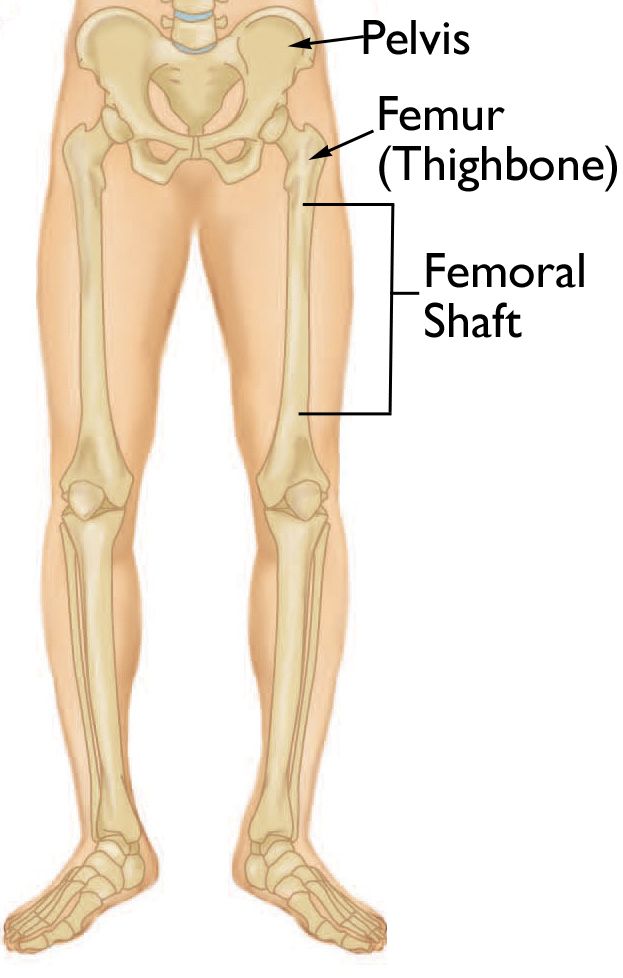
The femur, or thigh bone, is the longest, strongest, and heaviest bone in the human body. Its robust nature is crucial for bearing the weight of our torso and enabling locomotion. Consequently, a fracture of the femur is a significant injury, demanding immediate medical attention and a comprehensive treatment and rehabilitation plan. Understanding the anatomy, the mechanisms of injury, the immediate consequences, and the long-term recovery process is vital for anyone facing this challenging situation.
Anatomy and Biomechanics of the Femur
The femur extends from the hip joint to the knee joint. Its proximal end articulates with the pelvis at the acetabulum, forming the hip joint, a ball-and-socket joint that allows for a wide range of motion. The distal end articulates with the tibia and patella at the knee joint, forming the hinge mechanism that allows for flexion and extension of the leg.
The femur’s strength lies in its dense cortical bone and its inherent curvature, which helps distribute weight-bearing forces. It serves as the anchor point for powerful muscles of the thigh, including the quadriceps femoris anteriorly and the hamstrings posteriorly. These muscles play a critical role in walking, running, jumping, and maintaining balance. The femur also houses the bone marrow, responsible for producing blood cells.
Types of Femur Fractures
Femur fractures can occur in several locations, each with distinct characteristics and treatment implications:
-
Proximal Femur Fractures: These occur in the upper part of the femur, near the hip joint. They are further classified into:
- Intracapsular Fractures: These occur within the hip joint capsule and often involve the femoral neck. They are more common in older adults with osteoporosis and can disrupt the blood supply to the femoral head, potentially leading to avascular necrosis.
- Extracapsular Fractures: These occur outside the hip joint capsule, typically in the intertrochanteric region (between the greater and lesser trochanters) or subtrochanteric region (below the lesser trochanter). These are often caused by higher-energy trauma and tend to have better blood supply.
