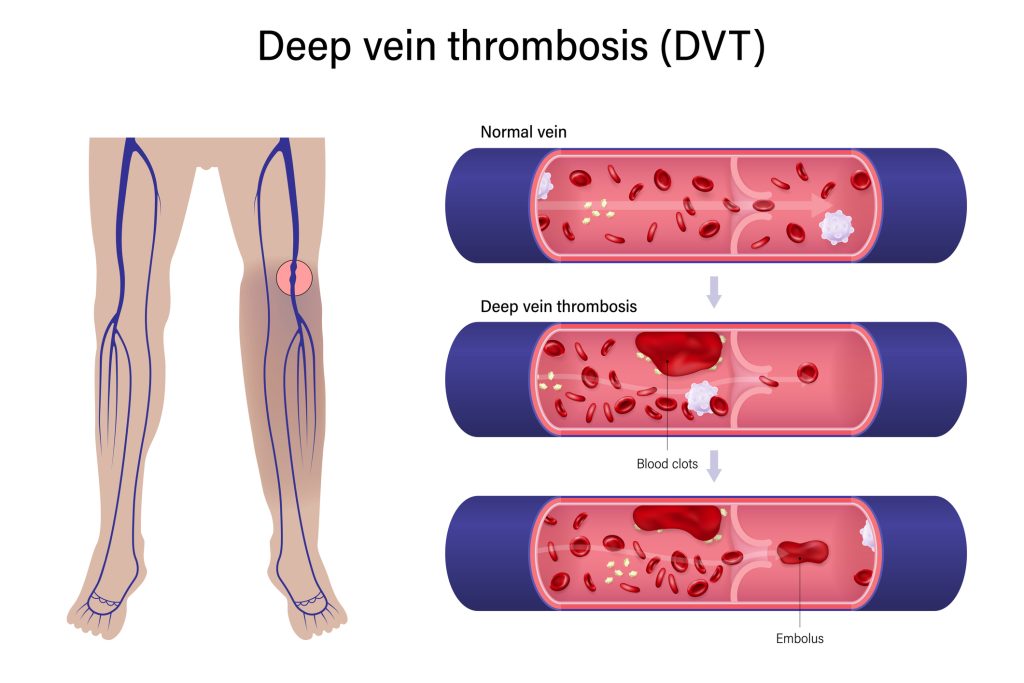
Deep Vein Thrombosis (DVT) prophylaxis refers to the preventative measures taken to reduce the risk of developing blood clots in deep veins, most commonly in the legs. These clots, if they dislodge and travel to the lungs, can cause a pulmonary embolism (PE), a potentially life-threatening condition. Understanding DVT prophylaxis is crucial across various medical settings, from hospital recovery to long-term care, and even for individuals with specific risk factors.
Understanding Deep Vein Thrombosis (DVT)
Deep Vein Thrombosis occurs when a blood clot, or thrombus, forms in one or more of the deep veins in the body. The vast majority of DVTs occur in the legs, but they can also form in the arms or pelvis. The underlying mechanism of DVT formation is often attributed to Virchow’s triad, a set of three factors that contribute to thrombosis:

- Venous Stasis: This refers to the slowing or cessation of blood flow. Immobility is a primary driver of venous stasis. When a person is bedridden due to illness, surgery, or long periods of travel, the muscles in the legs are not contracting regularly to help pump blood back to the heart. This stagnant blood is more prone to clotting.
- Endothelial Injury: Damage to the inner lining of blood vessels can trigger the clotting cascade. This can occur due to direct trauma, inflammation, surgery, or the presence of certain medical devices like catheters. Even subtle endothelial dysfunction can increase DVT risk.
- Hypercoagulability: This refers to an increased tendency of the blood to clot. This can be inherited (genetic predisposition) or acquired due to conditions such as cancer, pregnancy, hormonal therapy (like estrogen), inflammatory bowel disease, or certain medications.
Symptoms and Diagnosis of DVT
While many DVTs are asymptomatic, particularly smaller ones, recognized symptoms can include:
- Swelling: Often unilateral, affecting one leg more than the other.
- Pain or Tenderness: Typically felt in the calf or thigh, sometimes described as a cramping or aching sensation.
- Warmth: The affected area may feel warmer to the touch than the surrounding skin.
- Redness or Discoloration: The skin over the affected vein may appear reddish or purplish.
- Visible Superficial Veins: Veins near the surface of the skin may become more prominent.
Diagnosing DVT typically involves a combination of clinical assessment and diagnostic imaging. The Wells score, a clinical prediction rule, helps stratify patients into low, moderate, or high risk for DVT. If the clinical suspicion is moderate to high, further investigations are usually performed. The most common diagnostic tool is:
- Doppler Ultrasound: This non-invasive imaging technique uses sound waves to visualize blood flow in the veins. It can detect the presence of a clot and its location.
