Bullae, in the context of lung health, are abnormal air-filled sacs that can develop within the lung tissue. These are not simply small pockets of air but rather distinct, visible entities that represent a significant pathological change. Understanding what bullae are, how they form, and their implications for respiratory function is crucial for appreciating various lung conditions and their management. While the term “bullae” might sound technical, its implications are directly relevant to the broader field of health monitoring and the potential for advanced diagnostic tools, particularly those with remote sensing capabilities.
The Nature and Formation of Pulmonary Bullae
Pulmonary bullae are characterized by their thin walls and their presence within the lung parenchyma, often replacing healthy lung tissue. They can vary in size, from a few millimeters to several centimeters in diameter. Unlike blebs, which are subpleural, bullae are located entirely within the visceral pleura and extend into the lung’s interstitial space.
Etiology of Bullae Formation
The primary driver behind bullae formation is the destruction of alveolar walls, the tiny air sacs where gas exchange occurs. This destruction leads to the merging of multiple alveoli into larger, abnormal air spaces. The most common underlying condition associated with bullae is emphysema, a progressive and irreversible lung disease that is a major component of Chronic Obstructive Pulmonary Disease (COPD).
Several factors contribute to the damage of alveolar walls and the subsequent development of bullae:
- Cigarette Smoking: This is by far the leading cause of emphysema and, consequently, bullae. The chemicals in cigarette smoke trigger inflammation in the lungs, leading to the release of enzymes that break down elastin, a critical protein for lung elasticity. Over time, this breakdown weakens and destroys alveolar walls.
- Alpha-1 Antitrypsin Deficiency: This is a genetic disorder that can lead to early-onset emphysema, even in individuals who have never smoked. Alpha-1 antitrypsin is a protein that protects the lungs from damage by certain enzymes. In individuals with this deficiency, the protective mechanism is compromised, making the lungs more susceptible to damage.
- Environmental Pollutants: Long-term exposure to air pollution, occupational dusts, and chemical fumes can also contribute to lung inflammation and damage, potentially leading to bullae formation.
- Aging: While not a direct cause, the natural aging process can lead to some degree of lung tissue degradation, which may exacerbate the effects of other contributing factors.
The process of bullae formation is often insidious, developing over many years. As alveolar walls are destroyed, the lungs lose their natural elasticity, making it harder to exhale. The enlarged air spaces, or bullae, become inefficient at gas exchange, meaning less oxygen can enter the bloodstream and less carbon dioxide can be removed. This leads to symptoms like shortness of breath and reduced exercise tolerance.
Pathological Characteristics
From a microscopic perspective, bullae are characterized by:
- Destruction of Alveolar Septa: The fine walls separating the alveoli are broken down, leading to larger, irregular air spaces.
- Loss of Elastic Recoil: The elasticity of the lung tissue is significantly diminished, as the intricate network of elastic fibers is damaged.
- Inflammation: Chronic inflammation is a common feature, further perpetuating the cycle of tissue destruction.
- Thinned Walls: The walls of mature bullae are often very thin, making them prone to rupture.
The presence of bullae can significantly impact lung function by reducing the overall surface area available for gas exchange and trapping air within the lungs, a phenomenon known as air trapping. This mechanical inefficiency makes breathing a more arduous task.
The Clinical Significance of Pulmonary Bullae
The clinical significance of bullae lies primarily in their association with debilitating lung diseases and their potential to cause acute complications. Their detection and understanding are vital for diagnosis, prognosis, and treatment planning.
Symptoms Associated with Bullae
The symptoms experienced by individuals with bullae are largely dependent on their size, number, and the underlying condition, most commonly emphysema. However, some common manifestations include:
- Dyspnea (Shortness of Breath): This is the hallmark symptom. Initially, it may only occur with exertion, but as bullae progress, it can become noticeable even at rest. The reduced efficiency of gas exchange and the mechanical limitations of air trapping contribute to this feeling of breathlessness.
- Chronic Cough: Often a persistent cough, which may be productive of mucus, is present.
- Wheezing: A whistling sound during breathing can occur due to narrowed airways.
- Chest Tightness: A constricting sensation in the chest.
- Fatigue: The reduced oxygen supply to the body can lead to generalized tiredness and lack of energy.
