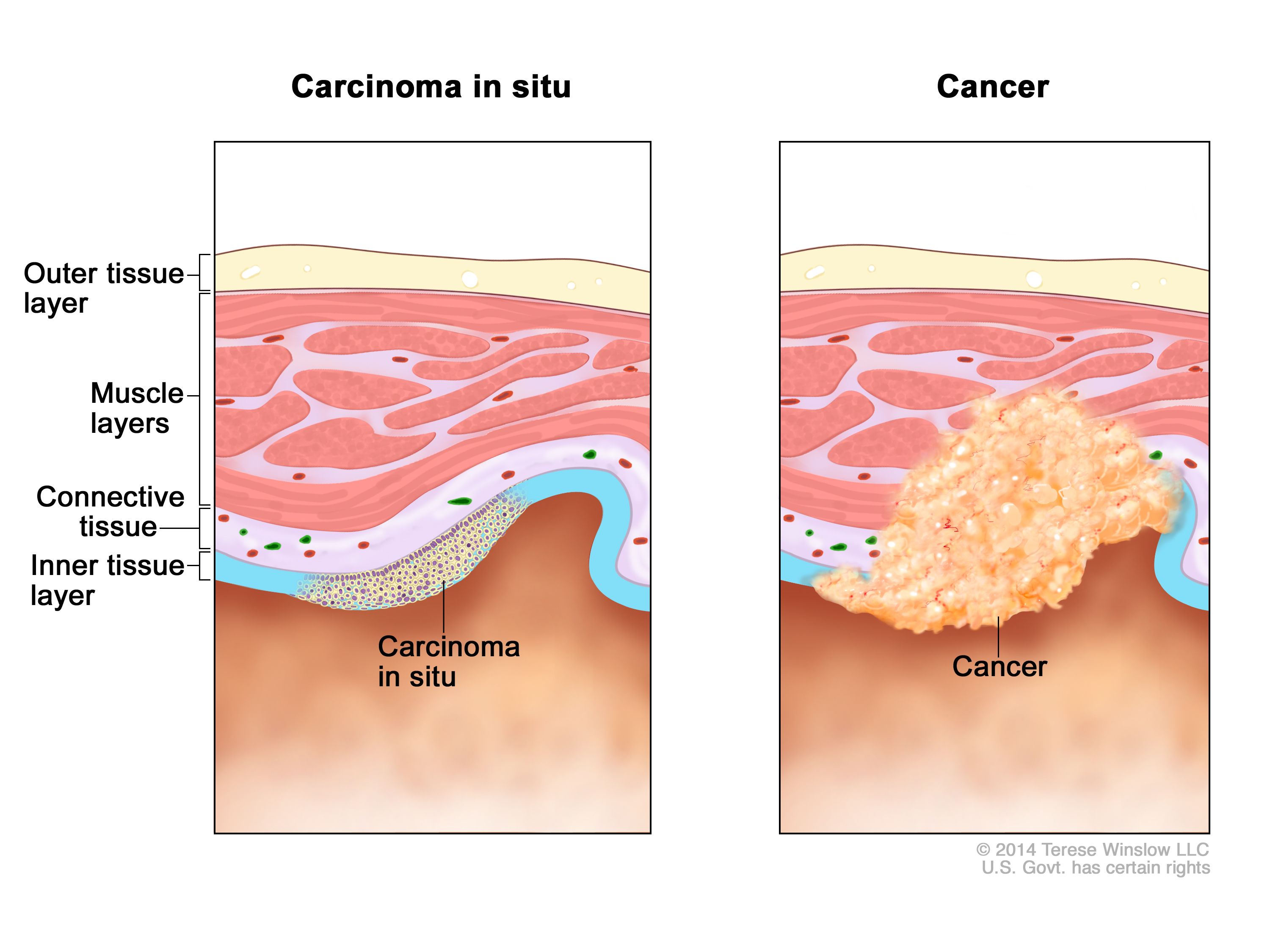
Carcinoma in situ represents the most advanced stage of pre-cancerous change. It is characterized by the presence of malignant cells that have a high degree of cellular atypia and have spread to involve the entire thickness of the epithelium but have not yet invaded the underlying basement membrane or connective tissue. In essence, it is a non-invasive cancer. The cells in CIS look very similar to those found in invasive cancer, but their inability to penetrate the basement membrane is the critical distinguishing factor. This “in situ” designation is pivotal, as it suggests that the abnormal cells are contained and have not yet acquired the ability to spread locally or to distant sites.
Key Differences and Similarities
The primary distinction between high-grade dysplasia and carcinoma in situ lies in the severity and the potential for progression. While both indicate significant cellular abnormalities, CIS is generally considered a more advanced and definitive precursor to invasive cancer. The cellular features in CIS are more overtly malignant than in high-grade dysplasia.
However, they share critical similarities:
- Pre-cancerous Nature: Both are stages that precede invasive cancer.