Other diagnostic methods, though less common for routine DVT diagnosis, may include:
- D-dimer Test: A blood test that measures a substance released when a blood clot breaks down. A negative D-dimer in a low-risk patient can help rule out DVT, but it is not specific and can be elevated in other conditions.
- Venography: An invasive procedure where contrast dye is injected into a vein, and X-rays are taken. This is considered the gold standard but is rarely used due to its risks and the availability of ultrasound.
Pillars of DVT Prophylaxis
DVT prophylaxis aims to interrupt the mechanisms leading to clot formation, primarily by addressing venous stasis and hypercoagulability. The approach to prophylaxis is typically tailored to the individual patient’s risk factors and the specific clinical context. The main strategies can be broadly categorized into mechanical and pharmacological methods.
Mechanical Prophylaxis
Mechanical methods aim to improve blood flow in the legs and reduce venous stasis without the use of medications. These are often used for patients who have contraindications to anticoagulation or as an adjunct to pharmacological therapy.
- Early Mobilization and Ambulation: For most patients, the simplest and most effective form of prophylaxis is to encourage movement as soon as it is medically safe. Frequent walking, leg exercises while in bed, and changing positions can significantly improve venous return.
- Graduated Compression Stockings (GCS): These specially designed stockings apply graduated pressure to the legs, starting with the highest pressure at the ankle and decreasing as the stocking moves up the leg. This compression helps to narrow the veins and improve blood flow, reducing venous stasis. GCS are particularly useful for patients who are immobile. However, their effectiveness can be limited if not fitted properly or if the patient cannot tolerate them due to discomfort or skin integrity issues.
- Intermittent Pneumatic Compression (IPC) Devices: These devices consist of inflatable sleeves or boots that are wrapped around the legs. An external pump inflates and deflates the sleeves intermittently, creating a squeezing action that mimics the muscle contractions of walking. This cyclical compression helps to move blood from the deep veins towards the heart, thereby reducing stasis and the risk of clot formation. IPC devices are frequently used in post-operative patients or those with significant immobility.
Pharmacological Prophylaxis
Pharmacological prophylaxis involves the use of medications that interfere with the blood clotting process. These agents are typically anticoagulants, which prevent the formation of new clots and slow the growth of existing ones, allowing the body’s natural mechanisms to break down the clot over time.
- Unfractionated Heparin (UFH): This is a traditional anticoagulant that works by enhancing the activity of antithrombin III, a natural anticoagulant in the body. UFH can be administered intravenously or subcutaneously. It has a rapid onset of action but a short half-life, requiring frequent monitoring of its anticoagulant effect (usually via activated partial thromboplastin time or aPTT). Due to the need for monitoring and the risk of heparin-induced thrombocytopenia (HIT), a serious immune-mediated complication, its use has declined in favor of newer agents for routine prophylaxis.
- Low Molecular Weight Heparins (LMWHs): Examples include enoxaparin, dalteparin, and tinzaparin. LMWHs are derived from unfractionated heparin but have a more predictable pharmacokinetic profile, a longer half-life, and generally do not require routine monitoring of coagulation parameters. They are administered subcutaneously and are a cornerstone of DVT prophylaxis in many hospital settings, particularly for patients undergoing surgery or with moderate to high risk.
- Direct Oral Anticoagulants (DOACs): This newer class of anticoagulants includes direct thrombin inhibitors (e.g., dabigatran) and Factor Xa inhibitors (e.g., rivaroxaban, apixaban, edoxaban). DOACs offer the advantage of oral administration, eliminating the need for injections and most routine laboratory monitoring. They have proven to be effective and safe for DVT prophylaxis in various scenarios, including post-orthopedic surgery and in patients with medical conditions associated with increased VTE risk. The choice of DOAC and its specific indication depends on the clinical guidelines and patient factors.
- Fondaparinux: This is a synthetic pentasaccharide that selectively inhibits Factor Xa. It is administered subcutaneously and offers a predictable pharmacokinetic profile without the need for routine monitoring. Fondaparinux is often used in patients who have contraindications to heparin or LMWHs, particularly in orthopedic surgery.
- Warfarin: This is an older oral anticoagulant that works by inhibiting the synthesis of vitamin K-dependent clotting factors. Warfarin has a slow onset of action and requires regular monitoring of the international normalized ratio (INR) to ensure therapeutic anticoagulation and minimize bleeding risk. While historically a mainstay for long-term anticoagulation, its use for short-term DVT prophylaxis has largely been supplanted by LMWHs and DOACs due to its monitoring requirements and interactions with diet and other medications.
Risk Stratification and Tailoring Prophylaxis
The decision to initiate DVT prophylaxis and the choice of method are guided by a comprehensive assessment of a patient’s risk factors for VTE. Healthcare providers utilize risk assessment models and clinical judgment to stratify patients and select the most appropriate preventative strategy.