- Weight Loss: In severe cases, the increased effort of breathing can lead to significant caloric expenditure, contributing to unintentional weight loss.
Complications of Bullae

Beyond the chronic symptoms, bullae can lead to several acute and potentially life-threatening complications:
- Pneumothorax: This is a critical complication where a bulla ruptures, allowing air to leak into the pleural space (the space between the lung and the chest wall). This air buildup collapses the lung, leading to sudden, severe shortness of breath and chest pain. Spontaneous pneumothorax, often associated with bullae, can occur without any apparent injury.
- Hemoptysis (Coughing up Blood): While less common, rupture of blood vessels within the bullae or surrounding inflamed tissue can lead to coughing up blood.
- Secondary Infection: The stagnant air within bullae can be a breeding ground for bacteria, leading to recurrent lung infections.
- Air Embolism: In rare cases, air can enter the bloodstream through ruptured bullae, leading to a serious condition called air embolism.
The development of complications underscores the importance of early detection and appropriate management of conditions that lead to bullae.
Diagnostic Modalities
Identifying pulmonary bullae typically involves a combination of clinical assessment and imaging techniques.
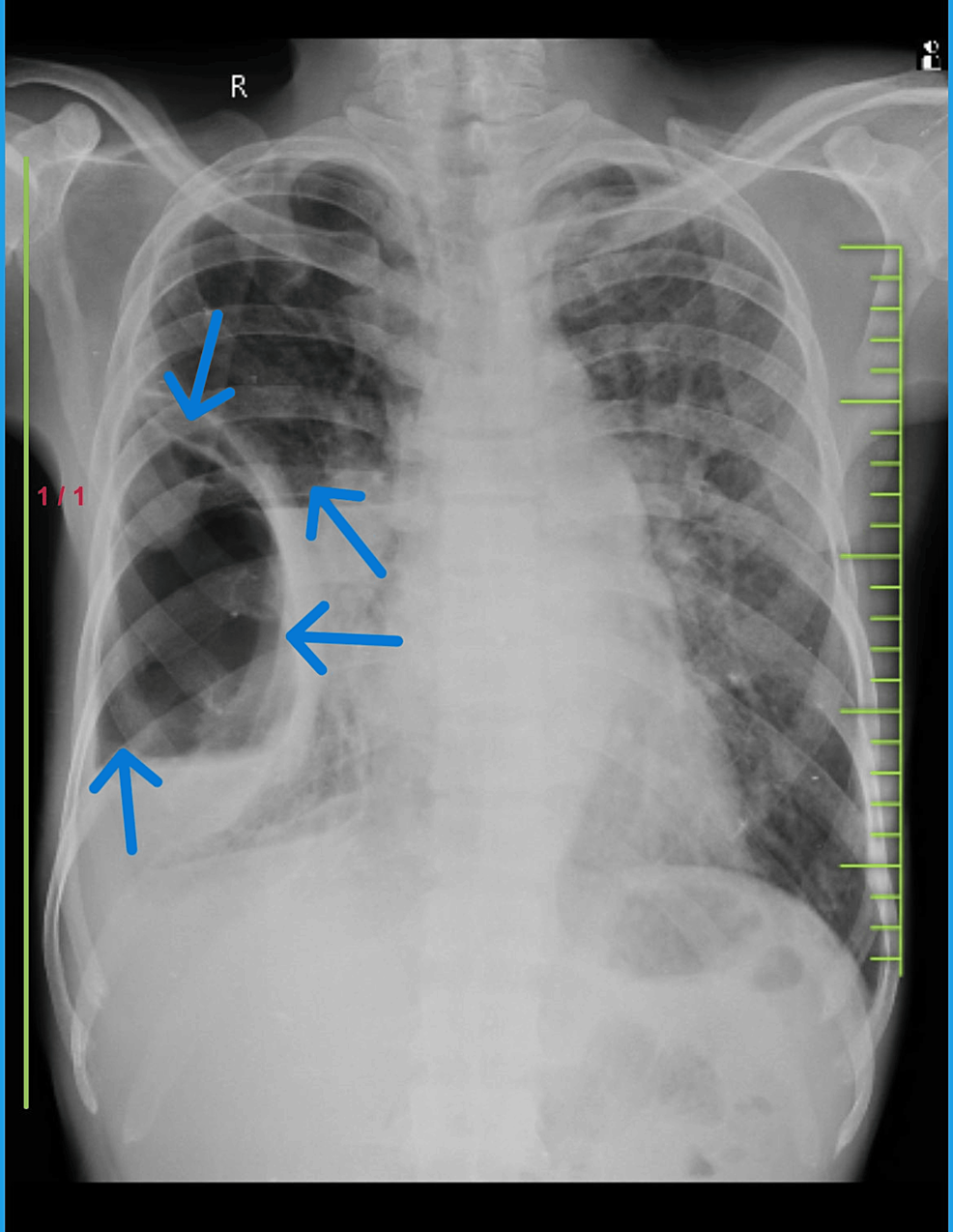
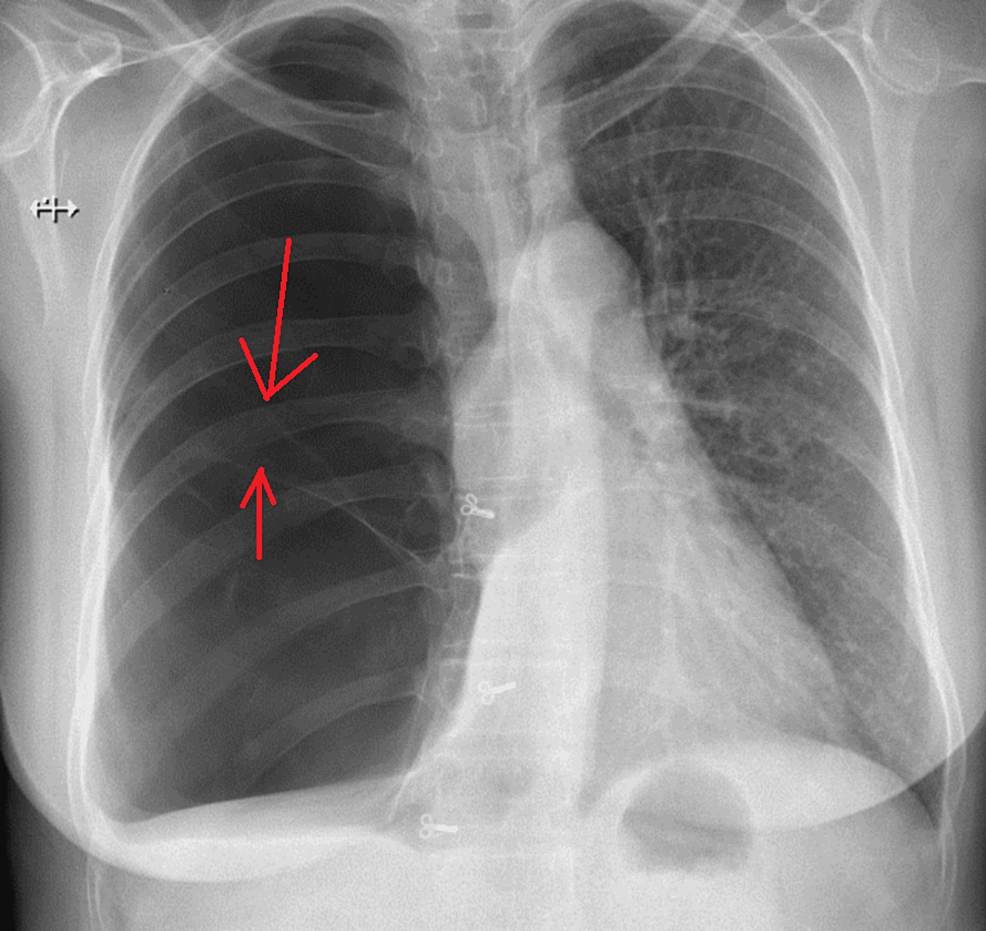
- Chest X-ray: A standard chest X-ray can often reveal the presence of large bullae as lucent (dark) areas within the lung fields, often with flattened diaphragms and hyperinflated lungs. However, smaller bullae or those obscured by other lung structures may not be visible.
- Computed Tomography (CT) Scan: A CT scan of the chest provides much more detailed images of the lungs and is the gold standard for detecting and characterizing bullae. It can precisely delineate their size, location, number, and the extent of associated lung damage. High-resolution CT (HRCT) is particularly useful for assessing the fine details of lung parenchyma.