- Epithelial Confinement: The abnormal cells are generally confined to the epithelial layer.
- Potential for Progression: Both carry a risk of developing into invasive cancer if left untreated.
- Detection through Screening: Both are often detected through screening tests and biopsies.
The classification of a lesion as high-grade dysplasia or CIS often depends on subtle histological features and the specific criteria used by pathologists. Sometimes, the terms are used interchangeably or in conjunction, such as “high-grade dysplasia/carcinoma in situ,” to reflect this spectrum of abnormality.
Management and Treatment Approaches
The management of high-grade dysplasia and carcinoma in situ is tailored to the specific location of the lesion, its size, the patient’s overall health, and the potential for progression. The primary goal is to remove the abnormal cells to prevent the development of invasive cancer.
Diagnosis and Biopsy
The definitive diagnosis of high-grade dysplasia or CIS is made through a biopsy. This involves obtaining a tissue sample from the abnormal area, which is then examined under a microscope by a pathologist. The pathologist will assess the cellular morphology, architectural patterns, and the presence or absence of basement membrane invasion to determine the grade of dysplasia or if it is carcinoma in situ.

Imaging techniques may be used to identify suspicious areas for biopsy, depending on the affected organ. For example, colposcopy with acetic acid and Lugol’s iodine is used to visualize cervical dysplasia, and endoscopy with biopsies is common for esophageal or gastric CIS.
Treatment Modalities
The treatment strategy is designed to eliminate the affected cells while preserving organ function as much as possible. Common treatment modalities include:
Local Excision or Resection
This involves surgically removing the abnormal tissue. The extent of the excision depends on the size and location of the lesion. For example, a cone biopsy is often performed for cervical CIS, removing a cone-shaped piece of the cervix containing the abnormal cells. Local excision is highly effective for CIS and often leads to a cure.
Ablative Therapies
In certain situations, less invasive ablative therapies can be used to destroy the abnormal cells. These methods aim to eliminate the tissue without requiring surgical excision. Examples include:
- Cryotherapy: Freezing the abnormal tissue.
- Laser Therapy: Using a laser beam to vaporize the abnormal cells.
- Radiofrequency Ablation (RFA): Using heat generated by radiofrequency waves to destroy the abnormal tissue.
- Endoscopic Mucosal Resection (EMR) / Endoscopic Submucosal Dissection (ESD): These endoscopic techniques are used for CIS in the gastrointestinal tract, allowing for the removal of superficial lesions.
Surveillance and Follow-Up
After treatment, regular follow-up appointments and screening tests are crucial to monitor for any recurrence of the dysplasia or CIS, or the development of new abnormalities. The frequency and type of follow-up will depend on the initial diagnosis, treatment received, and the individual patient’s risk factors.
In cases where the lesion is very small and has very low malignant potential, and in specific locations where it is highly likely to regress, a period of close surveillance without immediate intervention might be considered. However, this is a decision made on a case-by-case basis by a medical professional.
Implications and Prognosis
The prognosis for individuals diagnosed with high-grade dysplasia or carcinoma in situ is generally excellent, provided it is detected and treated appropriately. The key advantage of these conditions is that they are non-invasive, meaning they are confined to their original tissue layer and have not yet acquired the ability to spread.
Preventing Invasive Cancer
The primary implication of diagnosing high-grade dysplasia or CIS is the opportunity to prevent the development of invasive cancer. By intervening at this pre-cancerous stage, clinicians can effectively eliminate the risk of the disease progressing to a more dangerous and potentially life-threatening form. This highlights the critical importance of early detection and screening programs for various cancers.
Risk Factors and Recurrence
Certain factors can increase the risk of developing high-grade dysplasia or CIS, or the risk of recurrence after treatment. These can include:
- Human Papillomavirus (HPV) Infection: A significant risk factor for cervical, anal, and oropharyngeal CIS.
- Age: Risk can increase with age.
- Lifestyle Factors: Smoking, excessive alcohol consumption, and certain dietary habits can play a role in some types of CIS.
- Immunosuppression: Individuals with weakened immune systems may be at higher risk.
Understanding these risk factors allows for targeted screening and preventative measures.
Long-Term Outlook
With successful treatment and appropriate follow-up, the long-term outlook for patients with high-grade dysplasia and CIS is very positive. The vast majority of individuals can expect to live a normal lifespan without developing invasive cancer. However, ongoing vigilance is essential, as some individuals may develop new pre-cancerous lesions or even invasive cancer later in life, particularly if underlying risk factors are not addressed.
The distinction between high-grade dysplasia and carcinoma in situ, while sometimes subtle, carries significant weight in clinical decision-making. Both represent critical junctures in the pathway to cancer, offering a vital window for intervention and the preservation of health. Continued advancements in diagnostic tools and treatment techniques further enhance the ability to manage these conditions effectively, underscoring the success of proactive healthcare in preventing cancer.