Risk Factors for DVT
A multitude of factors can increase an individual’s risk of developing DVT. These are often grouped into general risk factors and those specific to particular medical or surgical situations.
General Risk Factors:
- Age: Risk increases with age, particularly over 60.
- Previous VTE: A history of DVT or PE significantly increases the risk of recurrence.
- Immobility: Prolonged bed rest, long travel, or casting of a limb.
- Malignancy: Active cancer or treatment for cancer.
- Hormonal Therapy: Estrogen-containing oral contraceptives or hormone replacement therapy.
- Pregnancy and Postpartum Period: Increased clotting risk during and immediately after childbirth.
- Obesity: Higher body mass index is associated with increased risk.
- Smoking: A contributing factor to endothelial dysfunction.
- Inflammatory Conditions: Such as inflammatory bowel disease.
- Inherited Thrombophilias: Genetic conditions that predispose to clotting.
Medical and Surgical Risk Factors:
- Major Surgery: Especially orthopedic surgery (hip or knee replacement), abdominal surgery, and cancer surgery.
- Trauma: Fractures, particularly of the pelvis or lower extremities.
- Acute Medical Illness: Congestive heart failure, severe respiratory disease, stroke, or acute infection requiring hospitalization.
- Central Venous Catheters: Placement of these devices can increase the risk of upper extremity DVT.
Risk Assessment Models
Various validated risk assessment tools exist to help clinicians quantify a patient’s VTE risk. For surgical patients, the Caprini score is commonly used, which assigns points based on numerous risk factors. For medical patients, tools like the IMPROVE VTE risk score are employed. These scores help guide the decision-making process regarding the intensity and duration of prophylaxis.
Tailoring Prophylaxis
The optimal prophylaxis strategy involves balancing the risk of VTE against the risk of bleeding complications associated with anticoagulant therapy.
- Low-Risk Patients: May require no specific prophylaxis beyond early mobilization.
- Moderate-Risk Patients: Often benefit from mechanical prophylaxis (GCS or IPC) or pharmacological prophylaxis with LMWH or a DOAC, depending on the clinical scenario and local guidelines.
- High-Risk Patients: Typically require a combination of mechanical and pharmacological prophylaxis, with close monitoring of their response and potential complications.
For instance, a patient undergoing hip replacement surgery is at very high risk of DVT and will usually receive both LMWH or a DOAC and mechanical prophylaxis with GCS or IPC for a specified duration postoperatively. Conversely, a young, healthy individual who has undergone a minor surgical procedure and is expected to ambulate quickly might only need encouragement for early mobility.
Complications and Monitoring
While DVT prophylaxis is a critical component of patient care, it is not without potential risks and requires careful monitoring.
Bleeding Risk
The primary complication of pharmacological DVT prophylaxis, particularly anticoagulation, is bleeding. The risk of bleeding varies depending on the specific anticoagulant used, the dose, the patient’s underlying health status (e.g., renal or liver function), and concomitant medications. Healthcare providers must carefully weigh the benefits of preventing VTE against the potential harms of bleeding. Signs of bleeding can range from minor bruising and nosebleeds to more serious gastrointestinal bleeding or intracranial hemorrhage.
Other Complications
- Heparin-Induced Thrombocytopenia (HIT): A rare but serious immune-mediated reaction to heparin and LMWHs that paradoxically increases the risk of clotting.
- Skin Necrosis and Ulceration: Can occur with prolonged use of compression stockings or IPC devices, especially in patients with peripheral vascular disease.
- Pain and Discomfort: Some patients may experience discomfort or pain from compression devices or injections.

Monitoring Strategies
Effective monitoring of DVT prophylaxis involves several aspects:
- Clinical Assessment: Regular observation of patients for signs and symptoms of VTE (swelling, pain, redness) and bleeding.
- Laboratory Monitoring: While routine monitoring is often not required for LMWHs and DOACs, specific laboratory tests may be necessary for unfractionated heparin (aPTT) or for patients with impaired renal or liver function.
- Adherence and Tolerance: Ensuring patients are adhering to prescribed prophylaxis and tolerating the treatment without undue side effects.
- Reassessment: Continuously reassessing a patient’s risk of VTE and bleeding throughout their hospital stay or treatment period, as risk factors can change.
In conclusion, DVT prophylaxis is a multifaceted approach to preventing potentially serious blood clots. It involves a thorough understanding of the pathophysiology of DVT, careful risk stratification of patients, and the judicious application of mechanical and pharmacological interventions. By employing these strategies, healthcare professionals aim to significantly reduce the incidence of DVT and its life-threatening complications, ensuring better patient outcomes and promoting recovery.