- Pulmonary Function Tests (PFTs): While PFTs do not directly visualize bullae, they are essential for assessing the severity of lung impairment. Tests like spirometry can measure lung volumes and airflow rates, revealing obstructive patterns consistent with emphysema and the presence of bullae.
The precise characterization of bullae through CT scans is crucial for guiding treatment decisions. For instance, the size and location of bullae can influence the suitability of surgical interventions.
Management and Treatment Strategies for Bullae
The management of pulmonary bullae is multifaceted, focusing on slowing disease progression, managing symptoms, and preventing or treating complications. The approach depends heavily on the underlying cause, the extent of lung damage, and the patient’s overall health.
Medical Management
For bullae associated with COPD and emphysema, medical management is the cornerstone of care:
- Smoking Cessation: This is the single most important intervention to prevent further lung damage and slow the progression of emphysema and bullae formation.
- Bronchodilators: Medications like short-acting and long-acting beta-agonists (LABAs) and anticholinergics help to relax the muscles around the airways, making breathing easier and reducing air trapping.
- Inhaled Corticosteroids: These can help reduce inflammation in the airways, particularly in patients with frequent exacerbations.
- Pulmonary Rehabilitation: This is a comprehensive program that includes exercise training, education, and nutritional counseling. It helps patients improve their exercise capacity, reduce symptoms, and enhance their quality of life.
- Oxygen Therapy: For patients with severe hypoxemia (low blood oxygen levels), supplemental oxygen therapy can improve oxygenation and reduce the strain on the heart.
- Antibiotics and Expectorants: These may be used to manage infectious exacerbations or to help clear mucus.
Surgical Interventions
In select cases, surgical options may be considered for patients with symptomatic bullae that significantly impair lung function.
- Lung Volume Reduction Surgery (LVRS): This procedure involves surgically removing the most diseased and hyperinflated parts of the lung, including large bullae. The goal is to reduce lung volume, improve the elastic recoil of the remaining lung tissue, and enhance the efficiency of breathing. LVRS is typically considered for patients with severe emphysema and bullae in specific locations who have not responded adequately to medical management. Careful patient selection is crucial for success.
- Bullectomy: This is a more targeted surgical procedure that involves removing individual, large, symptomatic bullae. It is often performed via video-assisted thoracoscopic surgery (VATS), which involves smaller incisions and a quicker recovery. Like LVRS, bullectomy aims to improve lung mechanics and alleviate symptoms.
Emerging Technologies and Future Directions
The understanding of lung diseases like emphysema and the pathology of bullae is continually evolving, paving the way for innovative diagnostic and therapeutic approaches.
- Advanced Imaging Techniques: While CT scans are currently the standard, ongoing research into novel imaging modalities may offer even greater precision in characterizing lung structures and identifying early signs of disease. This could include functional imaging techniques that assess gas exchange efficiency in specific lung regions.
- Minimally Invasive Interventions: Beyond VATS, there is a growing interest in even less invasive techniques for lung volume reduction. These include endoscopic procedures that use valves or coils to collapse diseased lung segments or bullae, offering a less risky alternative to traditional surgery for some patients.
- Biomarkers and Personalized Medicine: Research into biomarkers could help identify individuals at higher risk for developing bullae or predict their response to specific treatments. This would enable more personalized and effective management strategies.
- Remote Sensing and Monitoring: The potential for remote sensing technologies to contribute to lung health is significant. Imagine wearable sensors that can continuously monitor respiratory rate, oxygen saturation, and even subtle changes in lung mechanics. Data from such devices, potentially integrated with advanced analytical algorithms, could provide early warnings of exacerbations or changes in bullae status, allowing for timely intervention. Furthermore, aerial remote sensing technologies, when applied with specialized spectral analysis, could theoretically offer insights into broader environmental factors impacting lung health in communities, although direct detection of individual bullae from the air is not currently feasible. The focus here is on the indirect impact of environmental conditions that contribute to lung disease, which these technologies can help map and monitor.
The ongoing advancements in medical science and technology offer hope for improved diagnosis, more effective treatments, and a better quality of life for individuals affected by pulmonary bullae and the conditions that cause them.