-
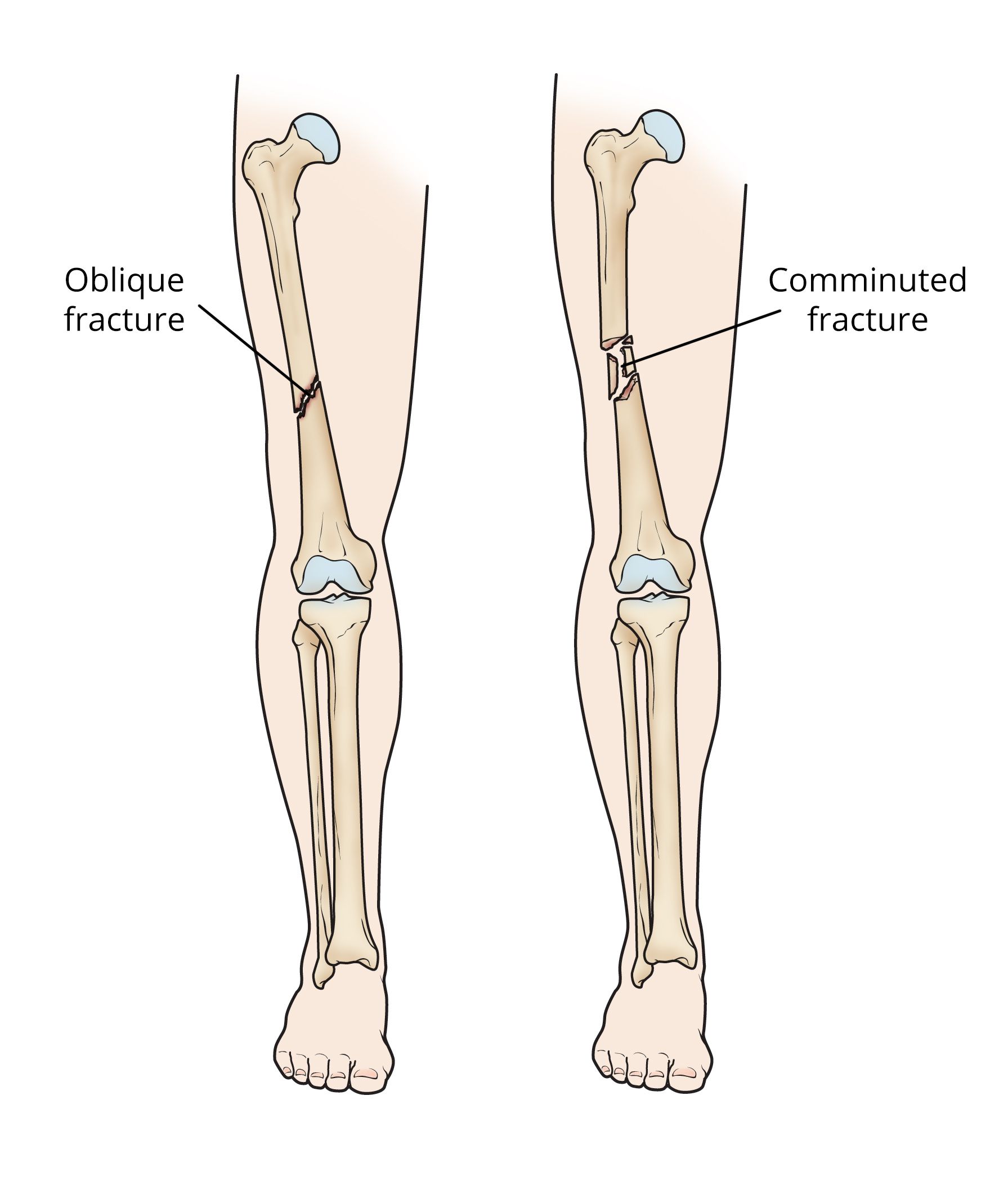
Femoral Shaft Fractures: These occur along the long, central portion of the femur. They are typically the result of significant force, such as motor vehicle accidents or falls from height, and often involve substantial displacement and bleeding due to the surrounding musculature.
-
Distal Femur Fractures: These occur in the lower part of the femur, near the knee joint. They can involve the articular surface of the knee, making them complex and prone to causing long-term knee stiffness and arthritis if not treated meticulously. These fractures can be intra-articular (involving the joint surface) or extra-articular.
Mechanisms of Injury and Immediate Consequences
The mechanism by which a femur fracture occurs dictates the severity and pattern of the break.
High-Energy Trauma
In younger, healthier individuals, femur fractures are almost always the result of high-energy trauma. This includes:
- Motor Vehicle Accidents: Direct impact or severe forces can fracture the femur.
- Falls from Height: Significant impact forces from a fall can result in a break.
- Contact Sports: Direct blows or forceful twisting of the leg during sports like football or hockey can cause fractures.
These high-energy mechanisms often lead to complex, comminuted (multiple fragments), or open fractures, where the bone breaks through the skin, significantly increasing the risk of infection and requiring urgent surgical intervention.
Low-Energy Trauma and Osteoporosis
In older adults, particularly those with osteoporosis, a fracture can occur from a seemingly minor fall, such as tripping or slipping. The weakened bone cannot withstand the forces of even a simple fall, leading to a fracture, most commonly in the proximal femur.
Immediate Consequences of a Femur Fracture
Regardless of the mechanism, a broken femur elicits a cascade of immediate physiological responses:
- Severe Pain: The intense pain is usually localized to the fracture site and is exacerbated by any movement.
- Inability to Bear Weight: The structural integrity of the femur is compromised, making it impossible to stand or walk on the injured leg.
- Deformity: The limb may appear shorter or angled abnormally due to the displacement of bone fragments and the pull of surrounding muscles.
- Swelling and Bruising: Significant bleeding from the bone and surrounding tissues leads to rapid swelling and ecchymosis (bruising).
- Hemorrhage and Shock: Femur fractures, especially those of the shaft, can result in substantial internal bleeding. The loss of blood volume can lead to hypovolemic shock, characterized by a rapid heart rate, low blood pressure, and altered mental status. This makes immediate stabilization and fluid resuscitation critical.
- Nerve and Blood Vessel Injury: In severe fractures, sharp bone fragments can damage nearby nerves and blood vessels, potentially leading to numbness, tingling, loss of motor function, or compromised circulation to the lower leg and foot.
Diagnosis and Initial Management
Upon presentation to an emergency department with a suspected femur fracture, a thorough assessment is initiated.
Diagnostic Procedures
- Physical Examination: A physician will assess for pain, deformity, swelling, bruising, and any signs of neurovascular compromise. The patient’s ability to move the injured limb and bear weight will be evaluated.
- Imaging Studies:
- X-rays: Standard anteroposterior (AP) and lateral X-rays of the femur and surrounding joints are the primary diagnostic tools. These images clearly visualize the fracture, its location, displacement, and any associated injuries.
- CT Scan: In complex fractures, particularly those involving the knee joint or requiring surgical planning, a computed tomography (CT) scan may be used to obtain more detailed cross-sectional images of the bone.
- MRI: Magnetic resonance imaging (MRI) is less commonly used for initial fracture diagnosis but may be employed to assess for associated soft tissue injuries, such as ligament tears or cartilage damage, or to evaluate for potential avascular necrosis of the femoral head in proximal femur fractures.
Initial Management in the Emergency Department
The immediate goal is to stabilize the patient and prevent further injury:
- Pain Control: Intravenous pain medication is administered to alleviate the severe pain.
- Immobilization: The injured limb is carefully splinted to prevent movement of the fracture fragments. Traction may be applied to help align the bone and reduce muscle spasm.
- Fluid Resuscitation: For significant blood loss, intravenous fluids and potentially blood transfusions are administered to manage shock.
- Wound Care: If the fracture is open, the wound is thoroughly cleaned, and intravenous antibiotics are administered to prevent infection.
Surgical Treatment and Stabilization
Given the severity of femur fractures, surgical intervention is almost always necessary to restore alignment, promote healing, and enable early mobilization.
Surgical Approaches
The specific surgical technique depends on the location and type of fracture:
-
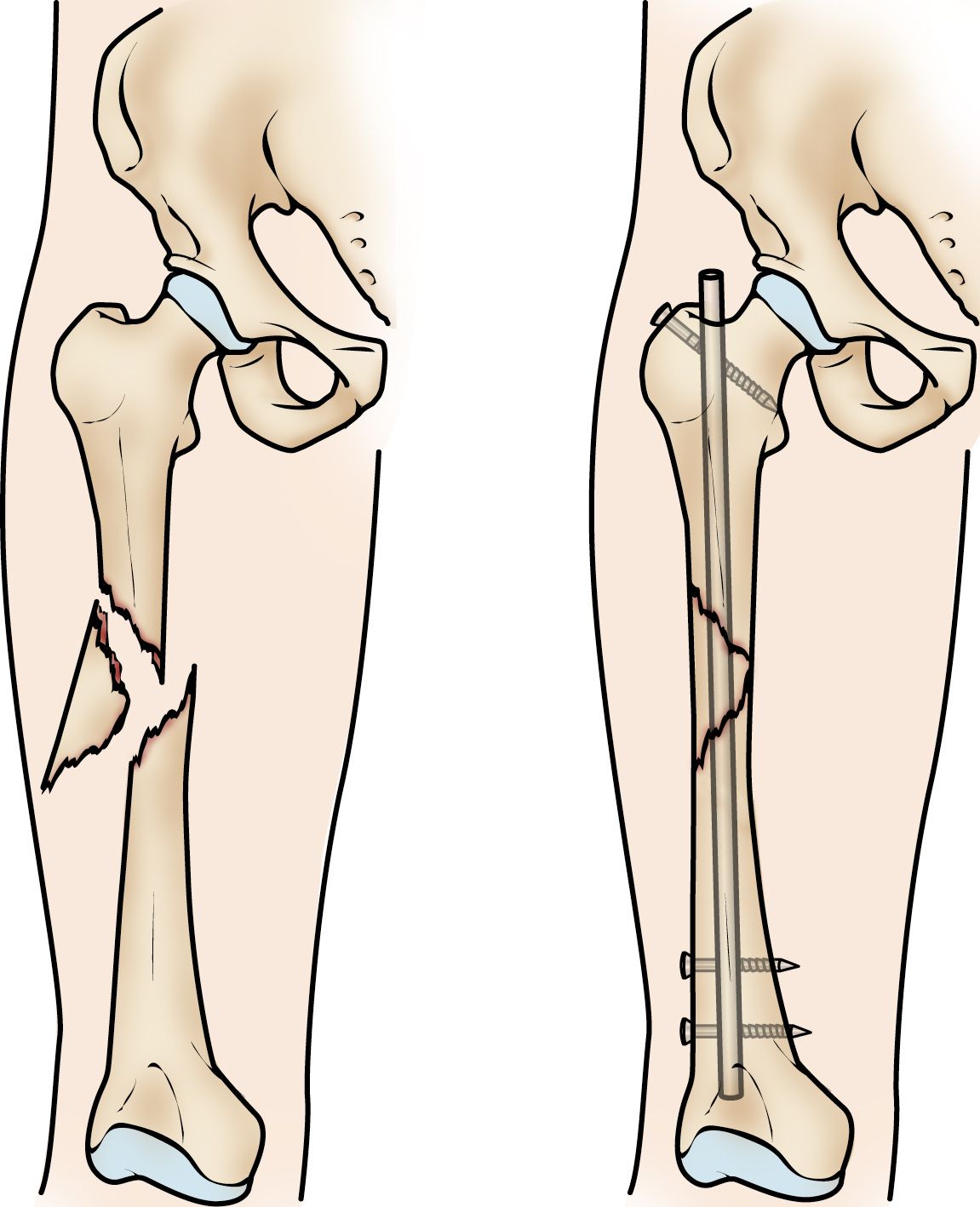
Intramedullary Nailing (IM Nailing): This is the gold standard for most femoral shaft fractures. A strong metal rod is inserted into the hollow medullary canal of the femur, extending from above the fracture to below it. The nail is then secured with screws at either end, providing stable fixation. This method allows for early weight-bearing as tolerated.
-
Plates and Screws: For proximal and distal femur fractures, especially those involving the joint surface, plates and screws are often used. These devices are attached to the outer surface of the bone, bridging the fracture site and holding the fragments together. Hip compression screws are commonly used for certain proximal femur fractures.
-
External Fixation: In cases of severe open fractures, significant soft tissue damage, or when immediate internal fixation is not feasible, an external fixator may be applied. This involves inserting pins through the skin into the bone on either side of the fracture, which are then connected by external bars. This provides temporary stability and allows for wound management before definitive internal fixation.
-
Total Hip Arthroplasty (THA) or Hemiarthroplasty: For severe, displaced proximal femur fractures, particularly in elderly or frail patients, replacing the hip joint with a prosthesis may be the most appropriate treatment to restore function and allow for early mobility.
Goals of Surgical Intervention
- Anatomical Reduction: Realigning the bone fragments as close to their original anatomical position as possible.
- Stable Fixation: Ensuring the fracture fragments are held securely in place to allow for bone healing without displacement.
- Early Mobilization: Facilitating prompt movement and weight-bearing to prevent complications such as muscle atrophy, joint stiffness, deep vein thrombosis (DVT), and pneumonia.
Rehabilitation and Recovery
The journey of recovery from a femur fracture is a marathon, not a sprint, and involves a multidisciplinary approach.
The Role of Physical Therapy
Physical therapy is an indispensable component of recovery. It begins in the hospital and continues long after discharge.
- Early Mobilization: Once cleared by the surgeon, patients will begin to move their hip and knee joints, often with the assistance of physical therapists and mobility aids like walkers or crutches.
- Range of Motion Exercises: Gentle exercises are crucial to prevent stiffness in the hip and knee joints.
- Strengthening Exercises: As healing progresses, progressively challenging exercises will be introduced to rebuild muscle strength in the quadriceps, hamstrings, gluteal muscles, and calf muscles.
- Gait Training: Patients learn to walk safely and efficiently, gradually progressing from using assistive devices to independent ambulation.
- Balance and Proprioception: Exercises to improve balance and the body’s awareness of its position in space are essential to prevent falls.
Potential Complications and Long-Term Outlook
Despite advancements in surgical techniques and rehabilitation, complications can arise:
- Infection: Especially in open fractures or with hardware placement, infection is a serious risk.
- Nonunion: The fracture fails to heal.
- Malunion: The fracture heals in an incorrect position, leading to deformity and functional impairment.
- Hardware Failure: The implants can loosen or break.
- Avascular Necrosis: The blood supply to the femoral head is disrupted, leading to bone death.
- Post-traumatic Arthritis: Damage to the joint surfaces during the fracture or subsequent joint stiffness can lead to the development of arthritis.
- Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE): Blood clots can form in the leg veins and travel to the lungs, a life-threatening condition.
- Chronic Pain: Persistent pain at the fracture site or in the surrounding joints.
- Muscle Atrophy and Weakness: Significant loss of muscle mass and strength.
- Joint Stiffness and Limited Range of Motion: Particularly in the knee and hip.
The long-term outlook for femur fracture recovery varies greatly depending on the fracture severity, the patient’s age and overall health, the effectiveness of surgical treatment, and the commitment to rehabilitation. With diligent adherence to therapy, most individuals can regain good function, though some may experience residual limitations. Full recovery can take anywhere from six months to over a year, requiring patience, perseverance, and a strong support system.